
Abstract
Purpose:
The initial treatment of dropped head syndrome (DHS) is basically nonsurgical, but the mode of onset of DHS and efficacy of conservative treatment have not been fully clarified.
Methods:
The subjects were 38 DHS patients without neuromuscular disease (11 men and 27 women, average age 74.5 years). Cervical collar, physical therapy, and temporary medication for cervical pain were provided for all DHS patients. The following parameters were measured on lateral global spine standing radiographs: sagittal vertical axis (SVA), cervical sagittal vertical axis, C2–C7 angle, first thoracic slope, thoracic kyphosis, lumbar lordosis, sacral slope, pelvic tilt, and pelvic incidence. According to the mode of onset of DHS, the subjects were classified into acute-onset group (<3 months) and chronic-onset group (≥3 months).
Results:
Acute- and chronic-onset DHS were observed in 20 and 18 patients, respectively. A history of cervical trauma was involved in nine and two cases of acute- and chronic-onset DHS, respectively. Acute-onset DHS included more balanced-SVA (B-SVA: −30 mm <SVA ≤40 mm) than chronic-onset DHS. In conservative cases, the recovery rate was better in acute-onset DHS with B-SVA. In acute-onset DHS treated conservatively, the recovery rate was significantly poor in cervical trauma cases.
Conclusions:
Acute-onset DHS includes more balanced SVA and a history of cervical trauma, while acute-onset DHS without a history of cervical trauma has better prognosis by conservative treatment. Surgical indications for DHS should be carefully determined, and sufficient conservative treatment is essential.
Keywords
Introduction
Dropped head syndrome (DHS) is followed by severe neck extensor muscle weakness, resulting in head overflexion or the so-called chin-on-chest deformity in upright position. DHS patients occasionally present with stiff neck pain and the inability to maintain a horizontal gaze. In 1992, Suarez and Kelly presented a syndrome characterized by a dropped head accompanied by neck extensor weakness without specific abnormality on electromyography or biopsy. 1 A typical characteristic of DHS patients is that the neck deformity can be corrected by passive neck extension, and these patients do not show severe cervical kyphosis in the temporary neutral position. 2 DHS caused by several neuromuscular diseases, 3 –5 and especially Parkinson's disease, has been well studied. 6 The term “isolated neck extensor myopathy” has been proposed to categorize a nonspecific DHS without neuromuscular or structural disorders and is considered to be of low prevalence. 7 Paraspinal muscle fatigue from kyphotic posture- and age-related muscle weakness has been considered as the causes of nonspecific DHS. 2,7,8 According to previous reports, the incidence of DHS seems to be greater in elderly woman, 9,10,11 and more than 80% of patients with DHS were older than 70 years. 11 As the proportion of elderly people increases, the number of patients with DHS followed by degenerative changes is expected to grow accordingly. Most previous studies have reported that dropped head condition was hardly improved by conservative treatment and surgery was then attempted. 1,7,12,13 However, we sometimes encountered patients whose symptoms, especially horizontal gaze, improved by conservative treatment. 9 The mode of onset of DHS without neuromuscular disease and the efficacy of conservative treatment remain controversial. Therefore, the objective of this study was to analyze the manner of the onset of DHS as well as the efficacy of conservative treatment.
Materials and methods
This research was a retrospective study of 38 consecutive DHS patients (DHS group: 11 men and 27 women; average age 74.5 ± 9.5 years) presenting with correctable chin-on-chest deformity, who visited our facility between 2014 and 2018. Conservative treatment (cervical collar, physical therapy, and temporary medication for cervical pain) was basically administered to all DHS patients. Physical therapy was performed at an outpatient clinic for posture guidance and strengthening of cervicothoracic extensor muscle with a physical therapist for at least 3 months. In addition, for imbalanced cases, pelvic exercise was also performed. DHS was defined as follows: (1) the patient showed chin-on-chest deformity in the natural position and had difficulty maintaining a horizontal gaze in an upright position for even a few minutes and (2) the deformity was correctable in the supine position. Recovery of DHS was evaluated by improvement of horizontal gaze in their general daily life based on interviews with the patients. The indications for surgery were the patients with severe activities of daily living (ADL) impairments (due to difficulty in maintaining a forward gaze, in standing, in sitting, in walking or in swallowing), who could not respond to conservative treatment. The mean follow-up period was 34.1 ± 20.3 months. Patients with posterior longitudinal ligament ossification, with neuromuscular disease, or with coronal deformity >30° were excluded. From the awareness of symptoms such as stiff neck pain and the inability to maintain a horizontal gaze due to chin-on-chest deformity was defined as the onset period. According to the onset period, the subjects were divided into acute-onset DHS (<3 months) and chronic-onset DHS (≥3 months).
