
Abstract
Background:
Dropped head syndrome (DHS) can be divided into two types, the positive sagittal vertical axis (SVA) type and the negative SVA type. However, the cervical sagittal alignment of DHS including global sagittal spinal alignment and the typical cervical alignment of the types of DHS is still unclear. The purpose of this study was to clarify the character of cervical sagittal alignment of DHS and analyze the relationship between cervical sagittal alignment and global sagittal spinal alignment.
Methods:
The subjects were 35 DHS patients (10 men, 25 women, mean 71.1 years old). They were divided into two groups: negative DHS (N-DHS group, SVA < 0 mm) and positive DHS group (P-DHS group, SVA ≥ 0 mm). As control, 28 age-matched cervical spondylosis patients (CS, 21 men, 7 women, mean 67.4 years old) were analyzed. The following parameters were measured on lateral global-spine standing radiographs: cervical SVA (C2-C7SVA), O-C2A (O-C2 angle), C2 slope (C2S), C2-7A (C2-7 angle), T1 slope (T1S) and C7SVA.
Results:
The results of measurements of each of the averaged sagittal alignment parameters were (CS, P-DHS, N-DHS): C2-7SVA(26.2 mm, 47.3 mm, 44.5 mm), O-C2 angle (35.0°, 37.1°, 39.3°), C2S (16.5°, 31.4°, 33.8°), C2-7A (9.3°, 9.9°, −16.6°), T1S (22.9°, 39.7°, 25.7°), C7SVA (35.3 mm, 51.0 mm, −43.1 mm). C2-C7SVA and C2S were significantly larger in both types of DHS compared to CS. Comparing P-DHS with N-DHS, C2-C7A and T1S were significantly smaller in N-DHS.
Conclusions:
O-C2A did not differ significantly among CS, P-DHS and N-DHS. In DHS patients, C2-7SVA and C2S were significantly larger than those of CS regardless of the type of DHS. The typical cervical sagittal alignment of DHS was different between P-DHS and N-DHS. In P-DHS, C2-7A and T1S were larger than those in N-DHS and the imbalance of thoraco-lumbar alignment should be noted.
Introduction
Dropped head syndrome (DHS) is associated with severe cervical extensor muscle weakness resulting in head over-flexion, a so-called chin-on-chest deformity in the standing or sitting upright position. 1 Such patients present with cervical pain and the inability to maintain a horizontal gaze. Some patients complain of difficulty in eating because the cervical mal-alignment makes it difficult to swallow food. 1 The typical characteristic of DHS is the cervical deformity, which can be corrected by passive cervical extension in the early stage 1 ; patients do not have severe cervical kyphosis in the neutral position despite the presence of dropped head in the cervical flexion position. In contrast, cervical kyphosis due to spondylotic change is usually rigid and uncorrectable by passive cervical extension, together with decreased cervical range of motion (ROM). 2 The term isolated cervical extensor myopathy (INEM) has been proposed to categorize patients with cervical extensor muscle weakness without neuromuscular or structural disorders. 3 As the proportion of elderly persons has increased, the number of patients with DHS due to cervical degenerative change is also expected to increase. 4 Previously DHS was simply described as a chin-on-chest deformity due to cervicothoracic extensor weakness without detailed structural analysis including global spinal alignment, 1,3,5 –7 and little is known about the characteristics of cervical sagittal alignment of DHS in relation to global sagittal spinal alignment.
A recent study reported that DHS can be divided into two types based on sagittal balance, the positive sagittal vertical axis (SVA) type and the negative SVA type. 8 Because the global sagittal spinal alignment is known to affect cervical alignment, 9,10 it can be expected that there will be differences in cervical sagittal alignment between the two types of DHS. 11,12 However, there are only a few studies regarding the cervical sagittal alignment of DHS while taking into consideration global sagittal spinal alignment, and thus the differences in cervical alignment between the types of DHS are still largely unclear. 8,13 The main reasons are that DHS without neuromuscular disorder is a relatively rare disease, 1 and DHS had been analyzed at only the cervical spine locally. 8 In a recent study, Kudo et al. analyzed the poor surgical outcome of DHS and proposed consideration of the global spinopelvic sagittal alignment parameters. 14
The purpose of the present study was to analyze the cervical sagittal alignment of DHS from the point of view of global sagittal spinal alignment.
