
Abstract
Study Design:
Retrospective cohort study.
Objectives:
The current evidence regarding how level of lumbar pedicle subtraction osteotomy (PSO) influences correction of sagittal alignment is limited. This study sought to investigate the relationship of lumbar level and segmental angular change (SAC) of PSO with the magnitude of global sagittal alignment correction.
Methods:
This study retrospectively evaluated 53 consecutive patients with adult spinal deformity who underwent lumbar PSO at a single institution. Radiographs were evaluated to quantify the effect of PSO on lumbar lordosis (LL), thoracic kyphosis (TK), sacral slope (SS), pelvic tilt (PT), pelvic incidence (PI), T1-spinopelvic inclination (T1SPI), T1-pelvic alignment (TPA), and sagittal vertical axis (SVA).
Results:
Significant correlations were found between PSO SAC and the postoperative increase in LL (r = 0.316, P = .021) and PT (r = 0.352, P = .010), and a decrease in TPA (r = −0.324, P = .018). PSO level significantly correlated with change in T1SPI (r = −0.305, P = .026) and SVA (r = −0.406, P = .002), with more caudal PSO corresponding to a greater correction in sagittal balance. On multivariate analysis, more caudal PSO level independently predicted a greater reduction in T1SPI (β = −3.138, P = .009) and SVA (β = −29.030, P = .001), while larger PSO SAC (β = −0.375, P = .045) and a greater number of fusion levels (β = −1.427, P = .036) predicted a greater reduction in TPA.
Conclusion:
This study identified a gain of approximately 3 degrees and 3 cm of correction for each level of PSO more caudal to L1. Additionally, a larger PSO SAC predicted greater improvement in TPA. While further investigation of these relationships is warranted, these findings may help guide preoperative PSO level selection.
Keywords
Introduction
Although coronal deformity may contribute to lower back pain,1,2 current evidence has largely identified fixed positive sagittal balance as the key underlying cause determining poor outcomes and disability in adult spinal deformity.3-5 A positive sagittal balance occurs when the center of gravity of the body falls anterior to the hip center due to an abnormal sagittal profile of the spine, and the patient alignment exceeds the cone of economy. 6 This is most commonly secondary to thoracolumbar spinal disc degeneration, iatrogenic malalignment following prior fusions or decompressions, trauma, or systemic arthritides such as ankylosing spondylitis.7,8 In an effort to compensate, sagittally imbalanced patients may retrovert the pelvis, flex the knees, hyperextend the hips, hypokyphose the thoracic spine, and hyperlordose the neck. These compensatory mechanisms may accelerate further degenerative changes along the weight bearing axis while doing little to mitigate symptoms.9,10
Recent years have seen a growing understanding of the complex relationships which exist between the spinal alignment, pelvic incidence, age, frailty, and other factors.11-13 These relationships have been investigated and utilized to develop patient-specific surgical targets for global spinal alignment which have been shown to correlate with improved health-related-quality-of-life (HRQOL) metrics and complication avoidance.
Development of these surgical targets has led to interest in predictability of surgical techniques utilized to correct sagittal malalignment. In order to correct sagittal imbalance and meet these surgical targets, osteotomies such as the posterior single column osteotomy (Ponte or Smith-Peterson) or the 3-column pedicle subtraction osteotomy (PSO) may be employed. The PSO is the most powerful osteotomy aside from the vertebral column resection and has been reported to generate over 30º of sagittal plane correction at each level.14-17 The PSO is most commonly utilized in patients with severe fixed sagittal imbalance, focal kyphosis, revision surgery for iatrogenic “flatback” syndrome, or in patients without a compliant intervertebral disc limiting efficacy of posterior single column osteotomies. 8
Despite its widespread utilization, few studies have evaluated the influence of the choice of lumbar level for PSO on global sagittal alignment. A multicenter study by Lafage et al studied the association between PSO location and the degree of osteotomy on spinopelvic correction in a series of 70 patients. 18 While the authors found several significant correlations, they did not find a relationship between the level of PSO and the magnitude of SVA correction. Biomechanically, this is not intuitive since a more caudally placed pivot point would in theory produce a greater effect along the rotational axis (Figure 1). However, other factors including the focal correction achieved with PSO, number of fusion levels, and surgical technique also may contribute.19,20
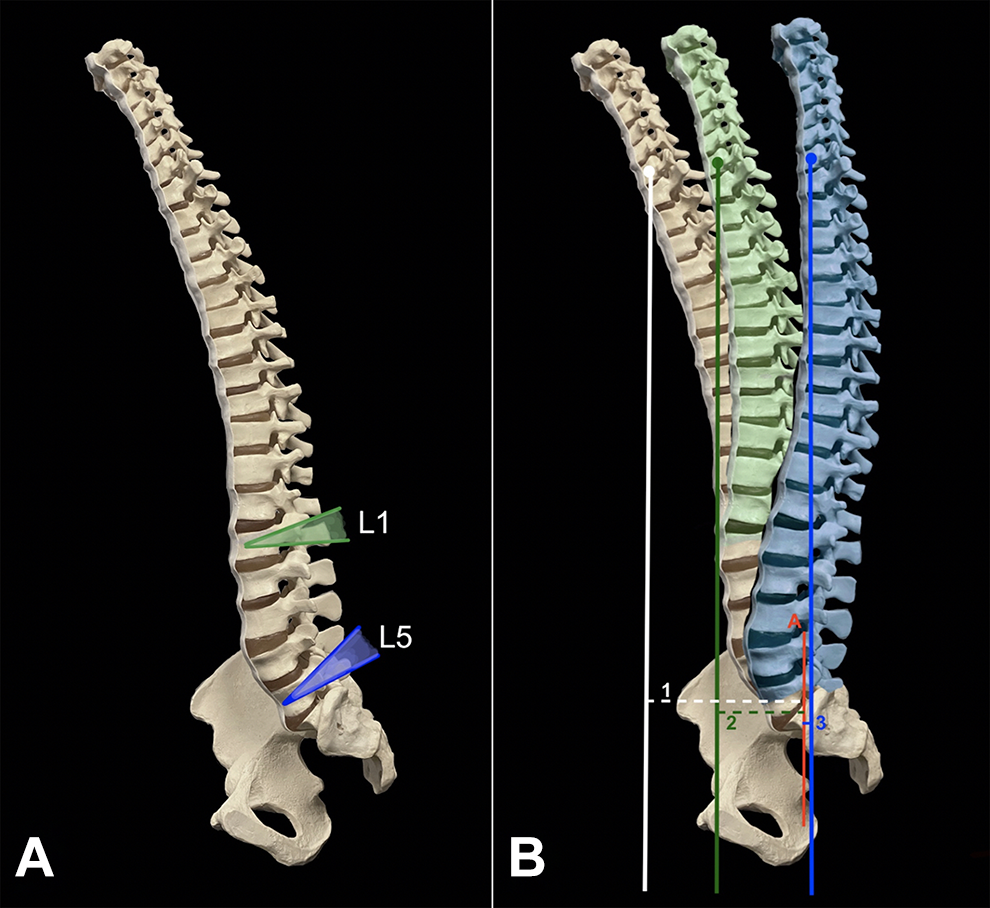
Representation of expected correction of sagittal vertical axis based on pedicle subtraction osteotomy (PSO) at differing levels. (A) Planned osteotomies at L1 and L5 vertebral bodies with (B) expected degree of correction increasing with more caudal PSO. Positive sagittal imbalance (Line 1) is returned to complete neutral axis in this model by L5 PSO (Line 3) compared to L1 PSO (Line 2). Line A = S1 endplate reference line for SVA measurement.
