
Abstract
Purpose:
Dropped head syndrome (DHS) is characterized by the passively correctable chin-on-chest deformity. The characteristic feature is emphasized in the cervical flexion position. The purpose of this study was to analyze the influence of cervical flexion on sagittal spinal alignment in patients with DHS.
Methods:
The study included 15 DHS subjects and 55 cervical spondylosis (CS) subjects as the control group. The following parameters were analyzed: cervical sagittal vertical axis (C-SVA), occipitoaxial angle (O–C2A), C2 slope (C2S), C2–C7 angle (C2–C7A), T1 slope (T1S), sagittal vertical axis, T1–T4 angle (T1–T4A), T5–T8 angle (T5–T8A), T9–T12 angle, lumbar lordosis, sacral slope, and pelvic tilt, in cervical flexion and neutral positions.
Results:
The values of C-SVA, O–C2A, C2S, and T1S were significantly different between CS and DHS at cervical neutral and flexion positions. C2–C7A showed significant difference in cervical neutral position, but the difference disappeared in flexion position. T1–T4A did not present a significant difference, but T5–T8A showed a difference in neutral and flexion positions.
Conclusions:
Malalignment of DHS extended not only to cervical spine but also to cranio-cervical junction and thoracic spine, except T1–T4. It is known that global sagittal spinal alignment is correlated with adjacent parameters, although in DHS the reciprocal change was lost from cranio-cervical junction to the middle part of thoracic spine at cervical flexion.
Keywords
Introduction
Dropped head syndrome (DHS) is a relatively rare condition that shows characteristic kyphotic posture without maintaining neutral position. The kyphotic deformity of DHS, which gradually progresses after upright posture with cervical extensor muscle weakness, severely impairs quality of life of individuals by causing various degrees of clinical disorders including neck pain, horizontal fixation difficulties, neurological symptoms, dysphagia, and gait disorders. 1 –3 In the supine position, the deformity becomes reduced. In contrast, cervical kyphotic deformities due to degenerative ankylosing spondylosis could not be greatly changed by cervical posture. 1,3 The characteristic dropped head feature is emphasized at cervical flexion, which is correctable even at the upright position in a short time, and therefore analysis of sagittal spinal alignment at cervical flexion is important for evaluating cervical deformity in DHS (Figure 1). There is controversy regarding the sagittal alignment of DHS, which is essential for understanding the pathophysiology and for planning treatment including corrective surgery. Previously, the evaluation of DHS sagittal alignment has been commonly based on cervical sagittal X-ray findings. 4 Cervical sagittal alignment was affected by global sagittal spinal alignment, 5 and some recent studies regarding DHS were based on analysis of global spinal sagittal alignment. 6 –8 The purpose of this study was to analyze the influence of cervical flexion on global sagittal spinal alignment in patients with DHS.

Representative photographs of DHS patients. (a) Neutral position and (b) flexion position. DHS: dropped head syndrome.