Subjects and methods
This research was a retrospective study of 35 consecutive DHS patients (DHS group: 10 men and 25 women; mean age 71.1 ± 8.5 years) who presented with correctable chin-on-chest deformity clinically, and 28 age-matched degenerative cervical disease patients (age range 65–85 years) who visited our facility between 2016 and 2019 with a diagnosis of cervical spondylosis (CS) without severe cervical spine deformity (CS group: 21 men and 7 women; mean age 67.4 ± 8.0 years). DHS was defined as follows: (1) the patient could not maintain a neutral cervical position even for only a few seconds, gradually showing a chin-on-chest position, (2) cervical deformity was correctable in supine position. The corrective alignment of the dropped head was examined by cervical computed tomography (CT) in the supine position. Patients with posterior longitudinal ligament ossification, neuromuscular disease, coronal deformity > Cobb 30°, or a history of previous spinal operation, and those unable to maintain an upright position without assistance were excluded.
Whole spine anteroposterior and lateral radiographs were obtained by digital slot-scanning radiography (DSSR) mode with the Sonialvision Safire fluoroscopy system (Shimadzu Corp., Kyoto, Japan) in the most stable and relaxed standing position with possible knee extension while maintaining a horizontal gaze in the fists-on-clavicle posture to ensure reasonable reproducibility. 15 The following parameters were measured: total distance from the plumb line of the pedicle center of the C2 vertebra to the posterior superior corner of the C7 vertebra (C2-7 sagittal vertical axis; C2-7SVA), the angle between the McGregor line and the inferior surface of the axis (O-C2 angle; O-C2A), the angle between the C2 lower endplate and the horizontal plane (C2 slope; C2S), the angle from the lower endplate of C2 to the upper endplate of C7 (C2-7 angle; C2-7A), the angle between the T1 upper endplate and the horizontal plane (T1 slope; T1S), and the distance from the C7 plumb line to the sacral posterior angle (C7SVA). The inter-agreement rates of the measurements for C2-7SVA, C2-7A, and C7SVA were satisfactory in the CS and DHS groups (Tables 1 and 2). 16 According to a previous classification 11 of cervical alignment by C7SVA, the DHS group was divided into two groups of negative DHS (N-DHS group, SVA < 0 mm) and positive DHS group (P-DHS group, SVA ≥ 0 mm). All subjects provided informed consent after receiving an explanation of the study protocol. This study was approved by the Institutional Review Board of our university. Values were presented as mean ± standard deviation (SD). JMP software package version 10.0 (SAS Institute Inc., Cary, NC, USA) was used for statistical analysis. The Shapiro-Wilk test was used for goodness-of-fit of normal distribution. The Wilcoxon-Mann-Whitney test was used for pairwise comparisons, and one-way ANOVA and the Steel-Dwass test were used for comparisons among the three sets of data. The Chi-square test was used for categorical variables. A p-value of < 0.05 was considered to indicate statistically significant difference.
Comparison of demographic data among CS, P-DHS, and N-DHS.
CS: cervical spondylosis; P-DHS: positive SVA DHS; N-DHS: negative SVA DHS.
a CS vs P-DHS.
b CS vs N-DHS.
cP-DHS vs N-DHS.
Comparison of spinal parameters among CS, P-DHS, and N-DHS.

CS: cervical spondylosis; P-DHS: positive SVA DHS; N-DHS: negative SVA DHS; C7SVA: C7 sagittal vertical axis; C2-7SVA: C2-7 sagittal vertical axis; O-C2A: O-C2 angle; C2S: C2 slope; C2-7A: C2-7 angle; T1S: T1 slope.
a CS vs P-DHS.
b CS vs N-DHS.
cP-DHS vs N-DHS.
Results
Females were in much greater majority in N-DHS than in P-DHS (Table 1). The results of measurements of each of the averaged sagittal alignment parameters (CS, P-DHS, N-DHS) were: C2-7SVA (26.2 mm, 47.3 mm, 44.5 mm), O-C2A (35.0°, 37.1°, 39.3°), C2S (16.5°, 31.4°, 33.8°), C2-7A (9.3°, 9.9°, −16.6°), T1S (22.9°, 39.7°, 25.7°), C7SVA (35.3 mm, 51.0 mm, −43.1 mm) (Table 2). O-C2A was not significantly different among CS, P-DHS and N-DHS. C2-7SVA and C2S were significantly larger in both P-DHS and N-DHS than CS. The C2-7A of N-DHS was significantly smaller than that of P-DHS and CS. T1S of P-DHS was significantly larger than that of N-DHS and CS (Table 2 and Figures 1 and 2).