This study sought to further investigate how the level at which PSO is performed and the magnitude of focal correction achieved impact global sagittal alignment among a series of patients treated with lumbar PSO at a single institution.
Methods
Patient Selection
Institutional Review Board approval was obtained (ORA 21 031 201) to retrospectively query a prospectively maintained database for the medical records of all consecutive patients who underwent spinal fusion between 2008 and 2020 for adult deformity with concomitant lumbar PSO at a single tertiary medical institution with one of three senior surgeons. Due to the retrospective nature, this study was exempt from obtaining informed consent. The criteria for inclusion were patients over the age of 18 with adult spinal deformity who underwent PSO for fixed iatrogenic imbalance, kyphoscoliosis, ankylosing spondylitis, neuromuscular scoliosis, or congenital scoliosis characterized by at least one of the following: SVA of 5 cm or more, pelvic tilt of 25 degrees or more, lumbar lordosis of 20 degrees or less, focal lumbar kyphosis of 20 degrees or less, or thoracic kyphosis of 60 degrees or more. The level at which PSO was performed was determined during preoperative planning based on several considerations. PSO was most performed at L3 and L4 as osteotomy at these levels is technically easier and poses fewer risks to the patient. However, more cephalad (L1 and L2) or caudal (L5) PSO was performed for instances where the apex of kyphotic deformity was noted at these levels, and it was determined that optimal angular correction could be best achieved by performing the PSO here. Patients were excluded if they had incomplete pre-and postoperative imaging, or if the imaging was deemed insufficient (femoral heads and/or C7 vertebra were not visible on standing lateral radiographs).
Demographic data collected including age, height, weight, body mass index (BMI), primary diagnosis, level of PSO, number of fusion levels, whether the procedure was a revision of a prior fusion, and whether a short fusion (extending no higher than T10) or long fusion (extending above T10) was performed. Intraoperative/early perioperative (<6 months) and late postoperative (>6 months) complications were collected.
Radiographic Outcome Measures
All measurements were performed using the final preoperative and first postoperative full-length standing lateral radiographs on the Opal-RAD picture archiving and communication system (PACS) software (Konica Minolta, Tokyo, Japan).
Sagittal spinopelvic alignment was evaluated by measuring lumbar lordosis (LL), thoracic kyphosis (TK), sacral slope (SS), pelvic tilt (PT), pelvic incidence (PI), T1-spinopelvic inclination (T1SPI), T1-Pelvic Angle (TPA), and SVA (Figure 2). The difference between PI and LL was calculated to evaluate for mismatch. The degree of segmental angular correction following PSO (PSO SAC) was calculated as the change in lordosis measured from the inferior endplate of the vertebra cephalad to the PSO level and the superior endplate of the caudal vertebra (Figure 3).