Whole spine anteroposterior and lateral radiographs were obtained by using digital slot-scanning radiography of a Sonialvision Safire fluoroscopy system (Shimadzu, Kyoto, Japan) in the most stable, relaxed standing position with possible knee extension while maintaining a horizontal gaze in the fists-on-clavicle posture. 14 The following parameters were measured: sagittal vertical axis (SVA, length from the plumb line dropped from the posterior–superior corner of the S1 vertebral body to the plumb line dropped from the center of C7), C2–C7 sagittal vertical axis (C-SVA, length from the plumb line dropped from the posterior–superior corner of the C7 vertebral body to the plumb line dropped from the center of C2), C2–C7 angle (angle from the lower endplate of C2 to the lower endplate of C7), first thoracic slope (T1 S, angle between the T1 upper endplate and the horizontal plane), thoracic kyphosis (TK, angle from the upper endplate of T4 to the lower endplate of T12), lumbar lordosis (LL, angle from the upper endplate of L1 to the upper sacral endplate), sacral slope (SS, angle between the sacral plate and the horizontal plane), pelvic tilt (PT, angle between the line connecting the midpoint of the sacral plate to the axis of the femoral heads and the gravity line), and pelvic incidence (PI, angle between the line perpendicular to the sacral plate from its midpoint and the line connecting the point to the middle axis of the femoral heads). 15,16 The inter-agreement rates of the measurements were satisfactory. 17 In reference to the previous standard measurement and the classification of global sagittal spinal alignment, 18 –20 the DHS group was divided into two groups according to SVA: normal balanced SVA (B-SVA); −30mm < SVA ≤ 40 mm and imbalanced SVA (IB-SVA); SVA ≤ −30 mm or SVA > 40 mm. IB-SVA was further divided into positive SVA (P-SVA), SVA > 40 mm and negative SVA (N-SVA), SVA ≤ −30 mm. This study was approved by the Institutional Review Board of our university. Values were presented as mean ± standard deviation. JMP software package version 10.0 (SAS Institute Inc., Cary, North Carolina, USA) was used for statistical analysis. Wilcoxon–Mann–Whitney test was used for pairwise comparisons. Χ 2 test was used for categorical variables. A p-value of <0.05 was considered to indicate a statistically significant difference.
Results
Comparison between acute-onset DHS and chronic-onset DHS
The number of patients with acute and chronic DHS was 20 cases (average age 73.7 years, 8 males and 12 females) and 18 cases (75.4 years, 3 males and 15 females), respectively. A history of cervical trauma was seen in nine cases with acute-onset DHS (eight cases from falling and one case from radiation therapy for esophageal cancer) and two cases with chronic-onset DHS (both with a history of cervical laminoplasty), respectively; the rate was significantly higher in acute than in chronic-onset DHS (Table 1). Most of the patients with a history of cervical trauma did not have severe cervical bony and soft tissue injury, but C7 vertebral fracture without severe cervical pain and neurological deficit was found in one patient with acute-onset DHS.
Background of acute- and chronic-onset DHS.a

DHS: dropped head syndrome; SVA: sagittal vertical axis; B-SVA: normal balanced SVA; IB-SVA: imbalanced SVA; P-SVA: positive imbalanced SVA; N-SVA: negative imbalanced SVA; NS: not significant.
a Values are expressed as mean ± standard deviation.
Global sagittal spinal alignment
Regarding global sagittal spinal alignment, 14 of 20 (70%) with acute-onset DHS represented B-SVA, whereas only 6 of 18 (33%) were classified as B-SVA in the chronic-onset DHS group (Table 1). When global sagittal spinal alignment was analyzed in detail by dividing each group of subjects into P- and N-SVA, the presence of P-SVA and N-SVA showed no significant difference in acute- and chronic-onset DHS (Table 1, Figure 1). The average values of the respective parameters of global sagittal spinal alignment between acute- and chronic-onset DHS did not differ significantly (Table 2).