Materials and methods
Fifteen DHS (average age 71.7 years, 7 males and 8 females) and 55 cervical spondylosis (CS) cases without global sagittal spinal alignment deformity 5 (CS, average age 49.1 years, 42 males and 13 females) who visited our institute between January 2016 and September 2017 and who had whole spine X-ray in cervical flexion and neutral positions without assistance were enrolled in our study (Table 1). Subjects with a history of neuromuscular disease, trauma, infection, tumor, inflammatory disease, ossification, or cervical deformities 9 as well as those having undergone spinal surgery were excluded. DHS was defined as follows: (1) The patient showed chin-on-chest deformity in the natural position and had difficulty maintaining a horizontal gaze at upright position for a few minutes and (2) the deformity was correctable in the supine position. 1 For the direct comparison between DHS and CS groups, “neutral position” in DHS patients in this study was defined as the posture of the DHS patients’ cervical neutral position before the onset of DHS as much as possible, which may not be “neutral” position for DHS patients, though. The following global spinal radiographic parameters were measured in the standing position by computer association as described previously 10 –14 : total distance from plumb line of pedicle center of C2 vertebra to posterior superior corner of C7 vertebra (cervical sagittal vertical axis (C-SVA)), distance from C7 plumb line to sacral posterior angle (sagittal vertical axis (SVA)), angle between McGregor’s line and the inferior endplate of C2 (occipitoaxial angle (O–C2A)), angle between C2 lower endplate and horizontal plane (C2 slope (C2S)), cervical lordosis assessed by C2–C7 angle (C2–C7A), which was defined as the angle from lower endplate of C2 to lower endplate of C7 (C2–C7A), angle between T1 upper endplate and horizontal plane (T1 slope (T1S)), angle between T1 upper edge and T4 lower edge (T1–T4 angle (T1–T4A)), angle between T5 upper edge and T8 lower edge (T5–T8 angle (T5–T8A)), angle between T9 upper edge and T12 lower edge (T9–T12 angle (T9–T12A)) (see Figure 2), angle from upper endplate of L1 to upper endplate of sacrum (lumbar lordosis (LL)), angle between sacral plate and horizontal plane (sacral slope (SS)), and angle between line connecting midpoint of sacral plate to axis of femoral head and gravity line (pelvic tilt (PT)) in cervical flexion and neutral positions. Whole spine anteroposterior and lateral radiographs were obtained using the digital slot-scanning radiography mode of SONIALVISION safire fluoroscopy (Shimadzu Corp., Kyoto, Japan) in both cervical flexion and neutral positions and the differences between the parameters between cervical flexion and neutral positions were compared. The intraobserver and interobserver agreement rates of the measurements by this system have been described previously. 