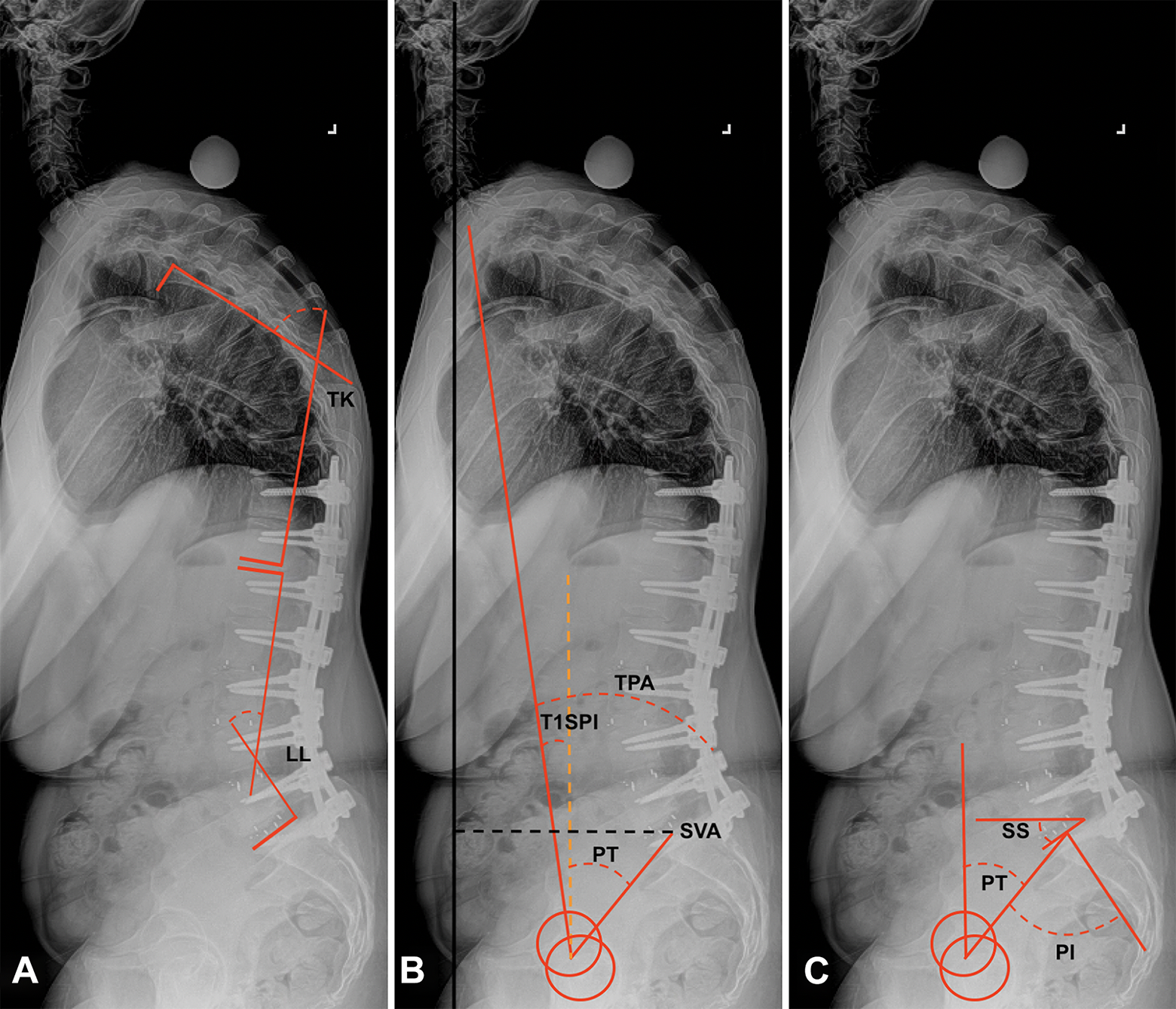
Parameters of sagittal spinopelvic alignment, including (A) lumbar lordosis (LL), thoracic kyphosis (TK), (B) pelvic tilt (PT), T1-spinopelvic inclination (T1SPI), T1-pelvic angle (TPA), sagittal vertical axis (SVA), (C) sacral slope (SS), and pelvic incidence (PI).
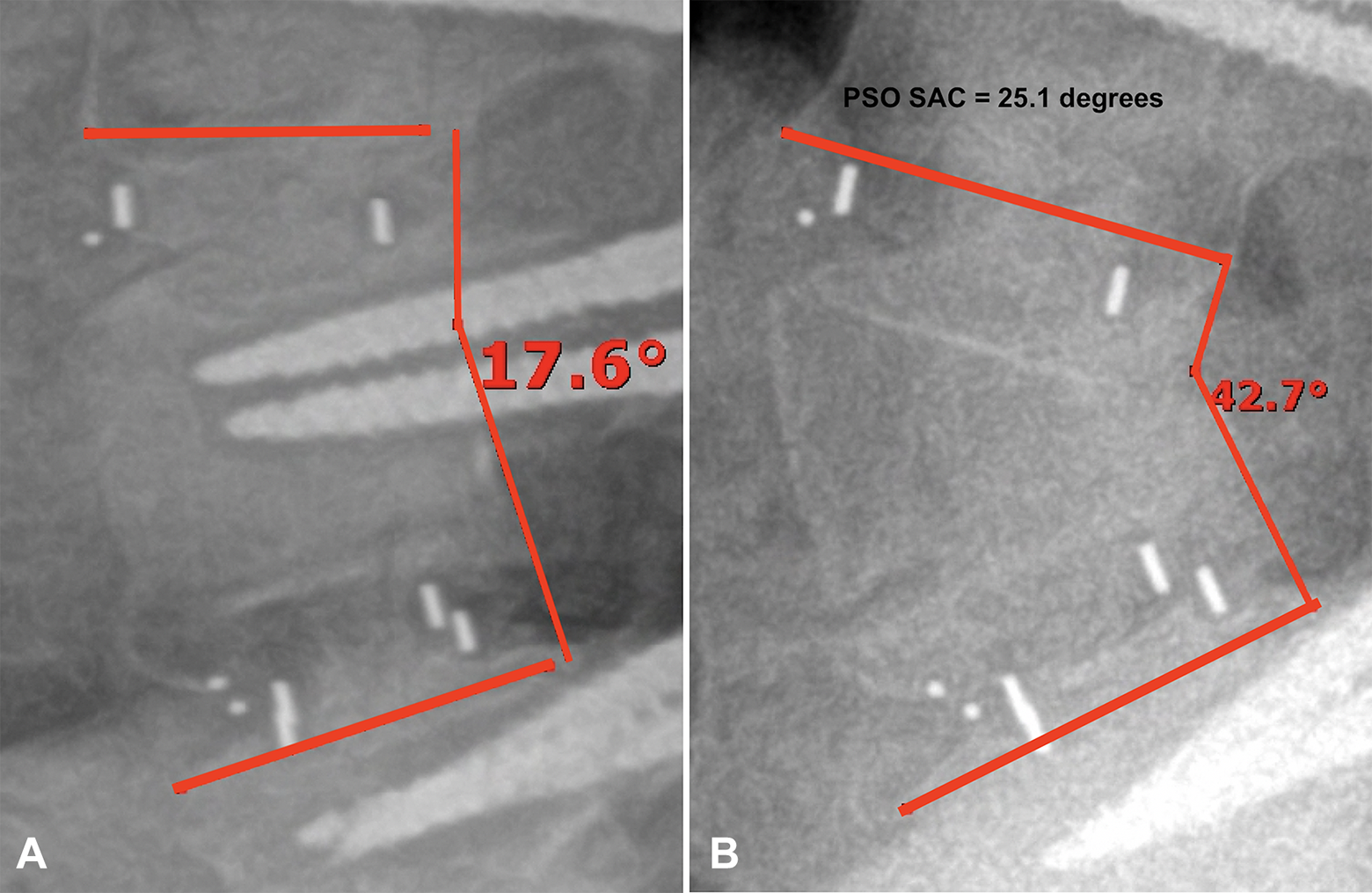
Measurement of the segmental angle from the inferior endplate of the cephalad vertebra and the superior endplate of the caudal vertebra (A) preoperatively and (B) after PSO. PSO SAC is calculated as the angular change post osteotomy.
