
Abstract
Purpose
Pseudoarthrosis and metal failure at L5-S1 following long fusion surgery for adult spinal deformity (ASD) remain major issues. Few studies report on which anterior column support technique is better in terms of achieving fusion and avoiding metal failures. Our study aimed to evaluate the fusion status and metal failure rate at L5-S1 after anterior lumbar interbody fusion (ALIF) versus transforaminal lumbar interbody fusion (TLIF).
Methods
The study population included patients aged >50 years who underwent surgery for ASD. Anterior column supports at L5-S1 using ALIF and TLIF were compared with ≥ 2-year follow-up. Fusion status on 2-year computed tomography (CT) scan, metal failure, visual analog scale (VAS), and Oswestry disability index (ODI) were evaluated.
Results
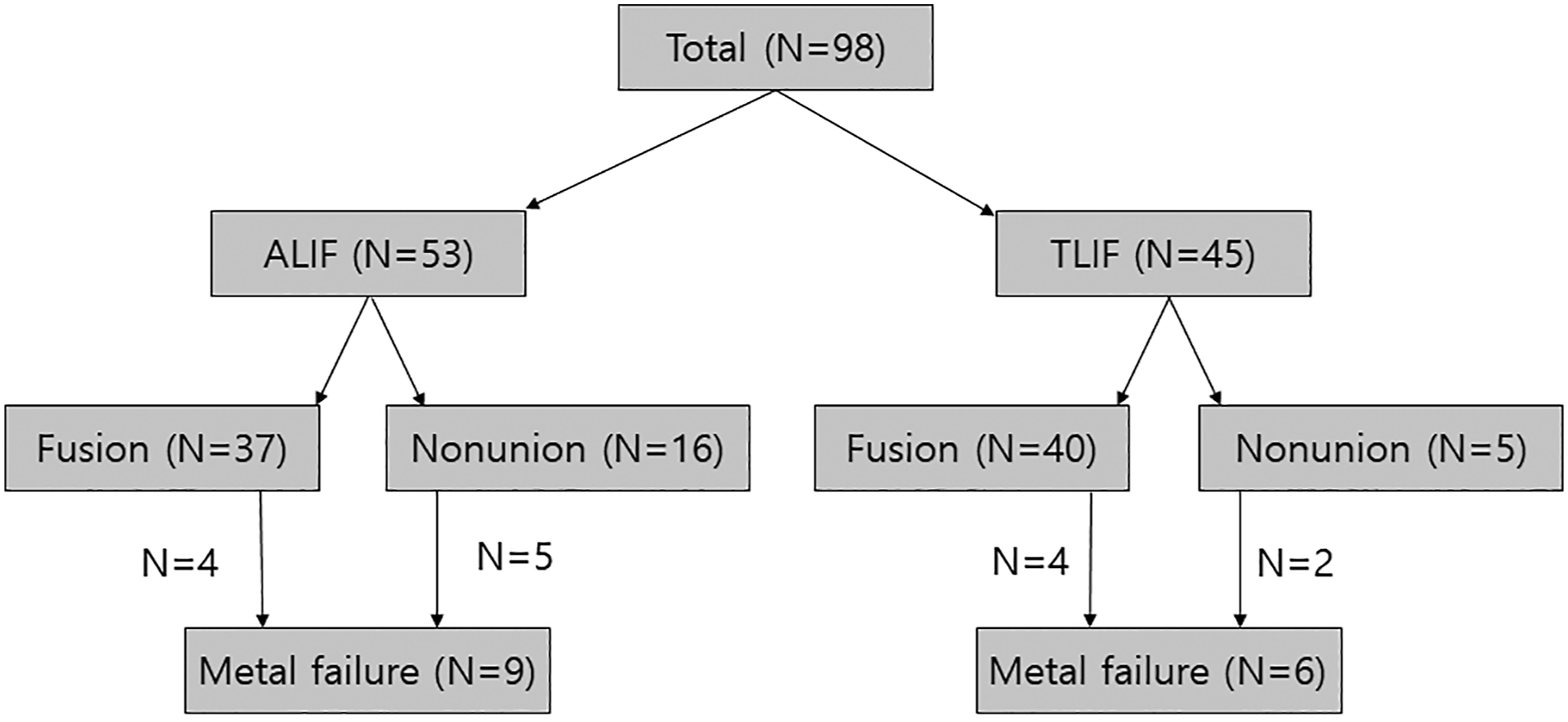
98 patients were included in this study (53 ALIF group and 45 TLIF group). We achieved solid fusion on 2-year CT scans in 88.9% and 69.8% patients in the TLIF and ALIF group, respectively. Metal failure developed in nine (17.0%) and six (13.3%) patients in the ALIF and TLIF group, respectively. The most common failure type was unilateral L5-S1 rod fracture (7 and five patients in the ALIF and TLIF group, respectively). Only one patient with bilateral rod fractures in the ALIF group required revision surgery. There were no differences in the VAS and ODI scores at the last follow-up.
