
Abstract
The gastrointestinal (GI) involvement, including acute pancreatitis (AP) from the novel coronavirus disease-2019 (COVID-19), is increasingly being reported. Recent evidence suggests that the pathogenesis of COVID-19 is mediated by the angiotensin-converting enzyme 2 (ACE-2) receptors and transmembrane protease serine 2 (TMPRSS2) for “priming,” which is highly expressed in the pancreas. To our knowledge, there is no other reported case of AP associated with COVID-19 after the respiratory symptoms are resolved. In this article, we present a patient with COVID-19, who came with intractable epigastric pain and resolved respiratory symptoms. A diagnosis of AP complicated with COVID-19 was made after laboratory and imaging workup, which was successfully managed conservatively.
Introduction
Patients with coronavirus disease-2019 (COVID-19) primarily present with respiratory symptoms like cough, fever, and dyspnea. 1 Recently, gastrointestinal (GI) manifestations such as abdominal pain, nausea, vomiting, and diarrhea are increasingly being reported in patients with severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection. 2 Although acute pancreatitis (AP) has well-established etiologies, the COVID-19 has been recognized as an emergent pathogen complicating AP. Most of the reported cases so far had mild pancreatic symptoms. 3 This case report highlights COVID-19 as a causality factor for AP in the absence of other known or identifiable risk factors.
Case Presentation
A 24-year-old Caucasian male presented with abdominal pain, nausea, vomiting, and 2 episodes of loose stools for 1 day. He had no significant past medical history except for a COVID-19 infection diagnosed 2 weeks ago, but his symptoms of cough and shortness of breath were resolved spontaneously. Initial vitals indicated blood pressure of 137/73 mm Hg, heart rate 83 beats/minute, temperature 97.9 °F, respiratory rate 18/minute, and arterial oxygen saturation 99% on room air. The physical examination was significant for epigastric pain and tenderness on deep palpation with no other findings.
On initial laboratory workup, lipase levels were 2025 units/L (reference range: 73-393 units/L), and a repeat COVID-19 by polymerase chain reaction (PCR) was positive. His urine drug screening was negative, blood alcohol levels were <3 mg/dL (reference range: ≤10 mg/dL), and triglyceride levels were 121 mg/dL (reference range: ≤150 mg/dL) on presentation. Additional laboratory data are summarized in Table 1. The differential diagnoses of AP ruled out in our patient are listed in Table 2.
Significant Laboratory Values at Days 1, 2, and 6.

Abbreviations: WBC, white blood cell; RBC, red blood cell; ALT, alanine aminotransferase; AST, aspartate transaminase.
Differential Diagnosis for Acute Pancreatitis in Our Patient.

Abbreviations: RUQ, right upper quadrant; COVID-19, coronavirus diseases-2019.
To rule out autoimmune pancreatitis.
The ultrasound of the abdomen was negative for gallstones or dilated common bile duct. A computed tomography (CT) scan of the abdomen and pelvis (A/P) with intravenous (IV) contrast was consistent with findings of moderately severe AP (Figure 1). The following day, the patient developed a fever of 100.5 °F, with a white blood cell (WBC) count of 12.7 k/µL and lipase levels of 4174 units/L. He was started on empirical piperacillin-tazobactam after the blood was drawn for cultures. The repeat contrast CT A/P showed increased fluid within the peripancreatic area compared with the prior study suggesting acute worsening (Figure 2). His symptoms improved on day 4, and oral intake gradually advanced to a low-fat diet. The antibiotics were discontinued after a negative blood culture report. His WBC count and lipase levels trended down to 9.3 K/µL and 301 units/L, respectively, and the patient was discharged on day 6 with instructions to return if he develops any fever or abdominal pain.

Contrast computed tomography scan of abdomen and pelvis showing a poor definition of fat planes surrounding the proximal to distal pancreatic body anteriorly but also posteriorly and frank fluid in retro gastric space (transverse view).