Statistical Analysis
All statistical methods were performed using SPSS version 26.0 (IBM Corporation, Armonk, NY). Patient demographics were established using descriptive statistics. Continuous variables were reported as means with standard deviations, and categorical variables were reported as proportions and absolute counts, unless otherwise specified. Pre-to postoperative changes in spinopelvic alignment were evaluated using paired t-test. Correlation analysis was performed to evaluate the relationship between PSO SAC and PSO level on spinopelvic alignment using the Pearson correlation coefficient. Multivariate linear regression was performed to assess for independent variables predicting greater magnitudes of change in T1SPI, TPA, and SVA. 21 Model covariates included the level at which PSO was performed, PSO SAC, and other clinically relevant demographic and procedural variables selected by the senior authors. Complications were evaluated by PSO level using Pearson’s chi square, while the relationships between PSO SAC, PSO level, and PROs were explored via correlation analysis. The threshold for statistical significance was set to P < .05.
Results
Patient Demographics
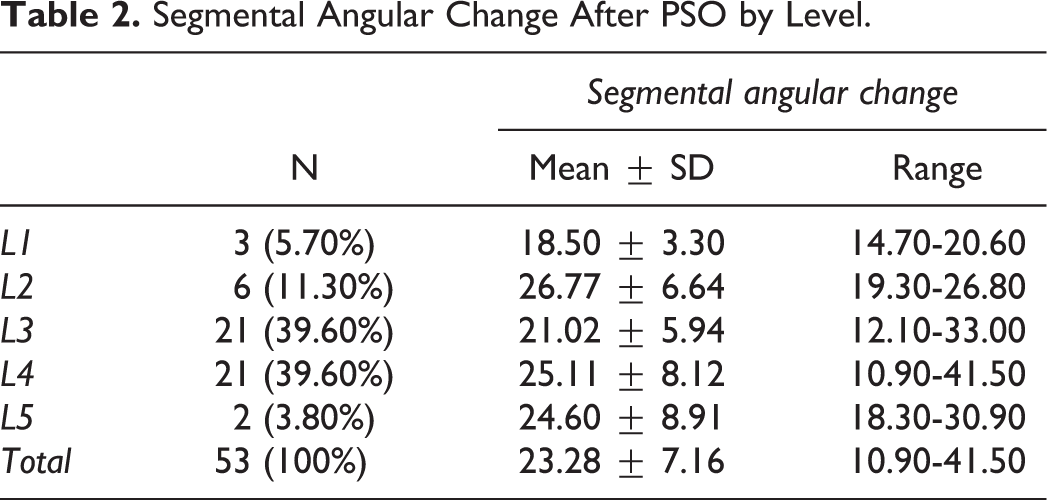
Overall, 64 patients underwent lumbar PSO between 2008 and 2020, of whom 11 were excluded on the basis of incomplete imaging, thus leaving 53 patients for statistical analysis. There were 37 women (69.8%) and 16 (30.2%) men with an average age of 62.06 ± 11.25 at the time of surgery and a mean follow-up of 42.32 ± 32.26 months (Table 1). The average number of levels fused was 8.08 ± 2.99 and 11 patients (20.8%) had a fusion that extended above T10. The PSO was performed at L1 in 3 patients (5.7%), L2 in 6 (11.3%), L3 in 21 (39.6%), L4 in 21 (39.6%), and at L5 in 2 (3.8%). The degree of PSO SAC was similarly distributed across lumbar levels on ANOVA analysis (P = .177), as demonstrated by Table 2.
Patient Demographics.
