
Abstract
Study Design
Biomechanical modeling study.
Objectives
Despite several recognized risk factors for proximal junctional kyphosis (PJK), its causative mechanism remains unknown. There are limited biomechanical studies to elucidate the association of sagittal alignment with PJK. Our aim is to determine the association of adjacent forces with PJK development.
Methods
ASD patients operated on with posterior fusion from T9-T11 to the pelvis and had 2 year follow-up were included in this retrospective study. Patient-specific musculoskeletal models were created from EOS images. High vs low normalized vertebral forces were defined based on a threshold of 0.2 for shear and 0.5 for compression. The load ratio was defined as the ratio of immediate postoperative to preoperative vertebral forces.
Results
A total of 35 patients (19 PJK, 16 Non-PJK) were included. PJK patients had statistically significant global malalignment with respect to global tilt (GT), T1 pelvic angle (TPA) and C2-UIV+1PA. A high-risk zone for the development of PJK is defined as high normalized shear and/or compression with a high load ratio. While none of the non-PJK patients were in the high-risk zone, 5 PJK patients were not in that zone, suggesting factors other than alignment may have contributed to this adverse event. Despite low shear for 3 of these non-PJK patients, they experienced high shear ratio.
Conclusions
The proposed thresholds were accurate in 86% of patients who developed PJK. These findings suggest postoperative shear at UIV+1 as an important risk factor for PJK. Keeping shear force low in alignment will help surgeons reduce PJK development.
Keywords
Introduction
Proximal junctional kyphosis (PJK) is an increasingly recognized postoperative complication of spine surgery and occurs in 20 to 40% of patients who undergo spinal deformity corrective fusion surgery.1,2 More than twenty risk factors have been identified that predispose patients to PJK,3,4 which can be categorized into surgical, patient and alignment variables. Surgical variables include pseudarthrosis or loss of proximal fixation, approach type (anterior vs posterior approach), the level of the upper instrumented vertebra (UIV) and lower instrumented vertebra (LIV), number of instrumented levels5,6 and the type of instrumentation (rod bending, screws, hooks, interbody cages). 7 Patient characteristics include age, sex, body mass index (BMI) and bone mineral density (BMD).4,8 Alignment variables include pre and postoperative radiographic parameters (eg, thoracic kyphosis (TK), lumbar lordosis (LL), sagittal vertical axis (SVA), pelvic incidence (PI), pelvic tilt (PT), and sacral slope (SS)). 9 Recently, a scoring system based on some of these identified risk factors was proposed to predict the risk of PJK preoperatively. 10 However, there are some limitations for existing risk factors and scoring systems. Most PJK risk factors such as age, BMD, and the number of fusion levels, are not modifiable or are difficult to alter through clinical interventions. Additionally, another limitation is the complexity and variability in how these factors interact with 1 another. For instance, while factors such as spinal alignment, fusion technique, and instrumentation type are considered important, their individual contributions to PJK risk can vary significantly between patients. Furthermore, patient-specific factors like muscle strength, soft tissue condition, and pre-existing spinal deformities are often not well-represented or quantified in existing risk models, yet they may play significant roles in the development of PJK. Despite the existence of these various risk factors,11-14 the perioperative prediction of PJK development is yet to be investigated.
Invasiveness of acquiring vertebral loading and unfeasibility of assessing its correlation to spinopelvic parameters have turned inverse dynamic-based musculoskeletal modeling into an efficient approach. Various musculoskeletal models have been proposed15-20 to determine vertebral loading affected by weight and height, spinopelvic alignment, and trunk muscle morphology.21-26 Changes in global sagittal alignment, lumbar typology, and sacral inclination have been shown to affect lumbar intervertebral forces, muscle activation and clinical outcome.27,28 Investigation of the correlation between intervertebral forces and pelvic incidence-lumbar lordosis mismatch introduced high shear force as a risk factor for adjacent segment disease in patients with lumbar fusion. 29 Association between sagittal alignment and vertebral loading at the adjacent segment in the fused spine was studied using musculoskeletal analysis of 205 patients with adult spine deformity (ASD). It was concluded that sagittal malalignment identified by Global alignment and proportion (GAP) score and pre-to-post-operative changes in GAP, global tilt (GT), LL and UIV slope were associated with changes in the adjacent forces. 30
We hypothesized that excessive postoperative vertebral loading at the proximal non-instrumented segment (adjacent force) is associated with PJK development. It is also hypothesized that the vertebral tolerance postoperatively can be estimated based on the preoperative forces. The purpose of this study was to determine if development of PJK can be predicted based upon immediate postoperative alignment utilizing a biomechanical approach to calculate vertebral loading. The proposed mathematical technique to simulate a pre-planned alignment not only fulfills the advantages of previous methods, 31 but also provides the opportunity to construct a simulated pre-planning sagittal alignment based on desired radiographic parameters. Utilizing this biomechanical approach may enable more effective preoperative planning to reduce excessive vertebral loading and lessen the risk of PJK development.