Contrast computed tomography scan of abdomen and pelvis showing increased fluid within the lesser sac and peripancreatic location (transverse view).
Discussion
Patients with COVID-19 presents classically with respiratory symptoms. 1 Lately, the evidence has shown the increasing presentation with GI symptoms such as diarrhea (13%), nausea/vomiting (10%), and abdominal pain (9%). 2 The most common viral affiliation of AP in comparison to COVID-19 is well reported in the literature and summarized in Table 3.4,5 However, COVID-19 has been reported as an emerging pathogen complicating AP. A study of 52 COVID-19 pneumonia patients depicted mild pancreatic injury in 17% of cases. 3 The pathogenesis in the GI tract is believed to be mediated through angiotensin-converting enzymes 2 (ACE-2) receptors and transmembrane protease serine 2 (TMPRSS2) for “priming,” which are abundantly expressed in GI epithelial cells, including pancreatic islets cells. The interaction of viral spike (S) proteins with ACE-2 receptors on target organs results in the endocytosis of the virus. Subsequently, the viral RNA and proteins are synthesized and assembled into new virions, which release the cytokines causing GI symptoms. The virus can also cause diffuse severe endotheliitis of submucosal vessels in several anatomical sites leading to diffuse microischemic disease that can subsequently result in AP.6,7 A literature review unveiled the GI tract as a site of asymptomatic viral shedding and a potential source of fecal-oral transmission. 8 Studies have shown that the time from onset of GI symptoms to hospital presentation is 9 days versus 7.3 days for respiratory symptoms. 9 The diagnostic criteria for AP per revised Atlanta classification included the presence of 2 out of the following 3 criteria: (1) abdominal pain (primarily sharp, epigastric, and radiating to the back); (2) elevated serum lipase or amylase more than 3 times the upper limit of the standard value; (3) characteristic imaging findings evident for AP. 10 Our patient met all the criteria mentioned above with no other source of AP except COVID-19. Most cases reported so far have concurrent respiratory system involvement. 9 On the contrary, our patient presented after the resolution of respiratory symptoms. The conservative management is only the mainstay in AP complicated with COVID-19. 11 Nevertheless, the diagnosis of COVID-19 and AP clinical symptoms in the absence of classical etiological factors suggests a strong correlation.
Common Viral Etiologies Complicating Acute Pancreatitis as Compared With SARS-CoV-2.
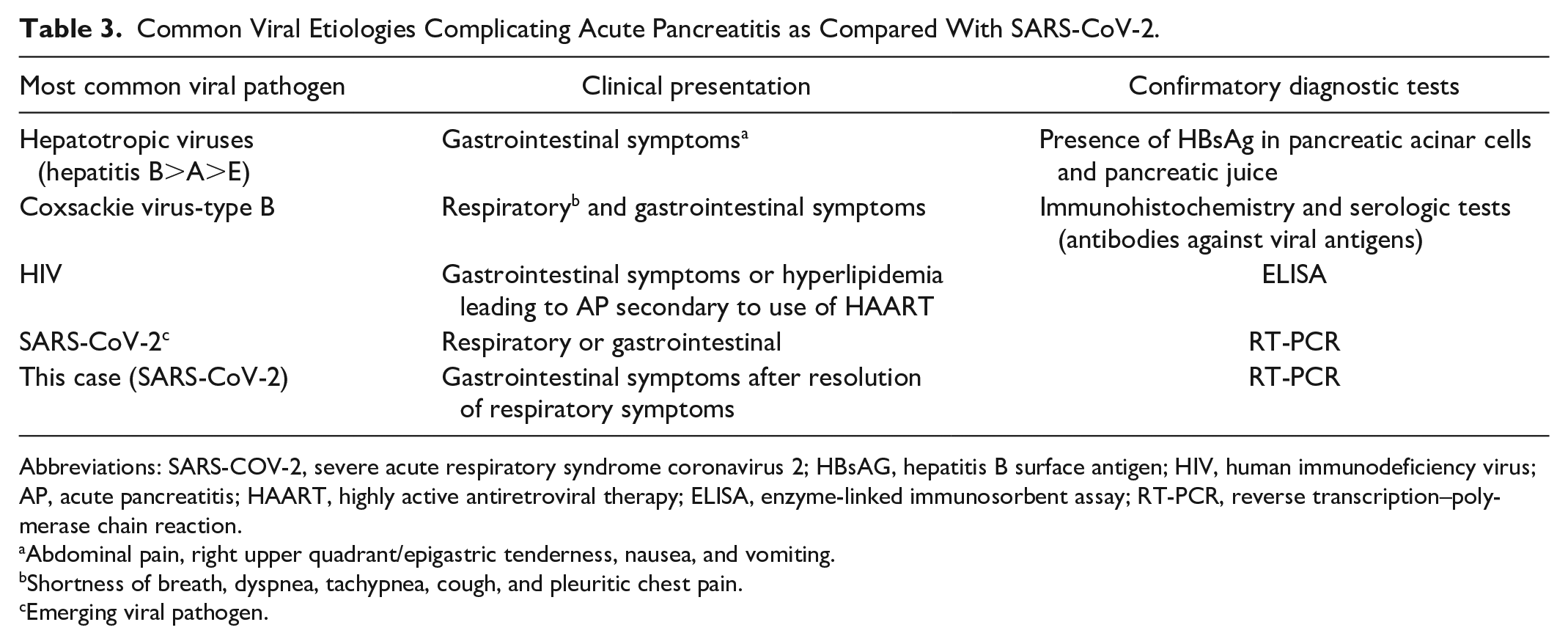
Abbreviations: SARS-COV-2, severe acute respiratory syndrome coronavirus 2; HBsAG, hepatitis B surface antigen; HIV, human immunodeficiency virus; AP, acute pancreatitis; HAART, highly active antiretroviral therapy; ELISA, enzyme-linked immunosorbent assay; RT-PCR, reverse transcription–polymerase chain reaction.
Abdominal pain, right upper quadrant/epigastric tenderness, nausea, and vomiting.
Shortness of breath, dyspnea, tachypnea, cough, and pleuritic chest pain.
Emerging viral pathogen.
Conclusions
A high index of suspicion should be maintained in patients with COVID-19 presenting with GI symptoms after the resolution of respiratory symptoms. Physicians should be cognizant regarding the differential of AP in such patients as a timely diagnosis can prevent future morbidity and mortality.
Footnotes
Author Contributions
Hafiz Muhammad Abrar Jeelani: Conception of the idea, Acquisition of data, manuscript writing, and final approval.
Muhammad Mubbashir Sheikh: Critical revision, manuscript writing, and final approval.
Shirly Susan Samuel: Critical revision, acquisition of data, conception of idea, and final approval.
Yetunde Bernice Omotosho: Critical revision, conception of idea, and final approval.
Artem Sharko: Acquisition of data, critical revision, conception of idea, and final approval.
Rami Albetar: Acquisition of data, conception of idea, critical revision, and final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Institutional review board approval is not required for case reports at the institution where this patient was treated.
Informed Consent
Published with the consent of the patient.