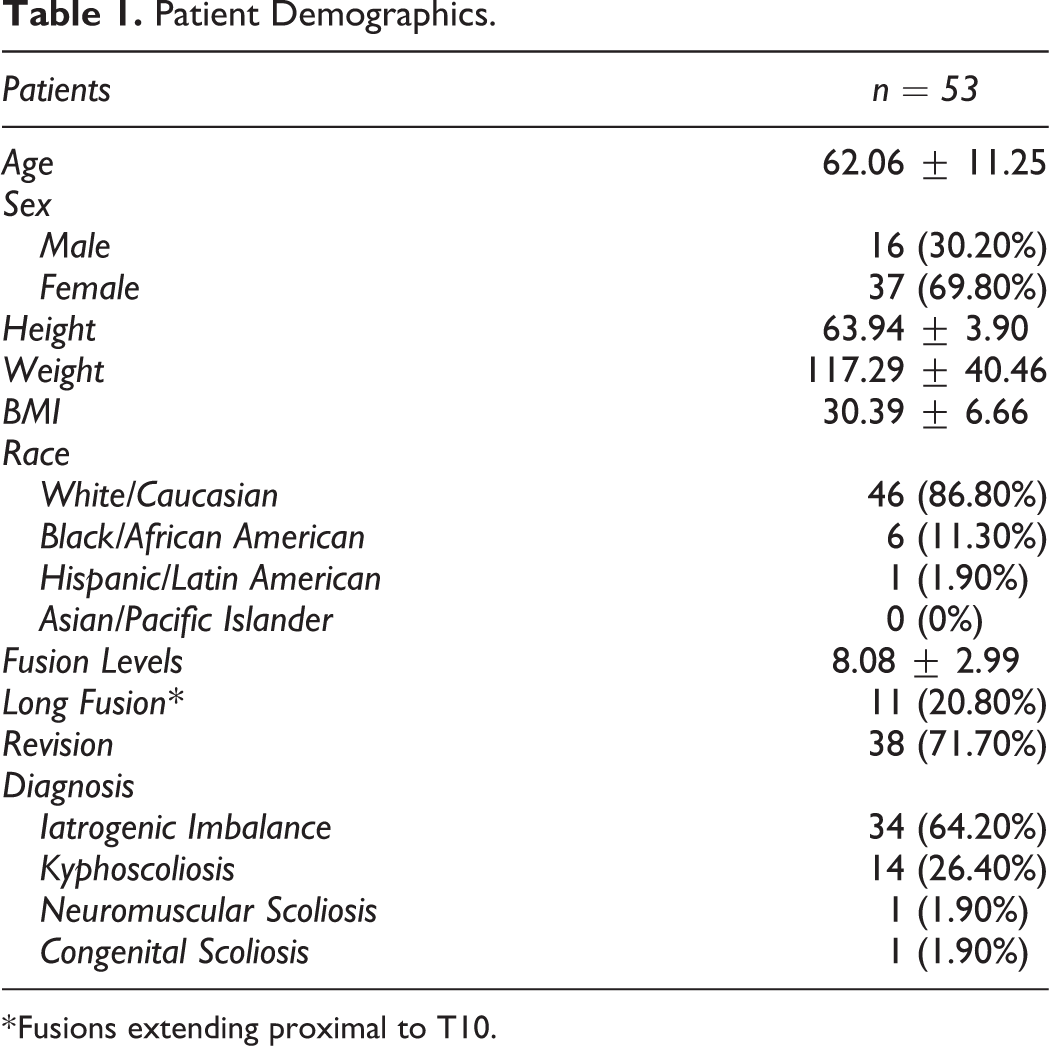
* Fusions extending proximal to T10.
Segmental Angular Change After PSO by Level.
Spinopelvic Correction
From preoperatively to postoperatively, there was significant correction in all parameters of spinopelvic alignment, including LL (P < .001), TK (P < .001), SS (P < .001), PT (P < .001), the mismatch between PI and LL (P < .001), T1SPI (P < .001), TPA (P < .001), and SVA (P < .001). There was no significant change in PI (P = .158), as expected, since this parameter is considered a constant (Table 3).
Sagittal Spinopelvic Alignment Pre-and Postoperatively.a
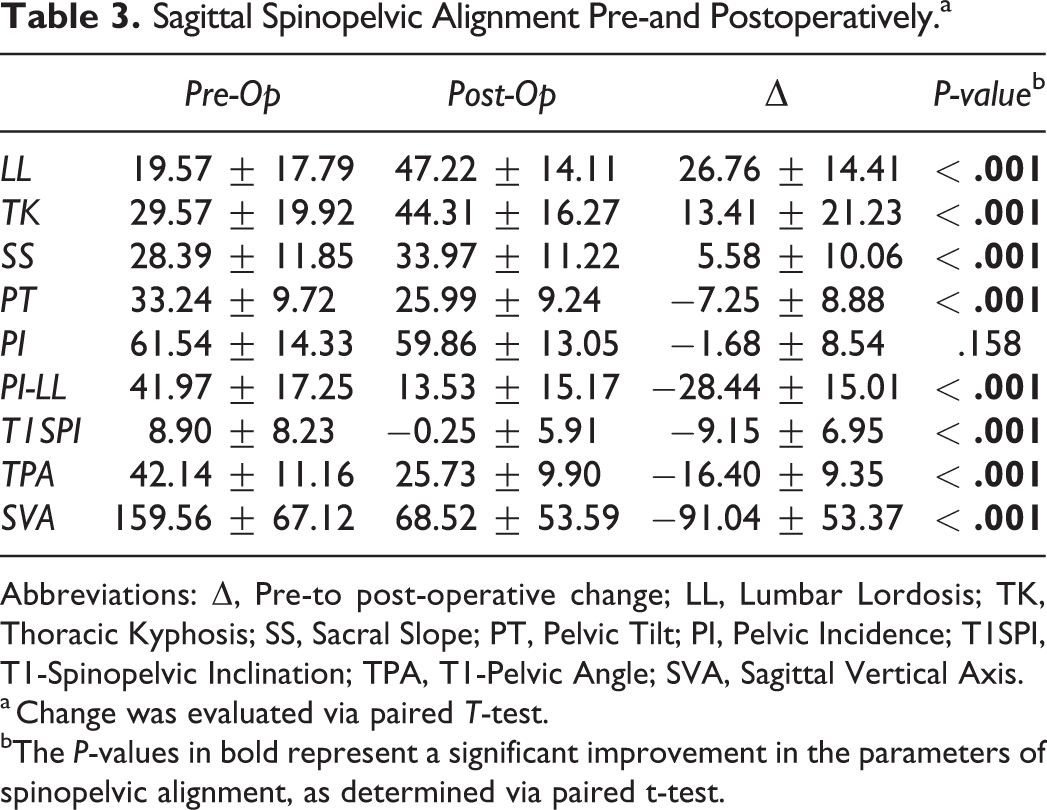
Abbreviations: Δ, Pre-to post-operative change; LL, Lumbar Lordosis; TK, Thoracic Kyphosis; SS, Sacral Slope; PT, Pelvic Tilt; PI, Pelvic Incidence; T1SPI, T1-Spinopelvic Inclination; TPA, T1-Pelvic Angle; SVA, Sagittal Vertical Axis.
a Change was evaluated via paired T-test.
bThe P-values in bold represent a significant improvement in the parameters of spinopelvic alignment, as determined via paired t-test.