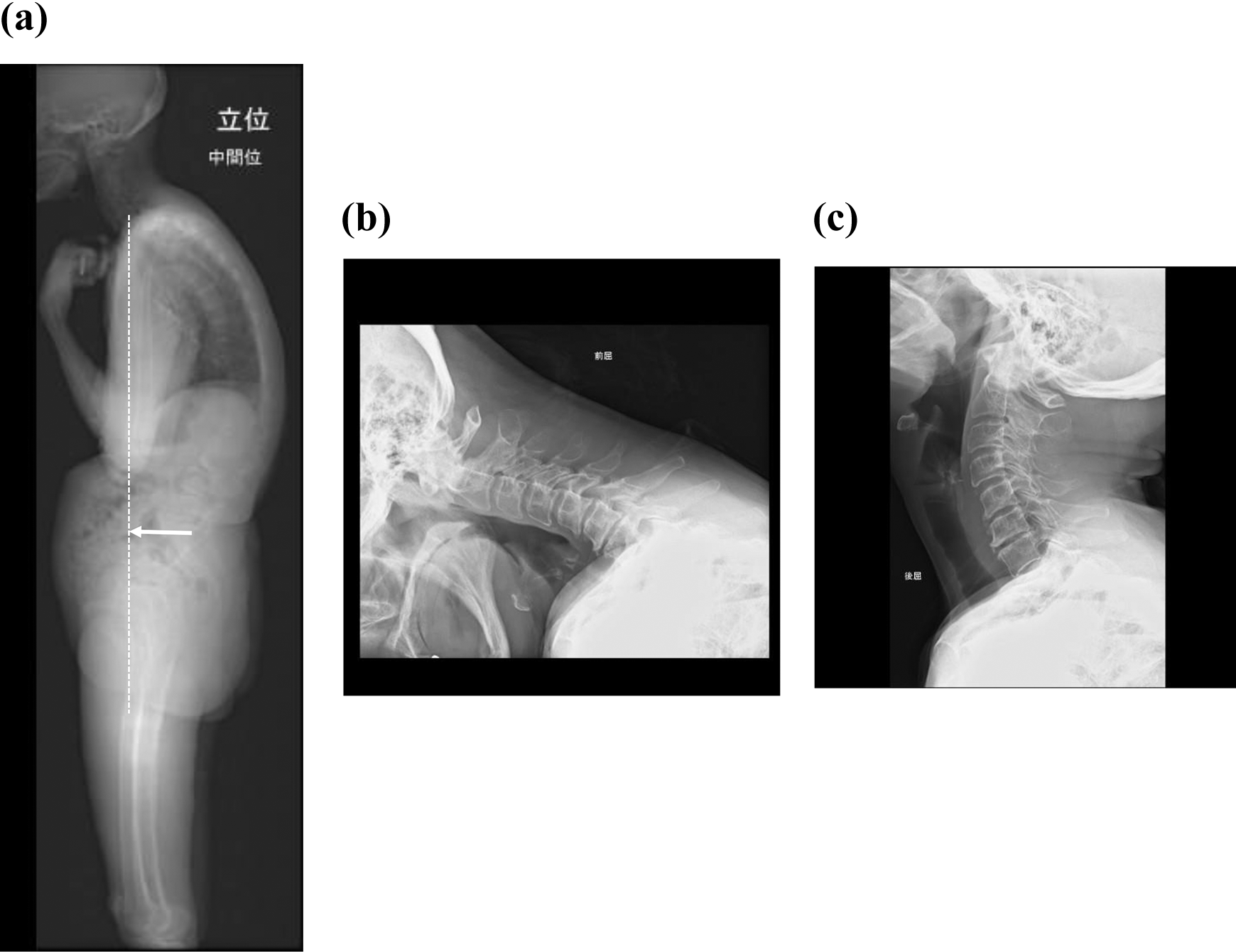
Representative cases of P-DHS. (a) Global sagittal spine X-ray findings in neutral position. C2-7SVA: 34.0 mm, C7SVA: 84.0 mm, O-C2 angle: 33°, C2 slope: 43°, C2-7 angle: 23°, T1 slope: 40°. White dotted line indicates C7 plumb line. (b) Cervical lateral X-ray image in flexion. (c) Cervical lateral X-ray image in extension. P-DHS: positive SVA DHS; SVA: sagittal vertical axis.