Materials and Methods
Subjects
A convenience sampling of thirty-five ASD patients [average age 65.8 (SD 11.4 yrs.), 24 females (68%)] operated on with a posterior fusion from lower thoracic (T9-T11) to the pelvis who had 2-year follow up were included in this retrospective, single center study. Study approval was obtained from the Institutional Review Board (IRB No. 21-5873). Exclusion criteria consisted of patients with spinal deformities derived from ankylosing spondylitis, neuromuscular diseases, fracture, infections, or Scheuermann kyphosis. The images of the thoracolumbar spine were acquired in coronal and sagittal planes using EOS imaging system (EOS Imaging, Paris, France) pre- and immediately post operation.
Patients were stratified into 2 groups based on the incidence of PJK at their last follow-up: PJK group and non-PJK group. PJK was defined when the postoperative Cobb angle between lower endplate of the UIV and the upper endplate of the 2 supra-adjacent vertebrae (UIV+2) is 10° higher than preoperative. 32
Musculoskeletal Model
We used an OpenSim full body musculoskeletal model including a fully articulated thoracolumbar spine.16,18,33 OpenSim is an open-source software platform for musculoskeletal modeling, simulation, and analysis. It integrates multibody dynamics to simulate the interaction of different parts of the body such as muscles, bones, and joints (as rigid bodies) under forces. The patient-specific musculoskeletal (MSK) models were created based on a generic sex-specific model of the spine and then these base models were scaled using patients’ measured heights, weights, and spinal curvatures. Based on the spine curvatures extracted from pre and immediate postoperative standing EOS images, 2 models were built for each patient. The location and orientation of each vertebra was obtained with a custom MATLAB script through the procedure briefly explained in Section 2.3. The simulations under upright standing posture were carried out in OpenSim software. Models were solved using static optimization based on inverse dynamics, with a cost function that minimized the total sum of squared muscle activation. 