Correlation Analysis
Using the Pearson correlation coefficient (r), the relationships between the change in sagittal alignment, PSO SAC, and PSO level were evaluated (Table 4). PSO SAC was significantly associated with ΔLL (r = 0.316, P = .021), ΔPT (r = −0.352, P = .010), and ΔTPA (r = −0.324, P = .018). Clinically, this can be interpreted as a significantly greater increase in LL, greater reduction in PT (i.e., pelvic anteversion), and greater reduction in TPA with a larger PSO.
Correlation Analysis Using the Pearson Coefficient (r).a
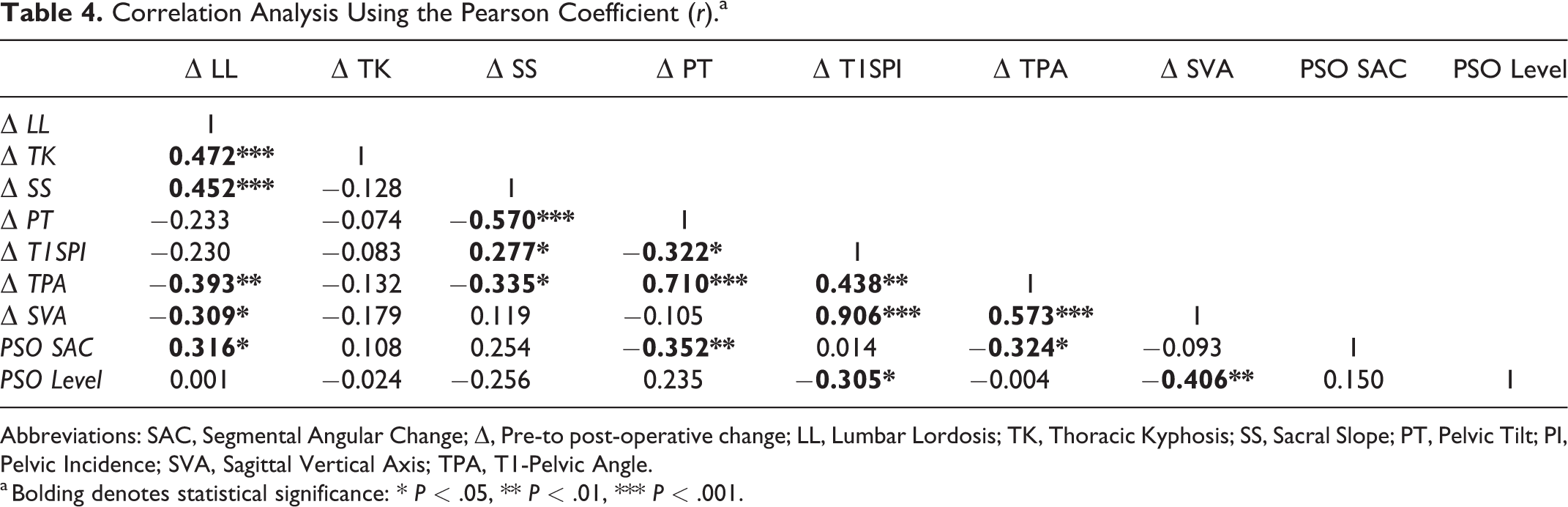
Abbreviations: SAC, Segmental Angular Change; Δ, Pre-to post-operative change; LL, Lumbar Lordosis; TK, Thoracic Kyphosis; SS, Sacral Slope; PT, Pelvic Tilt; PI, Pelvic Incidence; SVA, Sagittal Vertical Axis; TPA, T1-Pelvic Angle.
a Bolding denotes statistical significance: * P < .05, ** P < .01, *** P < .001.
PSO level was significantly correlated with T1SPI (r = −0.305, P = .026) and ΔSVA (r = −0.410, P = .002). Both of these relationships can be interpreted as a significantly greater correction of positive sagittal imbalance with more caudally performed PSO.
Additionally, ΔSVA was found to inversely correlate with ΔLL (r = −0.309, P = .024) and directly correlate with ΔT1SPI (r = 0.906, P < .001) and ΔTPA (r = 0.573, P < .001), suggesting that positive sagittal balance as measured by a decrease in SVA improved with increased LL and decreased T1SPI and TPA. There were significant correlations between ΔTPA and ΔLL (r = −0.393, P = .004), ΔTPA and ΔSS (r = −0.335, P = .014), ΔTPA and ΔT1SPI (r = 0.438, P = .001), as well as ΔTPA and ΔPT (r = 0.710, P < .001). In other words, increased LL and SS correlated with a greater improvement in TPA, whereas decreased PT and T1SPI directly correlated with decrease (improved) TPA.
Multivariate Analysis
A multivariate linear regression model was used to evaluate the overall effect of PSO SAC and PSO level on T1SPI, TPA, and SVA while controlling for age, BMI, the number of fusion levels, and whether the fusion was considered a long fusion (Table 5). PSO level was the only significant predictor for the magnitude of change in both T1SPI (β = −3.138, P = .009) and SVA (β = −29.030, P = .001). Clinically, this means that for each PSO level caudal to L1, the model predicted a greater improvement in T1SPI by approximately 3 degrees and a greater reduction in SVA by 29.03 mm, or approximately 3 cm.
Variables Significant on Multivariate Linear Regression Analysis Evaluating Independent Predictors of Change in T1SPI, TPA, and SVA.

Abbreviations: β, Unstandardized Coefficient; SE, Standard Error of β; CI, Confidence Interval of β; PSO, Pedicle Subtraction Osteotomy; T1SPI, T1-Spinopelvic Inclination; TPA, T1-Pelvic Angle; SAC, Segmental Angular Change; SVA, Sagittal Vertical Axis.