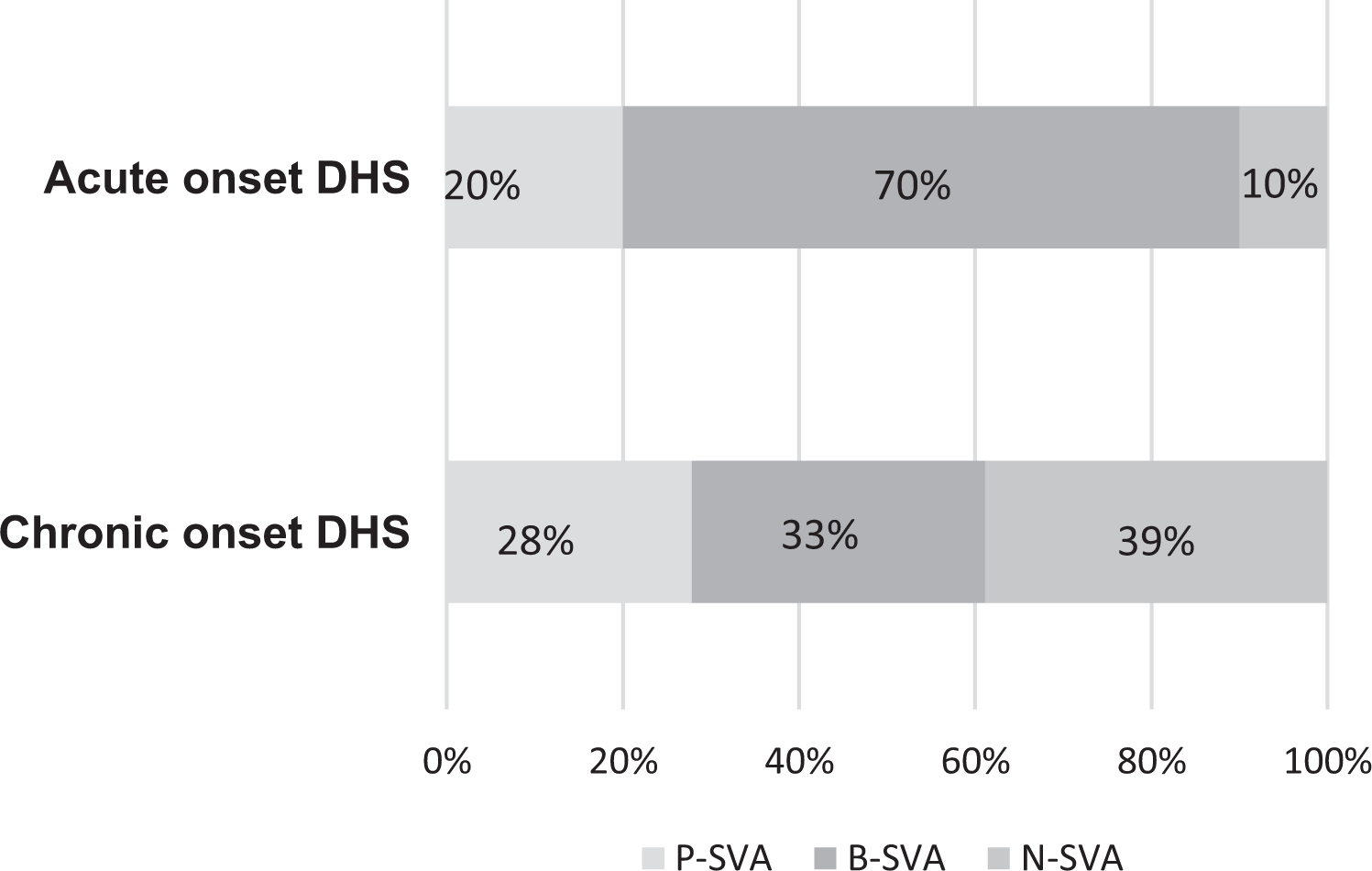
Global sagittal spinal balance in acute- and chronic-onset DHS. DHS: dropped head syndrome; SVA: sagittal vertical axis; B-SVA: normal balanced SVA; P-SVA: positive imbalanced SVA; N-SVA: negative imbalanced SVA.
Global sagittal spinal alignment in acute- and chronic-onset DHS.a

DHS: dropped head syndrome; SVA: sagittal vertical axis; C-SVA: C2–7 sagittal vertical axis; T1 S: first thoracic slope; TK: thoracic kyphosis; LL: lumbar lordosis; SS: sacral slope; PT: pelvic tilt; PI: pelvic incidence; NS: not significant.
a Values are expressed as mean ± standard deviation.