34 Individual muscle forces were calculated for upright standing posture. After prediction of muscle forces, intervertebral joints loading including compressive and shear forces were computed using joint reaction analysis. Both weight and spinal curvature contribute to vertebral forces. To isolate the effect of spinal alignment, vertebral forces were normalized by body weight, which make it easier to observe how changes in alignment impact the loading on individual vertebrae.
3D Reconstruction of Sagittal Alignment
To obtain vertebral and intervertebral location and orientation from bi-planar EOS images, a custom MATLAB script (MathWorks Inc, Natick, MA, USA) was developed. The location and orientation of each vertebra was identified using a set of anatomical landmarks. Following local coordinate systems determination, the relative rotation of each vertebra with respect to its parent was described by Euler angles as the successive x-y-z rotations of the local coordinate system with respect to its parent’s local coordinate system. In addition, the relative translations of intervertebral joints were calculated, and along with orientations were employed in the OpenSim model.
Construction of Simulated Mathematical Models
To construct alignment using EOS images or based on targeted sagittal radiographic parameters, a mathematical model was proposed. This tool will help simulate pre-planning alignments based on various realignment criteria or desired spinopelvic parameters. In the first step, a Bezier curve was fitted to IVD points collected from the preoperative EOS image. The relative distance of vertebral bodies was stored in the simulated alignment. Then, an optimization procedure was employed to modify Bezier control points to achieve targeted radiographic parameters including segmental, regional, or global sagittal alignments. The procedure also was implemented on actual pre- and postoperative alignments to achieve smooth models. To determine the control points of Bezier that best fits inside the vertebral points, an optimization algorithm was exploited. The optimization parameters were Bezier control points, and the cost function was the sum of squares of the minimum distances between each IVD point to the Bezier curve. To determine the minimum distance between each IVD point and the Bezier curve, another optimization was used. In the latter