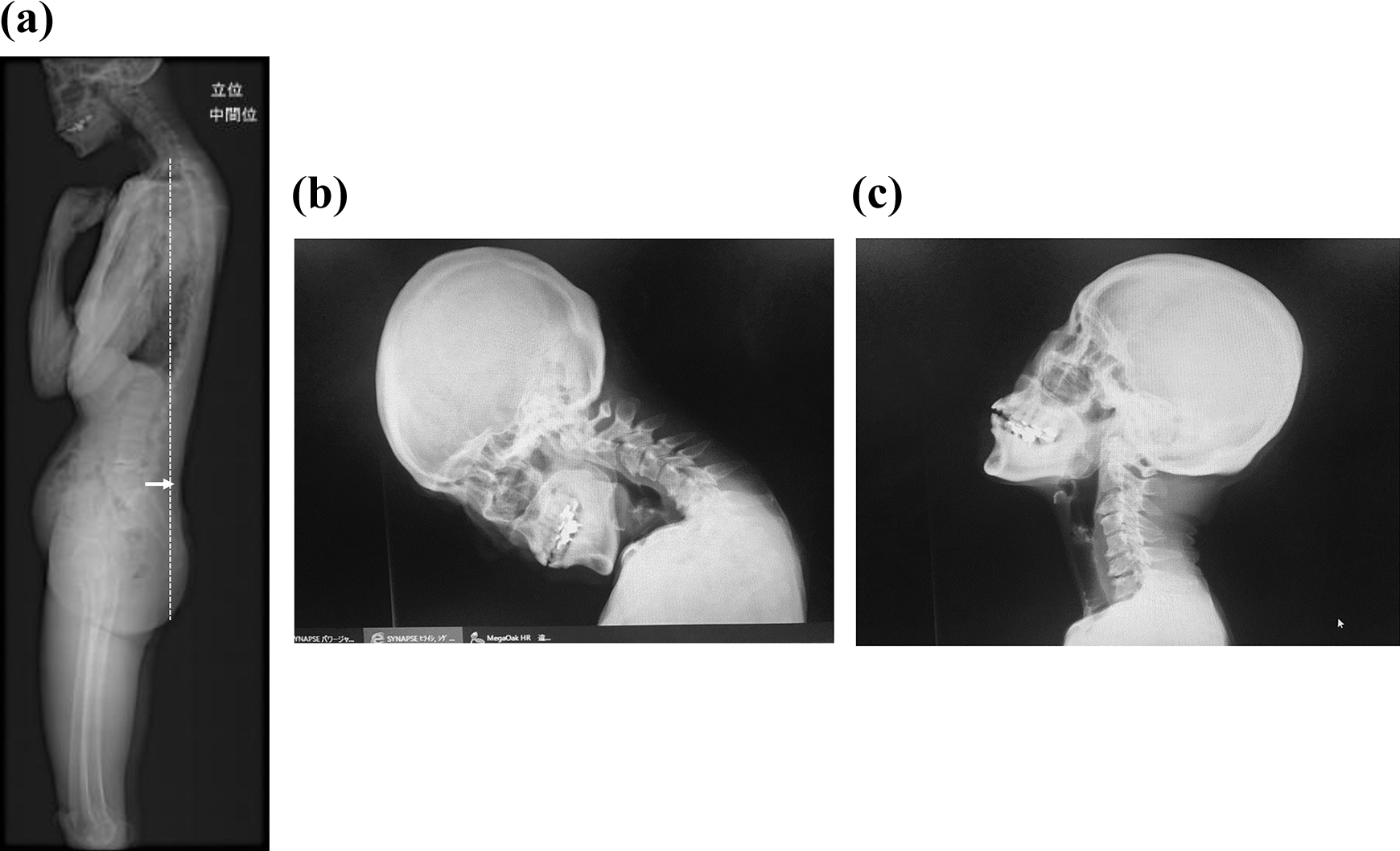
Representative cases of N-DHS. (a) Global sagittal spine X-ray findings in neutral position. C2-7SVA: 50.5 mm, C7SVA: −31.4 mm, O-C2 angle: 42°, C2 slope: 55°, C2-7 angle: −36°, T1 slope: 22°. White dotted line indicates C7 plumb line. (b) Cervical lateral X-ray image in flexion. (c) Cervical lateral X-ray image in extension. N-DHS: negative SVA DHS; SVA: sagittal vertical axis.