Treatment results
Cervical collar, physical therapy, and temporary medication for cervical pain were basically provided for all DHS patients. Five of 20 (25%) acute-onset DHS cases and 6 of 18 (33.3%) chronic-onset DHS cases underwent surgery, and there was no statistical difference between the two groups (Table 3). Comparing the recovery rate of the two conservatively treated groups, the recovery rate was higher in acute-onset DHS than in chronic-onset DHS. Of note was that 6 of 10 (60%) acute-onset DHS subjects with B-SVA recovered (Table 4).
Treatment of acute- and chronic-onset DHS.

DHS: dropped head syndrome; NS: not significant.
Recovery rate by conservative treatment of acute- and chronic-onset DHS.

DHS: dropped head syndrome; SVA: sagittal vertical axis; B-SVA: normal balanced SVA; IB-SVA: imbalanced SVA.
When the influence of a history of cervical injury was analyzed in the acute-onset DHS cases treated conservatively (n = 15), 7 of 9 (77.8%) without a history of cervical trauma recovered, whereas only 1 of 6 patients with such a history recovered, and this difference was statistically significant (Table 5).
Recovery rate by conservative treatment and history of cervical trauma of acute-onset DHS.
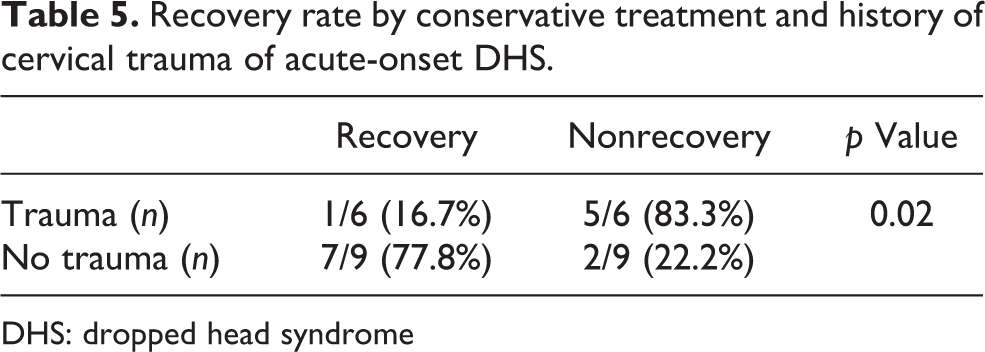
DHS: dropped head syndrome
Representative cases
Case 1
A 63-year-old male complained of difficulty in maintaining a horizontal gaze owing to dropped head condition through 2 months, and he had no history of cervical trauma or neuromuscular disease. The initial whole spine X-ray findings of the spinal sagittal parameters were as follows: SVA, −12 mm; C-SVA, 55 mm; C2–C7 angle, −29°; T1 S, 27°; TK, 21°; LL, 47°; SS 35°; PT, 24°; PI, 59°; and PI-LL, 12° (Figure 2(a) and (b)). SVA showed a normal balance. Therefore, this case was classified as acute-onset, B-SVA type DHS. Conservative treatment consisted of a neck collar brace, physical therapy, and temporary medication for neck pain. After 1 year of conservative treatment, the dropped head condition had been improved (SVA, 38 mm; C-SVA, 32 mm; C2–C7 angle, 13°; T1 S, 32°; TK, 32°; LL, 34°; SS, 31°; PT, 28°; PI, 59°; and PI-LL, 25°) (Figure 2(c) and (d)).