optimization algorithm, the optimization parameter was the curve parameter t, and the cost function was the distance between the point and the curve. This optimization was run for every IVD point and the obtained distances were used to construct the former optimization cost function. Figure 1 illustrates coronal and sagittal views of EOS images, as well as a Bezier curve fitted to intervertebral discs’ centers and its corresponding musculoskeletal model. For the sake of simplicity to illustrate sagittal alignment, the musculoskeletal model was represented without muscles, ribs, upper extremities, and the pelvis. Creating musculoskeletal model from an EOS image: (A) coronal view, (B) sagittal view of EOS image, (C) a Bezier curve fitted to intervertebral discs’ centers, (D) OpenSim musculoskeletal model represented without muscles, ribs, upper extremities, and pelvis.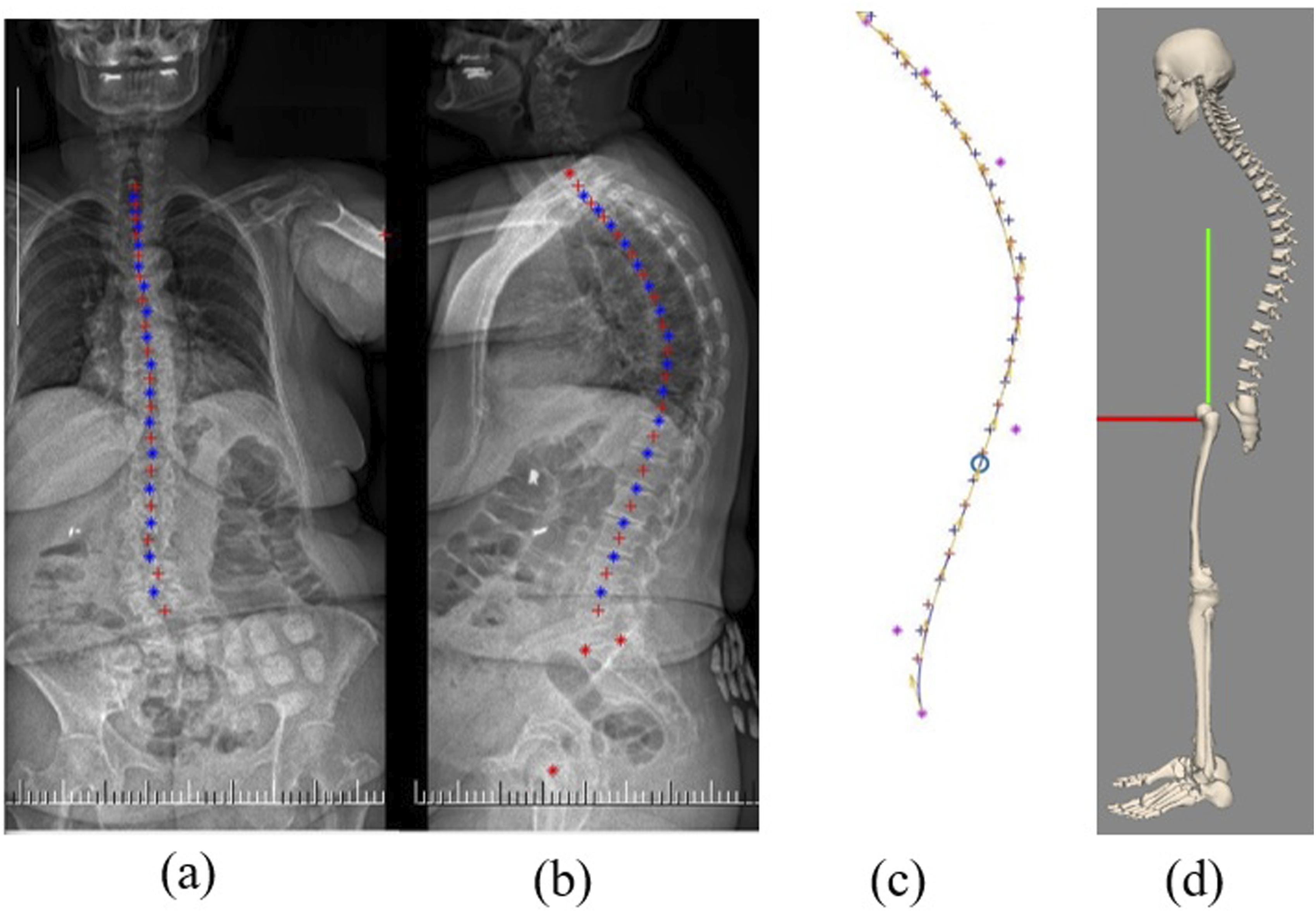
Statistical Analysis
Demographic and spinopelvic parameters were compared between 2 groups of PJK and non-PJK. Statistical analyses were completed utilizing an independent 2-sided t test with the level of significance set to 0.05. Continuous variables were expressed as means ± standard deviations to determine the difference between the PJK and non-PJK groups.
Results
Demographic Data of Patients in PJK and Non-PJK Groups.

Sagittal Radiographic Parameters
Comparison of Pre- and Postoperative Sagittal Radiographic Parameters Between PJK and Non-PJK Groups.
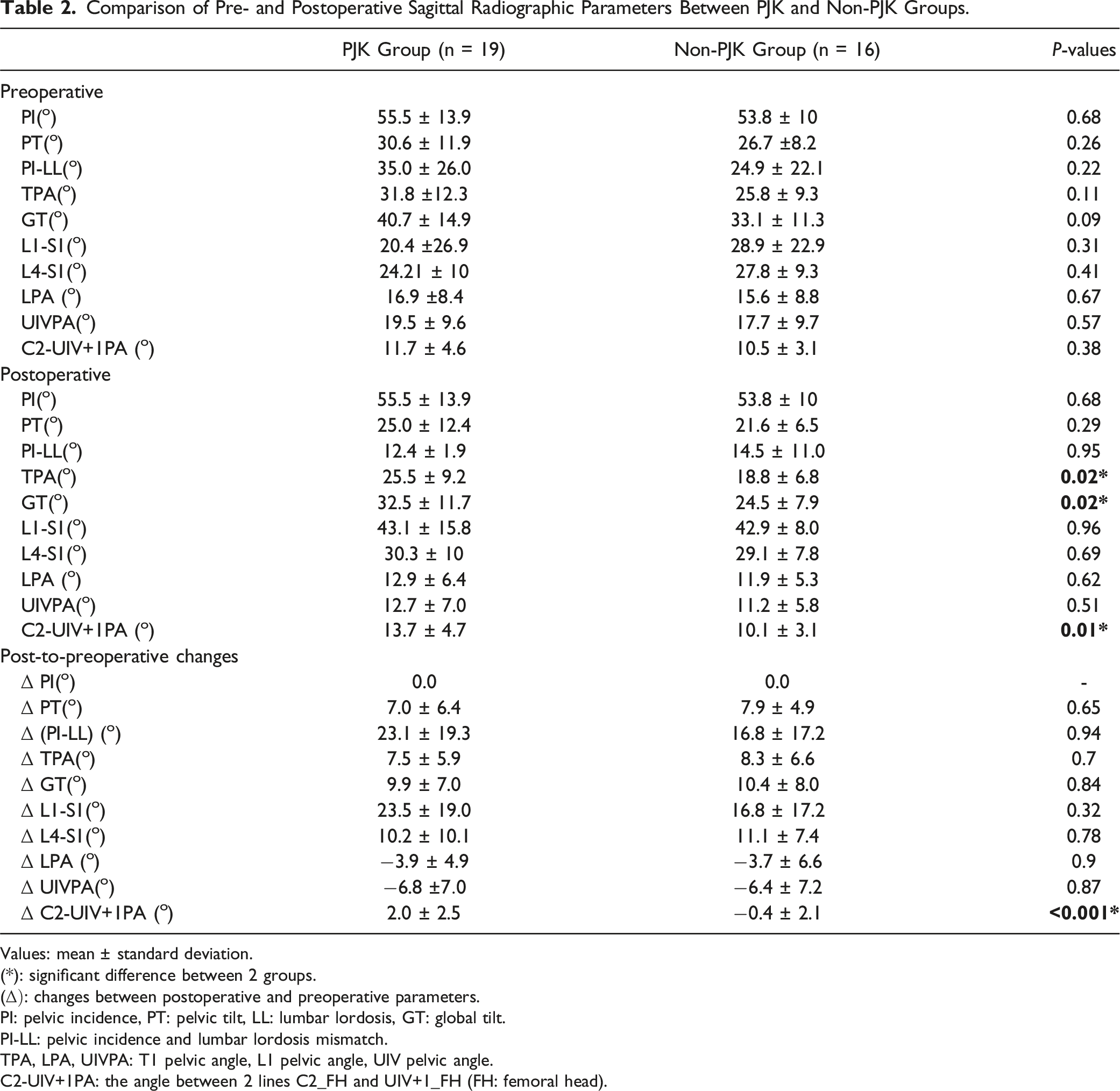
Values: mean
(*): significant difference between 2 groups.
(
PI: pelvic incidence, PT: pelvic tilt, LL: lumbar lordosis, GT: global tilt.
PI-LL: pelvic incidence and lumbar lordosis mismatch.
TPA, LPA, UIVPA: T1 pelvic angle, L1 pelvic angle, UIV pelvic angle.
C2-UIV+1PA: the angle between 2 lines C2_FH and UIV+1_FH (FH: femoral head).
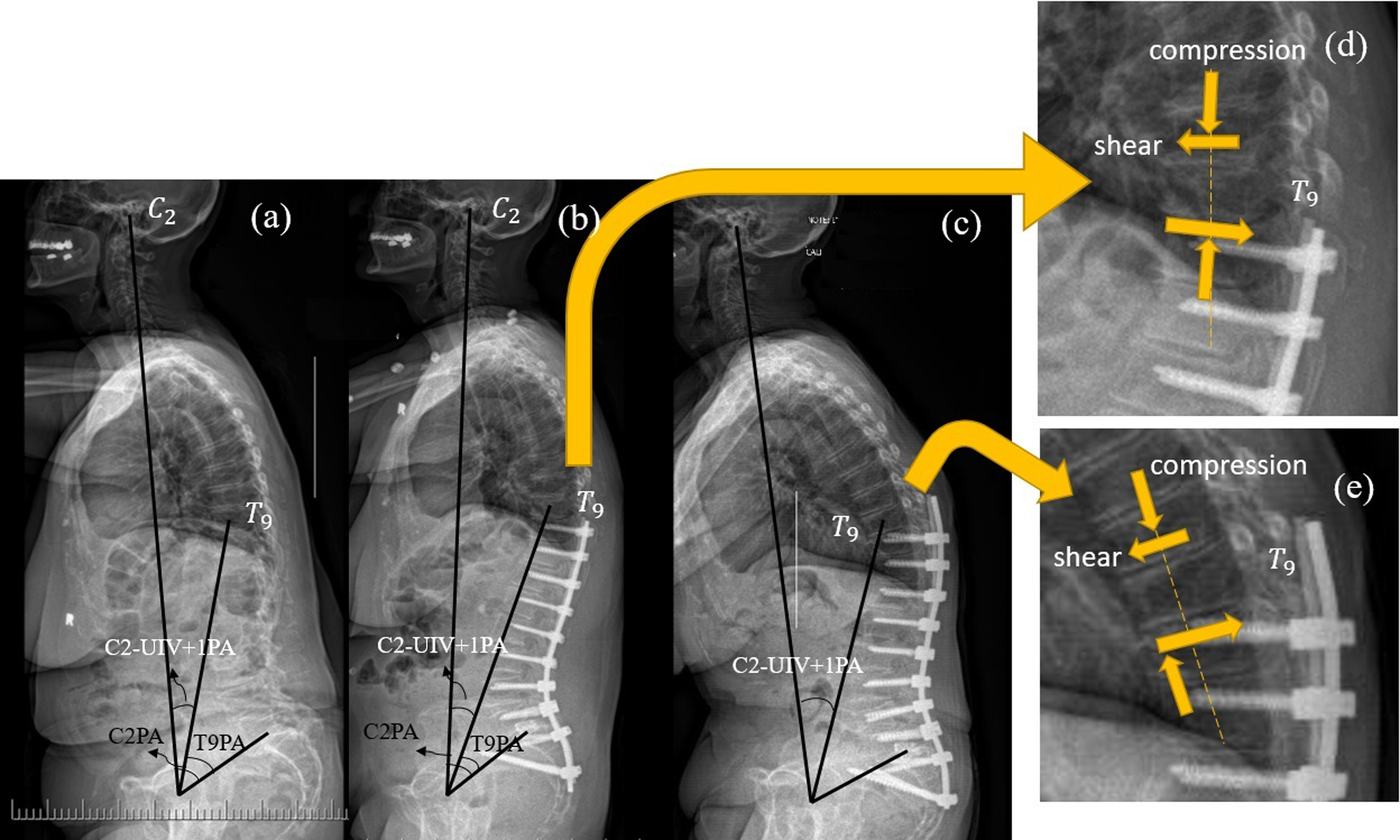
The demonstration of the C2-UIV+1PA angle or C2PA-T9PA mismatch in a patient with (A) preop, (B) immediate postop, and (C) 3-y follow up images. (D) Compression and shear forces on the superior and inferior endplates of T9 (UIV+1) in the immediate postop status, (E) displaced compression as a result of shear couple in the rotated posture of UIV+1 in the PJK stage.