Discussion
The present study demonstrated that O-C2A did not differ significantly among CS, P-DHS and N-DHS. Large C2S and C2-7 SVA were common characteristics in DHS, but T1S and C2-7A were different between P- and N-DHS.
O-C2A was maintained in DHS in both P- and N-DHS. Large C2S represented forward rotated head position. Large C2-7 SVA indicated enlarged horizontal distance between the plumb line of C2 and the vertebral body of C7, suggesting cervical imbalance. 17 A value of C2-7 SVA ≥ 40 mm is the threshold for cervical imbalance presenting with severe symptoms, and a low health-related quality of life. 10 Large C2-7 SVA induced the increase of cervical extensor lord by head gravity, because every inch of forward head posture can increase the weight of the head on the spine by an additional 10 pound. 1 The dropped head phenomenon in DHS could be thought to have resulted from prolonged C2-7 SVA and the consequential extensor muscle fatigue.
Kusakabe et al. reported that acute-onset DHS without a history of cervical trauma has a better prognosis by conservative treatment, and that surgical indications for DHS should be carefully determined. 18 Our previous data demonstrated a recovery rate of DHS of about 20%, with no significant difference between P- and N-DHS. 4
Regarding surgery for DHS, Kudo et al. reported that pre- and postoperative SVA and PI (pelvic incidence)-LL (lumbar lordosis) were associated with surgical outcomes of patients with DHS. 14 The present study could not analyze operative results because of the inclusion of many non-operative cases. However, our results showed that P-DHS represented low C2-C7A and T1 due to loss of thoraco-lumbar compensation, and also that there was a difference between P- and N-DHS concerning the sagittal spinal compensation mechanism. 8 Those results supported the importance of assessing the pre-operative SVA. The cause of P-DHS is a kyphotic spinal deformity and positive imbalance due to osteoporotic vertebral fracture and/or lumbar degenerative change. The differences of global alignment would affect the decision governing the operative method.
The occipito-cervical junction is also an important issue. The present results indicated that O-C2A did not differ significantly among CS, P-DHS and N-DHS. A previous study supported our results that large C2-7 SVA cases represent a small C7-T1 lordotic angle but O-C2A in comparison with age-matched control. 19 Konishi et al. also reported that C2-7A in DHS was not correlated with T1S, but with O-C2A. 20 Regarding the cervicothoracic junction, Murata et al. mentioned that relative risk factors in the occurrence of cervical positive imbalance of DHS were high in C2S, T1S and T1-T4 angle. 13 In DHS, while the occipito-cervical function could be preserved, the extensor disfunction of the cervicothoracic junction would be essential pathology. Therefore, when planning the rostral end of cervical surgery for DHS, cervicothoracic fixation must be included and O-C2 could be avoided regardless of the type of DHS. In N-DHS cases, correction surgery for cervical kyphosis would be needed and the length of spinal fixation would be successful between C2 and T4, as compensation in the thoracic and lumbar spine was still insufficient. However, in P-DHS cases, correction surgery for dropped head has to include consideration of the thoraco-lumbar spine. In fact, we experienced a case of P-DHS with a complaint of horizontal gaze disturbance that could be cured simply by correcting the thoraco-lumbar spinal mal-alignment without cervical surgery. 21
This study had the following limitations. The number of subjects was relative small, reflecting the small number of DHS patients in general, 1 and this study did not include cervical alignment in cervical flexion because the characteristics of the neutral position are more common in the general understanding of DHS. Despite these limitations, we consider that this study could at least highlight the common cervical sagittal alignment in DHS compared to age-matched cervical spondylosis.
Conclusions
O-C2A did not differ significantly among CS, P-DHS and N-DHS. In DHS patients, C2-7SVA and C2S were significantly larger than those of CS regardless of the type of DHS. The typical cervical sagittal alignment of DHS differed between P-DHS and N-DHS. In P-DHS, C2-7A and T1S were larger than those in N-DHS, and the imbalance of thoraco-lumbar alignment should be noticed.
Footnotes
Acknowledgement
We are indebted to Mr Arndt Gerz for editorial review of the English manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.