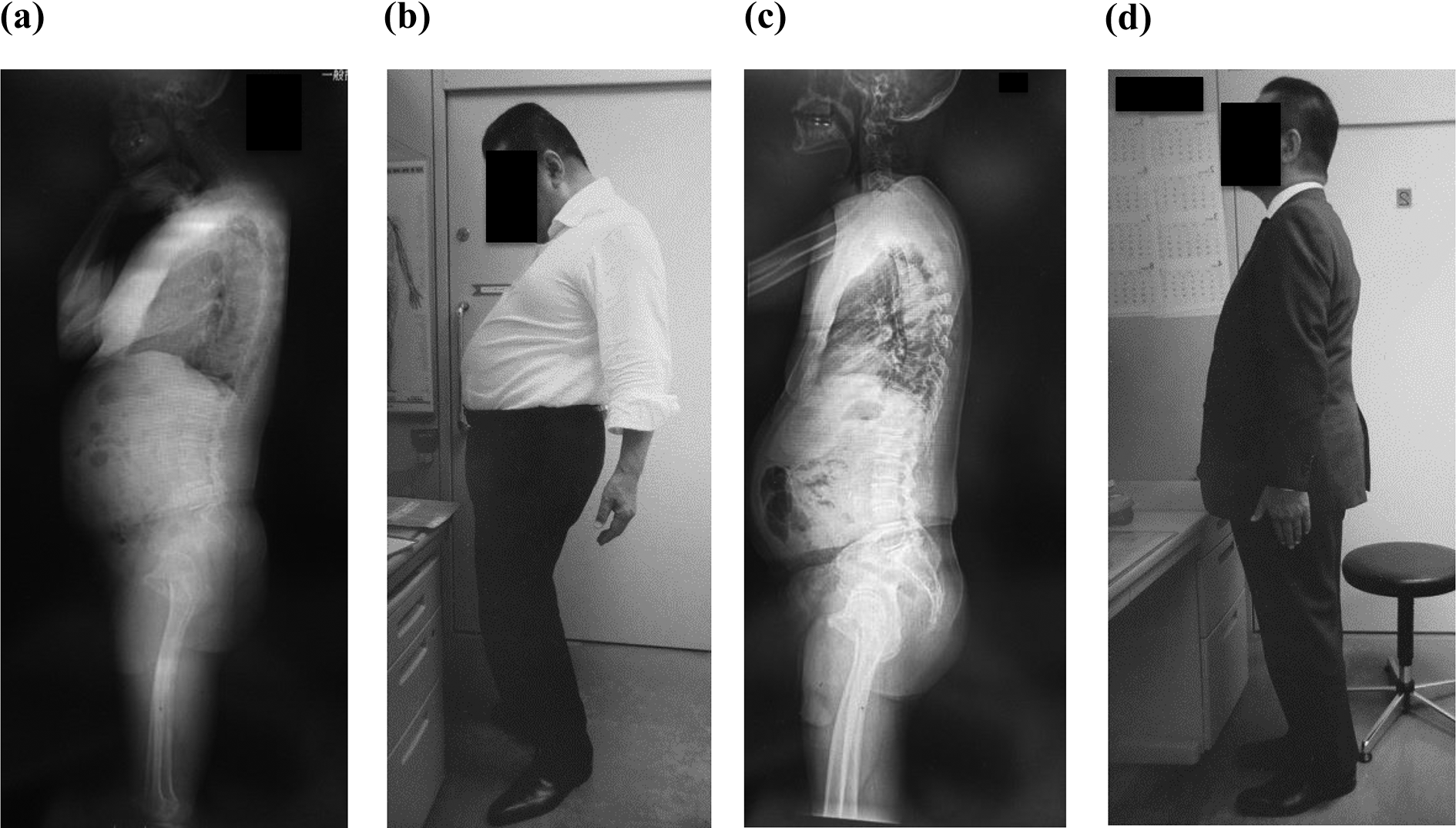
Case 1. (a) Global spine X-ray lateral view at initial attendance. (b) Photo at initial attendance. (c) Global spine X-ray lateral view after 1 year. (d) Photo after 1 year.
Case 2
A 62-year-old female complained of difficulty in maintaining a forward gaze and walking. The onset generally developed over 2 years. Her past illness was rheumatoid arthritis and she had taken steroids. Conservative treatment consisted of a neck collar brace, physical therapy, and temporary medication for neck pain. Initial findings of the spinal sagittal parameters were as follows: SVA, −63 mm; C-SVA, 43 mm; C2–C7 angle, −76°; T1 S, 7°; TK, 23°; LL, 61°; SS, 42°; PT, 18°; PI, 60°; and PI-LL, −1° (Figure 3(a) and (b)). SVA showed a negative imbalance. Therefore, this case was classified as chronic-onset, N-SVA type DHS. Conservative treatment given to her for more than 3 months was ineffective, and she still had severe ADL impairments. Cervical surgery was planned from C2 to T3. After anterior and posterior cervical corrective fusion, the cervical and global sagittal alignments were improved (SVA, −5 mm; C-SVA, 20 mm; C2–C7 angle, 3°; T1 S, 29°; TK, 38°; LL, 61°, SS, 44°; PT, 18°; PI, 62°; and PI-LL, 1°) (Figure 3(c) and (d)). Trunk balance was improved together with cervical symptoms.

Case 2. (a) Global spine X-ray lateral view at initial attendance. (b) Tomography at initial attendance. (c) Global spine X-ray lateral view after anterior cervical fixation.