Association of Vertebral Loading with PJK Development
The vertebral loading including compression and shear forces at UIV and UIV+1 (adjacent forces) was determined using the musculoskeletal analysis for PJK and non-PJK groups. To eliminate the effect of weight in the sagittal alignment-vertebral loading association study, adjacent forces were normalized to the patient’s weight. For most alignments, surgical fusion induced shear forces in opposite directions around UIV+1, i.e., anterior shear force at the superior surface and posterior shear force at the inferior surface. These opposing shear forces generate a shear couple (difference of these shear forces multiply by vertebral height) that contributes to forward bending of UIV+1. Given this observation, we sought to explore the association between this shear couple and PJK development. Additionally, the average of the absolute values of compression on the superior and inferior vertebral surfaces was represented as vertebral compressive force (Figure 2(D)).
Comparison Between Mean Postoperative Normalized Vertebral Loading and Load Ratios at UIV and UIV+1 Levels.
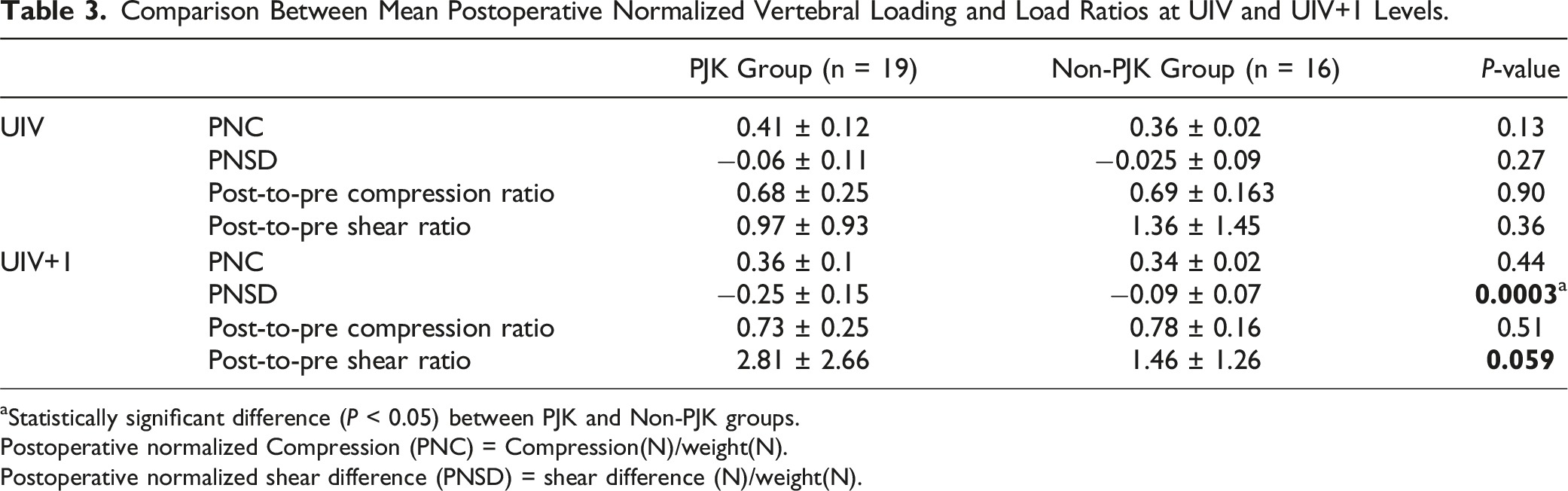
aStatistically significant difference (P < 0.05) between PJK and Non-PJK groups.
Postoperative normalized Compression (PNC) = Compression(N)/weight(N).
Postoperative normalized shear difference (PNSD) = shear difference (N)/weight(N).
Diagram of the Number of PJK and Non-PK (NPJK) Patients Based on (a) Normalized Shear Values and Post-to-pre Shear Ratio, and (b) Postoperative Normalized Compression Values and Post-to-pre Compression Ratio at UIV+1.