13 This study was approved by the Ethics Review Board of our institution. Values were expressed as mean ± standard deviation. Statistical analyses were performed using the JMP software package version 10.0 (SAS Institute Inc., Cary, North California, USA). t-Tests were used to determine intergroup differences between cervical flexion and neutral positions to analyze the outcome measures of parameters in sagittal spinal alignment. Correlations between the variables of spinopelvic parameters were analyzed by Pearson rank correlation coefficient. A p value <0.05 was considered to indicate a statistically significant difference between two groups.
Patient characteristics.

CS: cervical spondylosis; DHS: dropped head syndrome.
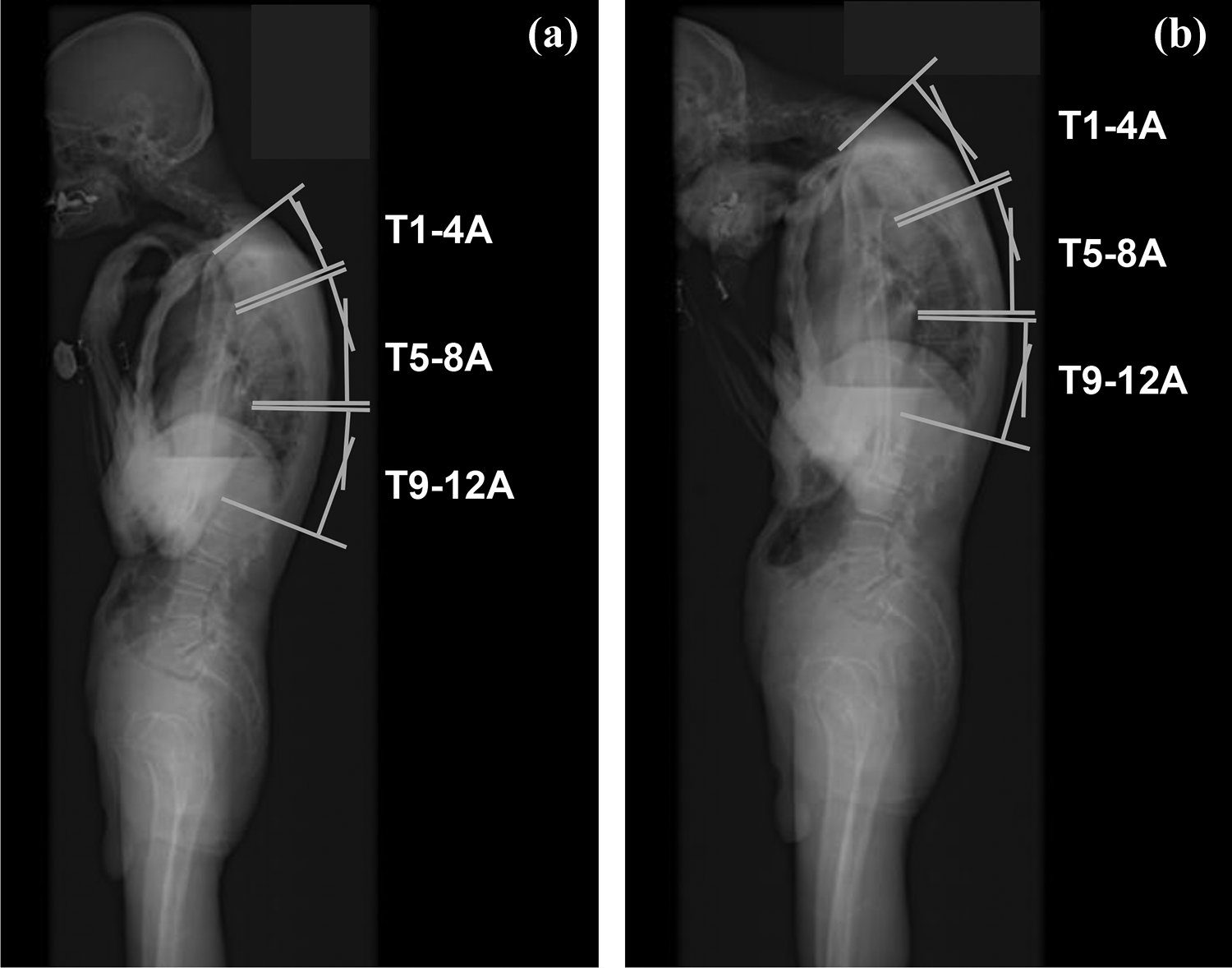
Representative X-ray images and thoracic angle measurement: (a) neutral position and (b) flexion position. T1–T4A: T1–T4 angle; T5–T8A: T5–T8 angle; T9–T12A: T9–T12 angle.
Results
The characteristics of DHS was elder and more female than CS (Table 1). The cervical range of motion of CS and DHS was 50.2 ± 28.2° and 28.6 ± 20.2°, respectively. The values of C-SVA, O–C2A, C2S, and T1S were significantly different between CS and DHS in cervical neutral and flexion positions. The C2–C7A showed significant difference in cervical neutral position, but the difference disappears in flexion. T1–T4A did not present a significant difference, but T5–T8A showed a difference in the neutral and flexion positions between CS and DHS. T9–T12A showed only a difference in cervical flexion position. PT in DHS was significantly larger in cervical neutral and flexion positions than CS (Table 2).
Sagittal spinal parameters of CS and DHS patients in neutral and flexion positions.a

CS: cervical spondylosis; DHS: dropped head syndrome; C-SVA: cervical-sagittal vertical axis; SVA: sagittal vertical axis; O–C2A: occipitoaxial angle; C2S: C2 slope; C2–C7A: C2–C7 angle; T1S: T1 slope; T1–T4A: T1–T4 angle; T5–T8A: T5–T8 angle; T9–T12A: T9–T12 angle; LL: lumbar lordosis; SS: sacral slope; PT: pelvic tilt.
aIn this study, a p value <0.05 was considered to indicate a statistically significant difference between two groups.
bindicates p < 0.05.
Regarding the correlation between C2–C7A and other adjacent spinal parameters, in CS, C2–C7A correlated with T1S and T5–T8A in cervical neutral and flexion positions, but it did not correlate in DHS. The correlation of C2–C7A with O–C2A was retained in cervical neutral position, but it disappeared in cervical flexion position (Table 3).