Discussion
The present results showed that the distributions of acute- and chronic-onset DHS were almost equal. Acute-onset DHS included more B-SVA than chronic-onset DHS. The history of cervical trauma was prominent in acute-onset DHS. In nonsurgical cases, recovery was better in acute-onset DHS whose SVA belonged to B-SVA, whereas the recovery was significantly poorer in those patients with a history of cervical trauma. These results suggested that DHS patients with acute onset, balanced alignment, and no history of cervical trauma are likely to have a chance to recover by conservative treatment.
According to a case series report, seven DHS cases, 9 of which four were acute onset (from 1 day to 2 weeks) and three were chronic (gradual) onset (from 1 year to 5 years), and 6 DHS cases were treated nonsurgically. One patient with acute onset without a cervical trauma history improved well and two with chronic onset showed mild improvement, while the other three, two with acute onset and a history of cervical trauma and one with chronic onset, did not improve. Those results were similar to those of our study.
The present study also showed that acute-onset DHS included more B-SVA or a history of cervical trauma, which means that it did not originate from global sagittal spinal mal-alignment but rather that some local cervical injury, inflammation, or edematous change in cervical paraspinal muscles would have been the local cervical pathogenesis of the acute-onset DHS. 7 Kastrup et al. reported a case of acute-onset DHS whose diagnosis was cervical myositis based on biopsy and magnetic resonance imaging at cervical extensor muscle and trapezius. 21 As for chronic-onset DHS, on the other hand, more imbalanced SVA was present, indicating that it would develop, at least in some cases, by the gradual progression of cervical deformity accompanied by global spinal degeneration. Therefore, this would be one of the possible reasons for the recovery rate of chronic-onset DHS to be worse than that of acute-onset DHS.
Regarding global sagittal spinal alignment, DHS has two types: SVA+ and SVA−.
10,22
When all the participants in the current study were divided according to SVA+ and SVA−, there were 19 cases each with SVA+ and SVA−, and there was no difference between the two groups in terms of conservative treatment recovery rate (results not shown), leading us to conclude that conservative treatment recovery of DHS cannot be evaluated by SVA+/−. As cervical sagittal deformity is affected by global imbalance,
23
we then classified patients into three groups for a more detailed analysis. Yukawa et al. reported that the normative SVA value in more than 100 asymptomatic subjects in their 70 s ranged from −10 mm to +15 mm (average: 4.5 ± 11.9 mm in males and 1.8 ± 13.1 mm in females).
19
From the standpoint of standard global balance,
18
–20
we defined B-SVA as −30 mm
This study had the following limitations. (1) Although the number of DHS patients evaluated in this study was the largest in comparison to previous reports of DHS, it was still a relatively small number for a more detailed analysis, due mainly to the rare appearance of DHS. 2 (2) It was a cross-sectional study, and a longitudinal follow-up observation would be needed for researching the prognosis. (3) The precise definition of DHS has not been established, and the causes and alignment of DHS were diverse. 8,10,24,25 DHS is different from spodylotic cervical kyphosis, and cervical alignment of DHS is not stable and affected by extensor muscle fatigue. Therefore, it was difficult to define the recovery of DHS according to the duration of horizontal gaze and sagittal spinal alignment in X-ray. In this study, we defined the recovery of DHS by the improvement in horizontal gaze in their general daily life on the basis of patient interviews, which were considered to reflect the state of DHS. To the best of our knowledge, this is the first study to examine the relationship between the mode of onset of DHS and the efficacy of conservative treatment, and useful information could be expected for deciding DHS treatment strategies. The issues concerning conservative treatment recovery in DHS would be multifactorial, and they should be analyzed in greater detail (age, muscle conditions, dynamic factors, etc.) from this point in the future.
Conclusion
To estimate the efficacy of conservative treatment, it is necessary to ask patients with DHS concerning the mode of onset and the history of cervical trauma as well as to measure global sagittal alignment. Acute-onset DHS includes more balanced SVA and more histories of cervical trauma, although the prognosis is better by conservative treatment if there is no history of cervical trauma. Surgical indications for DHS should be carefully established, and satisfactory conservative treatment is imperative.
Footnotes
Acknowledgments
The authors are indebted to Mr Arndt Gerz for the editorial review of the English manuscript. Advice and comments given by him have been a great help to us. The authors are also grateful to Ms Yuri Amamizu of the Department of Orthopedic Surgery for assistance with preparation of the initial English manuscript.
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.