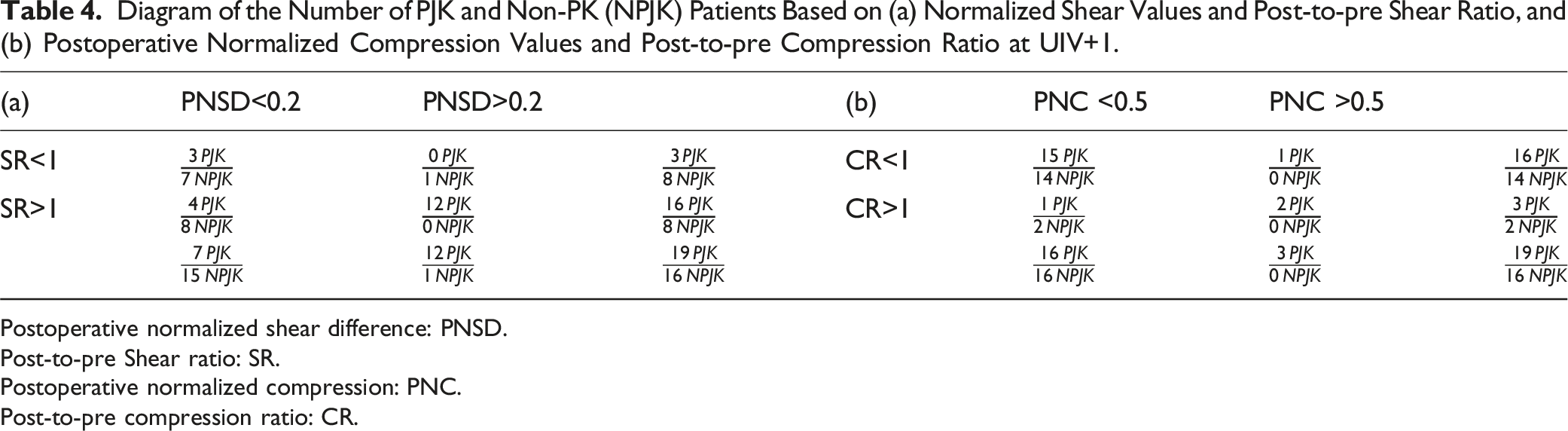
Postoperative normalized shear difference: PNSD.
Post-to-pre Shear ratio: SR.
Postoperative normalized compression: PNC.
Post-to-pre compression ratio: CR.
Of 16 non-PJK patients, 15 had postoperative normalized shear difference at UIV+1 (PNSD) < 0.2 (Table 4), and all experienced postoperative normalized compression (PNC) < 0.5 (Table 4). Notably, there were no non-PJK patients found in the regions combining high shear with a high shear load ratio (PNSD >0.2, SR >1), and high compression with high compression ratio (PNC >0.5, CR >1) called high-risk zones. This highlights the importance of lower vertebral loading at the early postoperative stage in preventing the occurrence of PJK. In contrast, these high-risk zones encompassed 14 patients who developed PJK. From the other 5 patients in the PJK group, 3 experienced higher postoperative shear forces compared to their preoperative ones (SR >1), despite their low shear values (PNSD<0.2). Those cases might demonstrate the need for more accurate and potential patient-specific threshold, but suggests that factors beyond alignment, such as bone and muscle quality, also contribute to the development of PJK. Figure 3 demonstrates a case of PJK and a case of non-PJK with their demographic data, pre and postoperative shear and compression with their load ratios. The demonstration of 2 PJK and non-PJK cases with their demographic data, pre and postoperative shear and compression with their load ratios.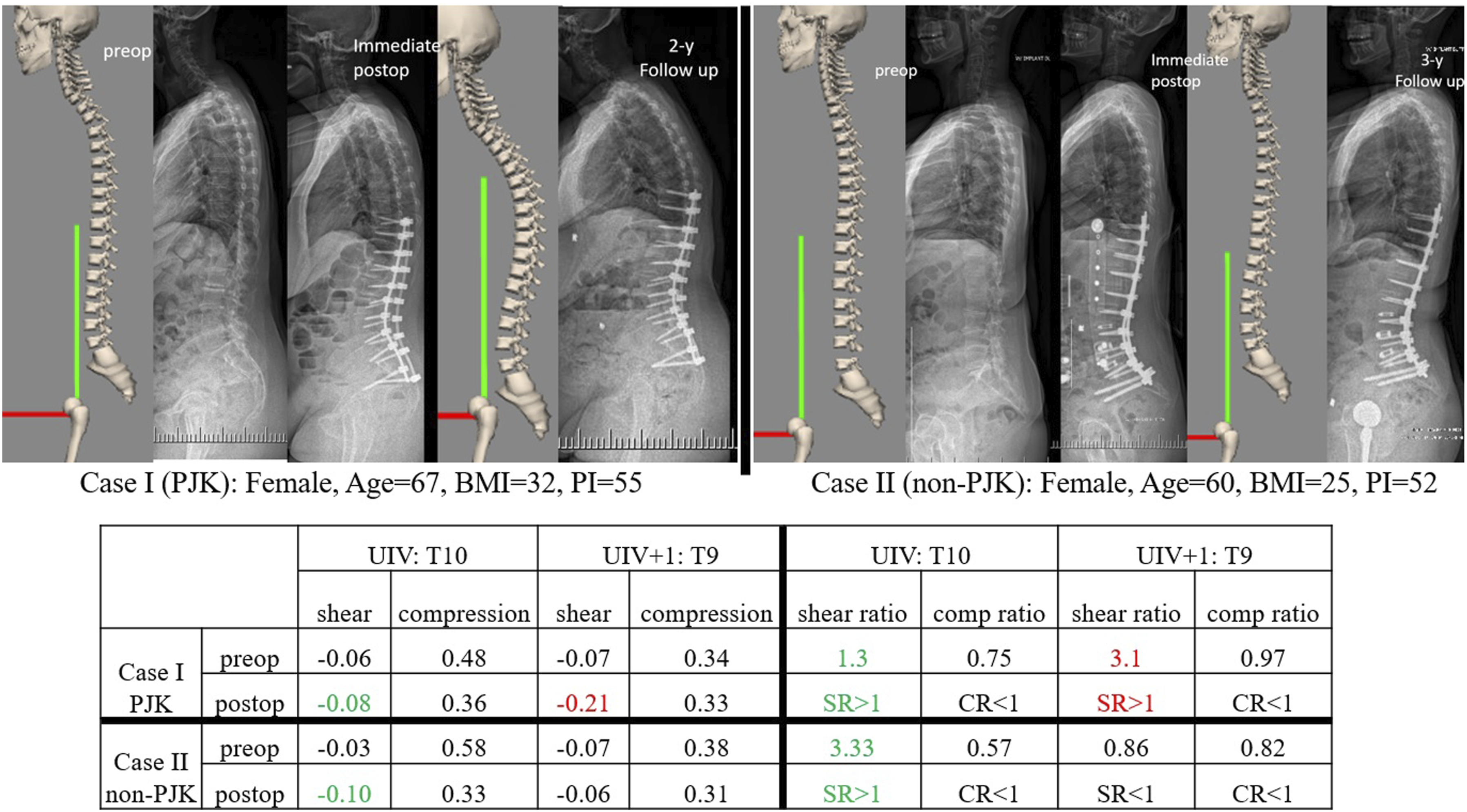
Discussion
Thirty patients (85%), 16 PJK (84%) and 14 non-PJK (87%), had low post-to-pre compression ratio (Table 4) indicating that for most patients compressive loading at the proximal junction decreases postoperatively. However, 24 patients (68%), 16 PJK (84%) and 8 non-PJK (50%), experienced higher shear force postoperatively. Although fusion decreases compression and increases shear forces at adjacent levels in most cases, the trends cannot be generalized, and it depends on post-to-pre changes in sagittal alignment. Factors such as weight and coronal alignment have an impact on vertebral loading; thereby, to study the vertebral loading changes due to sagittal alignment, we isolated the effect of sagittal alignment by normalizing vertebral loading to patients’ weights and disregarding their coronal alignments. This research highlights the postoperative shear value as an important risk factor for PJK development and underscores the importance of future work regarding preplanning alignment to optimize shear values at adjacent levels to reduce the risk of PJK occurrence.