Conclusions
TLIF showed a better fusion rate than ALIF at L5-S1 after long instrumented fusion for ASD. However, the capacity to restore sagittal parameters was greater in the ALIF group. There were no differences between the groups regarding metal failure rate, revision surgery, or clinical outcomes.
Keywords
Introduction
The goal of adult spinal deformity (ASD) surgery is to restore the optimal sagittal balance and achieve solid arthrodesis. Achieving solid fusion at the lumbosacral junction, L5-S1, remains a challenge, especially in a long instrumented fusion to the sacrum.1-4 The L5-S1 segment has unique anatomical characteristics such as poor bone quality of the sacrum, complexity of the sacral anatomy, and an anterior inclination. This makes the fixation at the lumbosacral junction potentially weak during the fusion process, thereby increasing the risk of pseudoarthrosis at this segment.5-7 Long fusion itself also increases the lever arm and moment force at the L5-S1.8, 9 Currently, sacropelvic fixation is a widely accepted technique to achieve solid fusion at the L5-S1 by protecting S1 screws.10-16 As in the sacropelvic fixation, the anterior column support at L5-S1 is also recommended to reduce mechanical failures at the lumbosacral junction.1, 11, 17-19 Thus, sacropelvic fixation combined with anterior column support has become the current standard to avoid lumbosacral pseudoarthrosis and mechanical failures after long instrumented fusion.
Anterior column support at L5-S1 can be performed through an anterior approach using anterior lumbar interbody fusion (ALIF) or a posterior approach using transforaminal lumbar interbody fusion (TLIF). It is well known that ALIF has an advantage over TLIF in terms of better restoration of disc angle (DA) and lumbar lordosis (LL) through a complete anterior release.1, 20 ALIF also facilitates a more thorough preparation of the disc space under direct visualization. This affords a larger cage or graft with a broad contact area. Theoretically, for that reason, we can expect better fusion and subsequent lower metal failure rates at L5-S1 after ALIF compared to TLIF. However, few studies have compared the results of these two fusion methods at L5-S1, especially in long fusion surgery for ASD. Therefore, the primary aim of this study was to compare the fusion status and metal failure rate at L5-S1 after ALIF and TLIF. The second aim was to compare the deformity correction capacity in the sagittal plane between ALIF and TLIF.
Materials and methods
Study population
This study was approved by the institutional review board (IRB) of our institution. The need for informed consent was waived because of the retrospective nature of this study. We retrospectively reviewed radiographic and clinical data retrieved from the center’s prospective ASD database. The study population included consecutive patients treated between 2009 and 2018, who were older than 50 years, who had undergone a greater than 4-level fusions to the sacrum with iliac screws and anterior column support at L5-S1 for ASD, and who had been followed up for more than 2 years. The primary reasons for surgery were sagittal imbalances with progressive back pain, either with or without neurogenic claudication, which were unresponsive to nonoperative treatment. All patients included in the study met at least one of the following radiographic criteria: 1) sagittal vertical axis (SVA) ≥ 50 mm, 2) pelvic incidence-lumbar lordosis mismatch (PI-LL) >10°, 3) pelvic tilt (PT) >25°, or 4) LL <30°.21, 22 Patients who had undergone previous L5-S1 fusion surgery were excluded. We also excluded patients with neuromuscular scoliosis, ankylosing spondylitis, postoperative surgical infection, or those who had been followed up for less than 2 years. We created two groups, an ALIF and a TLIF group, according to the fusion technique used at L5-S1.
Surgical details
All L5-S1 levels were treated with interbody fusion using ALIF or TLIF. In our institution, we prefer ALIF over TLIF for treating the L5-S1 segment, especially in long instrumented fusion for ASD. However, in case of an unsuitable major vessel anatomy, a history of abdominal surgery, or severely obese patients, the surgeons performed TLIF instead of ALIF. All ALIF surgeries were performed via the retroperitoneal approach, with the surgical corridor between the right and left common iliac vessels. Polyetheretherketone (PEEK) cages (Perimeter® from Medtronic or Syncage® from Depuy Synthes) filled with allogenous chip bone graft plus demineralized bone matrix (DBM) were used in all ALIF surgeries. No additional bone grafts were placed around the cage. For TLIF surgery, one (boomerang type) or two (bullet type) titanium cages filled with autologous bone graft plus DBM were used. The bone graft was packed around the cage as much as possible. An allogeneic chip bone graft was used when the local bone was insufficient to fill the disc space.