For change in TPA, significant predictors for a greater magnitude of change included PSO SAC (β = −0.375, P = .045) and the number of fusion levels (β = −1.427, P = .036). Clinically, this can be interpreted as an improvement in TPA by approximately 0.4 degrees for each additional degree of PSO and by 1.4 degrees for each additional level fused.
Complications
A total of 49 complications were recorded in 35 patients (66%) with no significant difference in overall complication rate by PSO level (P = .576), nor in the rates of early intraoperative/perioperative complications (P = .305), or late complications (P = .987) (Table 6). The most commonly observed early complication was intraoperative durotomy necessitating repair at a rate of 26.4%, whereas instrumentation failure with pseudarthrosis was the most common late complication seen among 28.3% of patients. Subanalysis of the frequencies of complication types revealed no significant differences by PSO level.
Early Intraoperative/Perioperative and Late Complications by Lumbar PSO Level.
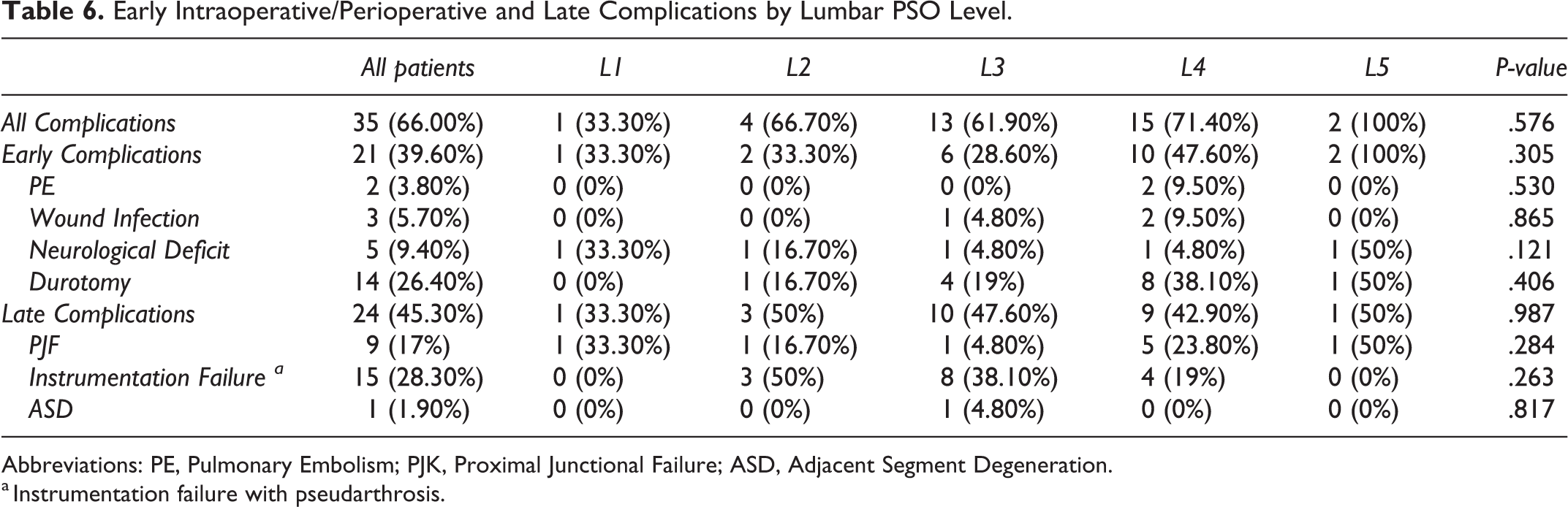
Abbreviations: PE, Pulmonary Embolism; PJK, Proximal Junctional Failure; ASD, Adjacent Segment Degeneration.
a Instrumentation failure with pseudarthrosis.
Discussion
With the establishment of surgical targets for sagittal correction in adult spinal deformity, increasing interest in corrective techniques has followed. The PSO is the most powerful spinal osteotomy aside from vertebral column resection and is commonly used in the correction of sharp or fixed kyphosis requiring correction of up to 30-40 degrees. However, despite the common use of the PSO, data regarding its impact on the sagittal profile and spinopelvic parameters is lacking. This study explored the impact of PSO level and SAC on global sagittal alignment, with specific emphasis on correction of SVA and TPA. Notably, more caudal PSO translated to greater correction in T1SPI and SVA by approximately 3 degrees and 3 cm, respectively, for each lumbar level caudal to L1, while a larger PSO SAC reduced TPA by approximately 0.4 degrees for each additional degree of osteotomy. Complications rates were similar at each PSO level.
This study is not without limitations. The retrospective nature of this analysis allows the possibility of selection bias. Additionally, this is a single-center study which could arguably limit the generalizability of its findings. However, the analysis did include patients from 3 different fellowship-trained spinal deformity surgeons who themselves trained at varying institutions. Furthermore, as this study included patients who had surgery over a 12-year period, there were likely advances in surgical techniques and technologies implemented into clinical practice which could not be controlled for. Lastly, increased study sample size could add further granularity to the data. However, in the literature on PSO a cohort of 53 patients is sizable, and significant findings were identified in our radiographic analysis indicating adequate power.
Recent years have seen increasing emphasis on the importance of the sagittal plane and its effect on outcomes and HRQOL measures in adult scoliosis. Prior work has suggested surgical targets for patient specific operative correction in order to optimize outcomes, and a LL within 10 degrees of PI has been shown to correlate with improved health-related-quality-of-life measures. 11 Similarly, derangements of SVA have been associated with worse patient outcomes, and the surgical goal of SVA < 50 mm has been recommended. 12 There has also been mounting evidence of the interrelation of the spinal column and the lower extremity in adult scoliosis.22,23 Other analyses have reported on the importance of PT as a reflection of pelvic compensation for sagittal imbalance, with increasing pelvic retroversion developing to maintain the center of gravity over the femoral heads with progressive loss of lumbar lordosis. 24 Further investigation of the interrelated nature of SVA and PT led to the reporting of TPA as a single parameter combining both sagittal axis derangement and pelvic compensation. 25
To date, the most robust study investigating the relationship between PSO vertebral level, degree of PSO, and spinopelvic and sagittal correction has been a multicenter study by Lafage et al reporting the outcomes in a series of 70 patients. 18 The authors reported that PSO SAC correlated with correction of spinopelvic parameters, including LL, TK, SS, and PT. They also reported that while PSO level did affect PT, it did not affect SVA. As the authors of that study acknowledged, these findings are somewhat counterintuitive to expectations as, based upon simple trigonometric calculations, one would anticipate a greater SVA correction with a more caudal osteotomy.19,20,26 They suggested that further investigation of this phenomenon was merited.