In the analysis of forces at the UIV and UIV +1, it is demonstrated that compressive loading did not change significantly between PJK and non-PJK groups. However, the shear difference at the UIV+1 level was notably higher in the PJK group compared to the non-PJK group. Furthermore, apart from assessing shear status (high/low), post-to-pre load ratio assessment also needs to be considered. Osteoporosis, independent of sagittal malalignment, is a well-known risk factor for PJK,35,36 however we believe that studying preoperative loading provides the opportunity to consider BMD and sagittal alignment simultaneously by evaluating the vertebra’s load bearing ability based on its preoperative condition. Low post-to-pre ratio indicates safe zone in terms of PJK probability and specifies the ability of the vertebra to tolerate postoperative loads even in the presence of high shear or compression. As demonstrated in Tables 4a and 4b, 16 of 19 PJK patients experienced higher postoperative shear than their preoperative value; moreover, 8 of 16 non-PJK patients were in the low shear ratio zone (SR <1) and 14 of them were in the low compression ratio zone (CR <1). It is worth mentioning that there were no significant differences in spinopelvic parameters of PJK and non-PJK groups pre and postoperatively, however there were significant differences in global alignment parameters TPA, GT, and C2-UIV+1PA angle. Therefore, comparing postoperative vertebral forces with preoperative forces provides valuable insights for potentially predicting PJK development by combining the impact of BMD status and adjacent forces resulting from postoperative sagittal alignment.
There are interactions between postoperative vertebral loading values and post-to-pre load ratios, which can be recognized from the changes in the number of PJK and non-PJK patients in Table 4 In the low shear ratio zone (SR <1), the number of PJK patients from 3 at low shear (<0.2) decreased to zero at high shear (>0.2). Conversely, in the high shear ratio (SR >1) category, the number of PJK patients increased from 4 in low shear zone to 12 in high shear zone. This contrasting trend in PJK occurrence between low and high shear values within different shear ratio zones indicates an interaction between these 2 parameters. Similarly, in Table 4, a decreasing trend in the number of PJK patients can be noted from low compression to high compression in the low compression ratio (<1). Conversely, the number of PJK patients increased in the high compression ratio zone, which again suggests an interaction between compression values and compression ratios.