Evaluation of fusion on CT
We obtained 3D reconstructed CT scans of sagittal and coronal images. For all patients, we routinely performed 3D CT to assess fusion attainment at 2 years postoperatively. However, CT was performed earlier for four patients who had experienced a metal failure within 2 years (17.9, 18.0, 18.7, and 20.0 months, respectively). We evaluated the fusion status at L5-S1 on CT images and classified them based on the Brantigan, Steffee, and Fraser (BSF) criteria as follows (Figure 1)
23
: pseudarthrosis (grade 1) is indicated by significant resorption of the bone graft or visible lucency around the periphery of the graft or cage. Locked pseudarthrosis (grade 2) is indicated by visible lucency only in the middle of the cages, with solid bone growing into the cage from each vertebral endplate. Fusion (grade 3) is indicated by bone bridges covering at least half of the fusion area. In this study, we considered grade 3 as a fusion and grade 1 or 2 as a nonunion. Coronal and sagittal CT images according to BSF criteria
Preoperative, intraoperative, and postoperative variables
Demographic variables included age, sex, smoking status, American Society of Anesthesiologists (ASA) grade, diabetes mellitus (DM), body mass index (BMI, kg/m2), and osteoporosis. Intraoperative variables included interbody fusion number, total fusion level numbers, prior fusion surgery other than L5-S1, and pedicle subtraction osteotomy (PSO).
We evaluated metal failure developing at L5-S1 on routine follow-up plain radiographs. In this study, we observed two types of metal failure: rod fractures between L5 and S1 screws and concurrent loosening of S1 and iliac screws. We excluded other metal failures that developed below the S1 screw, such as rod fractures between the S1 and iliac screws or isolated iliac screw fractures. We excluded these from the analysis because these failures are known not to be related to lumbosacral pseudoarthrosis, but the mobility of the sacroiliac joint, and are considered to be minor failures that do not deteriorate the clinical outcomes.24, 25 Because the follow-up duration was significantly longer in the TLIF group, we had to consider the time to calculate the metal failure rate. Thus, in this study, we performed Kaplan–Meier survivorship analysis with the log-rank test to calculate and compare the metal failure-free probability between the ALIF and TLIF groups.
We measured sagittal parameters, including pelvic incidence (PI), LL, PI-LL, sacral slope (SS), PT, thoracic kyphosis (TK), and SVA preoperatively and at the 2-year follow-up. To evaluate the local radiographic change at the L5-S1 segment, we measured the disc height and DA. We defined DA as the angle between the two lines parallel to the lower endplate of L5 and the upper endplate of S1. We measured DH using the vertical distance between the midpoints of the upper and lower endplates. When the SVA was less than 50 mm, we considered the correction to be optimal.26, 27 To evaluate the correction loss during follow-up, we again measured LL, DA, and DH at the final follow-up. Clinical assessments were performed using the visual analog scale (VAS) for back pain and Oswestry disability index (ODI). We measured and compared the VAS and ODI preoperatively and at the final follow-up. The minimal clinically important difference (MCID) for ODI was set at 15 points.
Statistical analysis
Data are presented as frequencies with percentages for categorical variables and means with standard deviations for continuous variables. Fisher’s exact test was used to compare the categorical variables. For comparison between two groups, Student’s t-test was used for continuous variables with normality and the Mann–Whitney test for continuous variables without normality. Statistical analyses were performed by professional statisticians using SPSS software (version 25.0.0; SPSS Inc., Chicago, IL, USA). A p value less than 0.05 were considered statistically significant.
Results
Demographic and baseline data.

Data are presented as the mean ± SD or as the number of patients (percentage).
ALIF, anterior lumbar interbody fusion; TLIF, transforaminal lumbar interbody fusion, ASA, American Society of Anesthesiologists; DM, diabetes mellitus, BMI, body mass index; PSO, pedicle subtraction osteotomy; PI, pelvic incidence; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; SVA, sagittal vertical axis; DA, disc angle; DH, disc height.
Bold p values indicate statistical significance.
Comparison of fusion and metal failure between two groups.

Data are presented as the mean ± SD or as the number of patients (percentage).
ALIF, anterior lumbar interbody fusion; TLIF, transforaminal lumbar interbody fusion.
Bold p values indicate statistical significance.
† Grade 1 indicates pseudoarthrosis, grade 2 locked pseudoarthrosis, and grade 3 fusion. Grade 1 and 2 were considered as nonunion in this study.