This analysis sought to build on prior work to assess the relationship between spinal level of PSO, degree of PSO osteotomy, and spinopelvic parameters in a large cohort at a single institution. Similar to past findings, PSO SAC significantly correlated with correction of LL and PT, although no correlation was found with TK and SS among this study’s cohort. Moreover, PSO SAC correlated with change in TPA, a relationship which was previously unexplored. This finding was further investigated via multivariate analysis, which found that larger osteotomy translated to a greater reduction, and therefore improvement, in TPA of approximately 0.4 degrees per additional degree of osteotomy. Contrary to the findings of Lafage et al, this study also found a significant relationship between PSO level and correction of sagittal balance, with approximately 3 degrees of further correction in T1SPI and 3 cm in SVA with each level of more caudal osteotomy.
Since T1SPI is the angular equivalent of SVA in measuring positive sagittal balance, the 2 are highly interrelated (r = 0.906). Therefore, as might be expected, the level of PSO directly affected the magnitude of correction in both measurements. Conversely, despite the strong correlations between T1SPI and TPA (r = 0.438) and SVA and TPA (r = 0.573) both among this study’s patients and in the literature, 27 there was no correlation found between PSO level and TPA. Conversely, correlations were found between PSO SAC and TPA, but not SAC and T1SPI or SVA. While this may seem counterintuitive at first, it is likely attributed to the inherent relationship between TPA and PT (r = 0.710) since TPA is an angular measurement combining both PT and T1SPI. 27 Given that there was a trend toward a lesser reduction in PT with more caudal PSO in this analysis (r = 0.235, P = .091), it is likely that the inverse effects of PSO level on T1SPI and PSO level on PT canceled each other out. On the other hand, a larger PSO SAC significantly correlated with a greater postoperative reduction of PT and TPA, thus reducing compensatory pelvic retroversion, but had no significant effect on T1SPI or SVA. This suggests that a larger angle of osteotomy may contribute more substantially to sagittal pelvic orientation than to the alignment of the spinal column.
The results of this analysis stand in contrast to the results reported by Lafage et al which did not identify an association between PSO level and correction of SVA. 18 This correlation is somewhat intuitive and expected given trigonometric calculations which would predict increasing SVA correction with a more caudal PSO. It is possible that this discrepancy between this analysis and the findings of Lafage is secondary to the changes in PT and TK. The authors of the prior analysis postulated that their findings of variable degree of post-osteotomy PT change, with more caudal PSO levels resulting in greater reduction of PT, may have offset the change in SVA. This is in stark contrast to the findings of the present study, which found a trend toward a lesser reduction in PT with more caudal PSO (r = 0.235, P = .091). Furthermore, Lafage et al identified an increase in TK correlated with PSO SAC that this analysis did not identify. That increase in TK could have dampened the improvement in SVA in that analysis. Given that there were a greater percentage of long fusions in the prior study, it is possible that the increase in TK was associated with surgical correction via the more cephalad extent of fusion, which was not controlled for. Considering the discrepancies in the findings between this study and those previously reported by the 70 patient, multicenter analysis by Lafage et al, another larger multicenter study could be indicated to add further validation to this and prior work.
While the findings of this study demonstrate improved correction with more caudal osteotomy, the choice of vertebral level for lumbar PSO should be tailored to the patient’s specific clinical situation. For example, the surgeon should consider the underlying cause of the imbalance (particularly in the presence of focal kyphotic deformity), levels of prior surgery / scar, and other factors such as local anatomy. Specifically, more cephalad PSO at L1 or L2 poses a risk for injury to the conus medullaris. Osteotomies at L3 may place the L3 nerve at risk, which is arguably more morbid than lower level nerve palsies due to poor patient tolerance of quadriceps palsy. On the other hand, more caudal osteotomies often necessitate that the fusion be extended to include the pelvis, thus increasing the risk for complications such as instrumentation failure, proximal junctional failure, and nonunion. 28 Lastly, osteotomies at L5 are considered more challenging due to the lordotic angle of L5 and the unique morphology of the pedicles. Despite these level-dependent considerations and challenges, no differences were found in the rates of any complications by PSO level. However, future large-scale prospective studies will need to address the relationships between PSO level, alignment parameters, complications, and outcome measures.
Conclusion
Increasing focus on the sagittal component of adult spinal deformity and the complexity of spinopelvic relationships has led to growing interest in the predictability of surgical techniques available for operative management of sagittal imbalance. This analysis identified significant correlations between PSO SAC and the magnitude of correction in TPA, as well as PSO level and correction in SVA and T1SPI. Specifically, larger PSO SAC significantly predicted an additional 0.4 degrees of correction for each degree of added osteotomy. Lumbar PSO level significantly predicted greater improvement in T1SPI and SVA, quantified by an increase of roughly 3 degrees and 3 cm of correction, respectively, for each lumbar level below L1. These findings could serve as a guide for operative planning.
Footnotes
Authors’ Note
All co-authors have seen and agree with the contents of the manuscript. Each author certifies that his or her institution approval the reporting of this investigation (ORA 21 031 201) and that all investigations were conducted in conformity with ethical principles of research. The manuscript submitted does not contain information about medical device(s)/drug(s). This work was performed at Rush University Medical Center, Chicago, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.