We demonstrated that postoperative alignment in the high-risk zones characterized by a combination of high shear difference at the UIV+1 level (NSD >0.2) and high shear ratio (SR >1), as well as high compression difference at UIV+1 (NC >0.5) and high compression ratio (CR >1), is strongly associated with the development of PJK. Alignments that do not meet any of high-risk zone criteria were proposed as safe alignments. Incorporating the preoperative loading in the post-to-pre load ratio, makes the high-risk zone criteria patient specific. Using the proposed biomechanically derived criteria, we successfully identified all non-PJK patients (100% specificity) and predicted PJK development in 14 out of 19 patients (73% sensitivity). The moderate sensitivity suggests that factors other than alignment may have contributed to this adverse event. Furthermore, 3 out of 5 non-predicted PJK patients were in the low shear but high ratio zone; this may be due to the setting of the shear load threshold. Further investigation is required to identify the optimal patient-specific threshold which may consider other factors such as muscle weakness or pseudarthrosis at the UIV.
In all but 5 patients, shear forces at the UIV+1 create a counterclockwise shear couple; anteriorly directed shear force at the superior endplate and posteriorly directed shear force at the inferior endplate which tends to bend the vertebra forward. To maintain equilibrium at this level, an opposing (clockwise) moment in UIV+1 is generated by shifting compression under the rotated UIV+1. These changes are depicted in Figure 2(D) and (E). The rotated UIV+1 on the top of UIV shifts UIV/UIV+1 compressive loading anteriorly, increasing the Cobb angle between UIV and UIV+1 and shifting the compressive loading to the superior anterior aspect of the UIV vertebral body. Depending on the bone mineral density of UIV and UIV+1, this can cause compression fracture at the superior anterior wedge of UIV and/or inferior anterior wedge of UIV+1; consequently, contributing to proximal junctional failure (PJF) development. Therefore, shear couple at UIV+1 is 1 of the crucial contributing factors for PJK development with the mentioned causative mechanism, which can be effected by variety of alignment-related risk factors including LL overcorrection, 37 pelvic non-responsiveness, 38 posteriorly displaced L1 (L1-gravity line distance), 39 and more posterior UIV location from femoral head. 40
While numerous strategies have been employed to lower the risk of PJK, focusing on minimizing shear couple through pre-planned sagittal alignment with minimal shear at the UIV+1 level is potentially a crucial step in PJK prevention. The approach of utilizing Bezier curve can be used to simulate pre-planned alignment and assess shear loading at the proximal junction. This offers a valuable opportunity to decrease the risk of PJK development. Predicting postoperative alignment has always been essential for identifying postoperative complications. Lafage et al. 41 analyzed sagittal alignment, free of the influence of PJK by developing a virtual model, which consists of a combination of postoperative alignment from fused pelvis to UIV-1, preoperative alignment of unfused segment (C2-UIV), and the correction of PT based on the following equation: PT =1.14 + 0.71 × PI – 0.52 × (maximum lumbar lordosis) – 0.19 × (maximum thoracic Kyphosis). To exclude the effect of PJK on sagittal alignment, immediate postop images were used in our study. It has identified that increased shear forces at the UIV+1 is associated with the development of PJK in addition to confirming already established global malalignment measures. This elucidates the possibility of utilizing biomechanical modelling to compare and determine optimal sagittal alignment to lower shear forces and lesser PJK risk.
Although our study has several unique strengths, it is important to acknowledge several limitations. A primary limitation is the small sample size and the inclusion of patients from 2 surgeons at a single institution and thus our results may not be generalizable. To establish the effectiveness of vertebral loading assessment in predicting PJK development, larger cohorts should be investigated. However, it is crucial to note that this study demonstrated the feasibility of a musculoskeletal analysis-based approach to determine a causative mechanism for PJK development based on immediate postoperative sagittal alignment. A second limitation pertains to the omission of other factors associated with PJK, such as osteoporosis and sarcopenia, in our analysis. These parameters were not considered in this study, which may have implications for the comprehensiveness of our current findings and future work.
Conclusion
This research demonstrates that the shear couple resulting from shear forces around UIV+1 mostly increases due to the fusion and can count as the main causative mechanism of PJK development. This study has described the loading changes at the proximal junction following ASD surgery and the relationship between increased shear forces and development of PJK. We propose 2 thresholds for normalized shear and compression: 0.2 and 0.5, respectively. A high-risk zone was defined by combining the high shear/compression with high post-to-pre load ratio (>1). The outcome of this research suggests that the preoperative planning and alignment goals need to consider the impact of shear force at the proximal junction to optimize sagittal alignment while decreasing the risk of PJK.
Supplemental Material
Supplemental Material - The Association Between Adjacent Forces and the Development of Proximal Junctional Kyphosis: A Musculoskeletal Analysis
Supplemental Material for The Association Between Adjacent Forces and the Development of Proximal Junctional Kyphosis: A Musculoskeletal Analysis by Fatemeh Alavi, Christopher J. Nielsen, Stephen Lewis, Raja Rampersaud, and Angela M. Cheung in Global Spine Journal
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions of Dr. Dennis E. Anderson and Dr. Jacob J. Banks for their support in the musculoskeletal analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Schroeder Arthritis Institutes, University Health Network and UHN foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.