Correlation between C2–C7A and thoracic sagittal alignment in neutral and flexion positions.a

C2–C7A: C2–C7 angle; CS: cervical spondylosis; DHS: dropped head syndrome; O–C2A: occipitoaxial angle; C2S: C2 slope; T1S: T1 slope; T1–T4A: T1–T4 angle; T5–T8A: T5–T8 angle; T9–T12A: T9–T12 angle.
aIn this study, a p value <0.05 was considered to indicate a statistically significant difference between two groups.
b(): p Value.
cindicates p < 0.05.
Discussion
The malalignment of DHS extends not only to the cervical spine but also to the cranio-cervical junction and thoracic spine as well as lumbopelvic spine. This study showed the correlation of C2–C7A with O–C2A maintained at cervical neutral position in DHS, but this was lost at cervical flexion position (Table 3), which relates to the evidence that clinical symptoms caused by DHS is found more clearly at cervical flexion. 1 –3 Regarding thoracic sagittal alignment, which affects cervical sagittal alignment, 15,16 the T1S and T5–T8A were correlated with C2–C7A at cervical neutral and flexion positions in CS but not in DHS (Table 3), suggesting that the reciprocal change of cervicothoracic spine was lost in DHS. The global sagittal alignment was maintained (SVA < ±40 mm 17 ) in both CS and DHS patients (Table 2), indicating that the spinopelvic harmony was not altered in both groups.
The present results showed that T1–T4A did not differ between DHS and CS in cervical neutral and flexion positions (Table 2). Thoracic spine is involved in approximately 33% of cervical flexion and 21% of cervical rotation and is closely associated with cervical movement 18 ; nevertheless, T1–T4A was not correlated with C2–C7A in neutral and flexion positions in this study (Table 3). Because T1–T4 is included in strongly constructed shoulder girdle (scapula bone and rhomboid muscles). Rhomboid minor and major muscles are located from the scapula to C7–T5. 19 These results would provide useful information for physiotherapy and corrective surgery for DHS. There have been various discussions about surgical strategies for DHS, and recent studies demonstrated that there are at least types of DHS classified by sagittal imbalance in cervical alignment and global alignment. 6 –8 Differences in the type of DHS may impact on surgical strategies for corrective surgery. When posterior cervical reconstruction surgery for DHS with cervical imbalance is performed, 6 –8 T1–T4 may provide suitable bone anchorage for the distal end of vertebrae. 1,20 Considering that reciprocal change of the cranio-cervical region was maintained at cervical neutral position, but was lost at cervical flexion position in DHS patients, the cephalic end of cervical fixation for DHS may not be needed to include the occipital region. Indeed, there have been no reports regarding the case that the occipital region as cephalic end for posterior cervical reconstruction surgery for DHS, yet various symptoms caused by DHS were improved in the previous reports. 2,3 Taken together, the measurement of global sagittal alignment at cervical flexion would be useful for decision-making and surgical planning by the physician caring for patients with DHS.
This study has some limitations. (1) The number of subjects was relatively small due to the rare appearance of DHS. 1 –3 (2) Global sagittal spinal alignment was not divided into the following two types: SVA+ and SVA− 7,21 due to the sample size. Previous studies reported that there were no significant differences of global sagittal spinal parameters except SVA between SVA+ and SVA− in DHS. 7 (3) CS could not fit age match to DHS because the patients were enrolled at the same period.
Conclusions
Malalignment of DHS extended not only to cervical spine but also to cranio-cervical junction and thoracic spine except T1–T4. It is known that global sagittal spinal alignment is correlated with adjacent parameters, although in DHS the reciprocal change was lost from cranio-cervical junction to the middle part of thoracic spine at cervical flexion.
Footnotes
Acknowledgments
We are indebted to Mr Arndt Gerz for the editorial review of the English manuscript. Advice and comments given by him have been of great help to us. Yuri Amamizu of the Department of Orthopedic Surgery assisted with the preparation of the initial English manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.