‡ Survival time to failure was compared using Kaplan–Meier survivorship analysis with log-rank test.

Kaplan–Meier survivorship curve. Kaplan–Meier survivorship curve showing the metal failure-free probability.
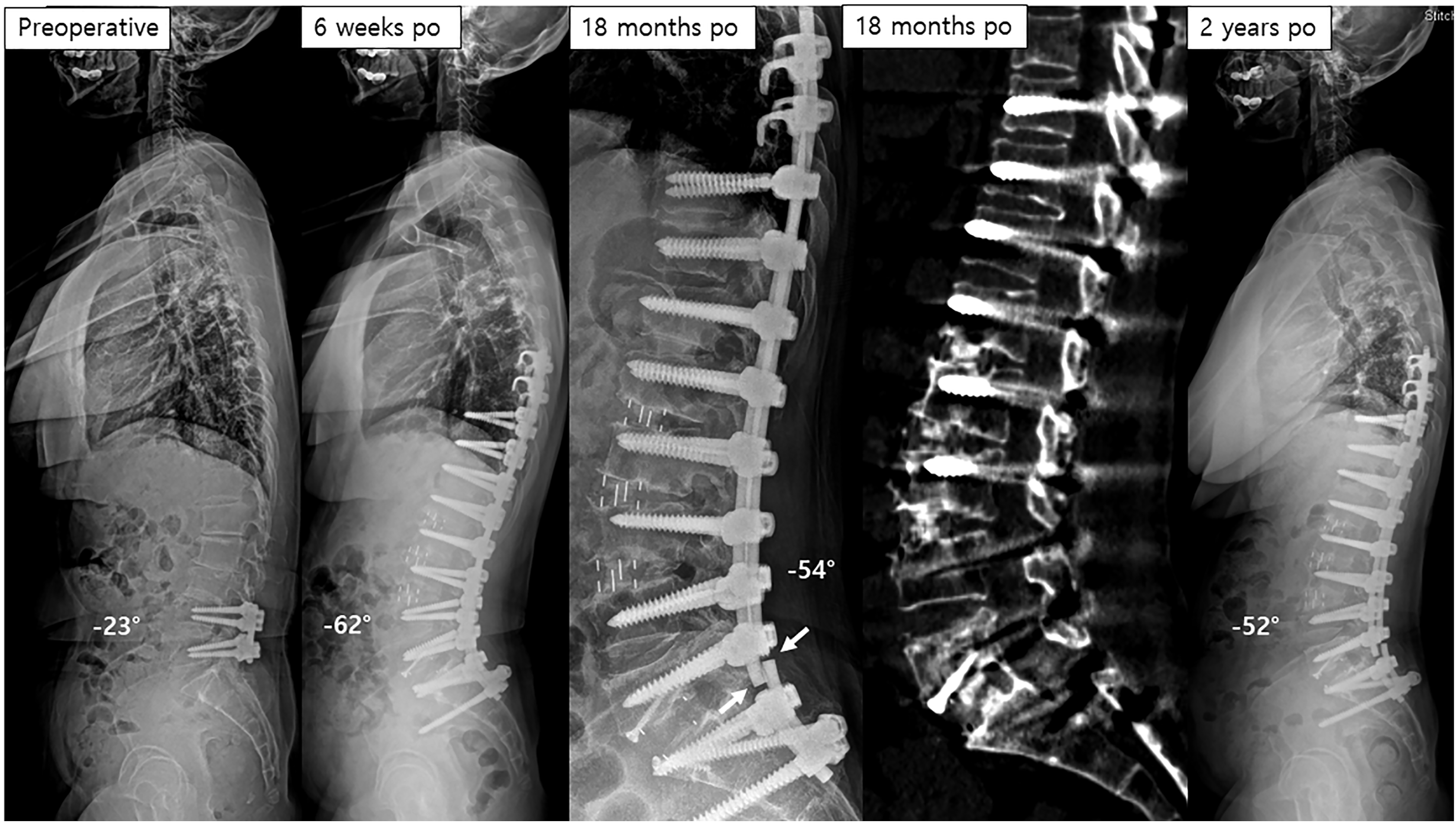
Case illustration

Case illustration
Comparison of clinical outcomes.

Data are presented as the mean ± SD or as the number of patients (percentage).
ALIF, anterior lumbar interbody fusion; TLIF, transforaminal lumbar interbody fusion; VAS, visual analog scale; ODI, Oswestry disability index; MCID, minimal clinically important difference.
Bold p values indicate statistical significance.
Comparison of postoperative radiographic parameters.
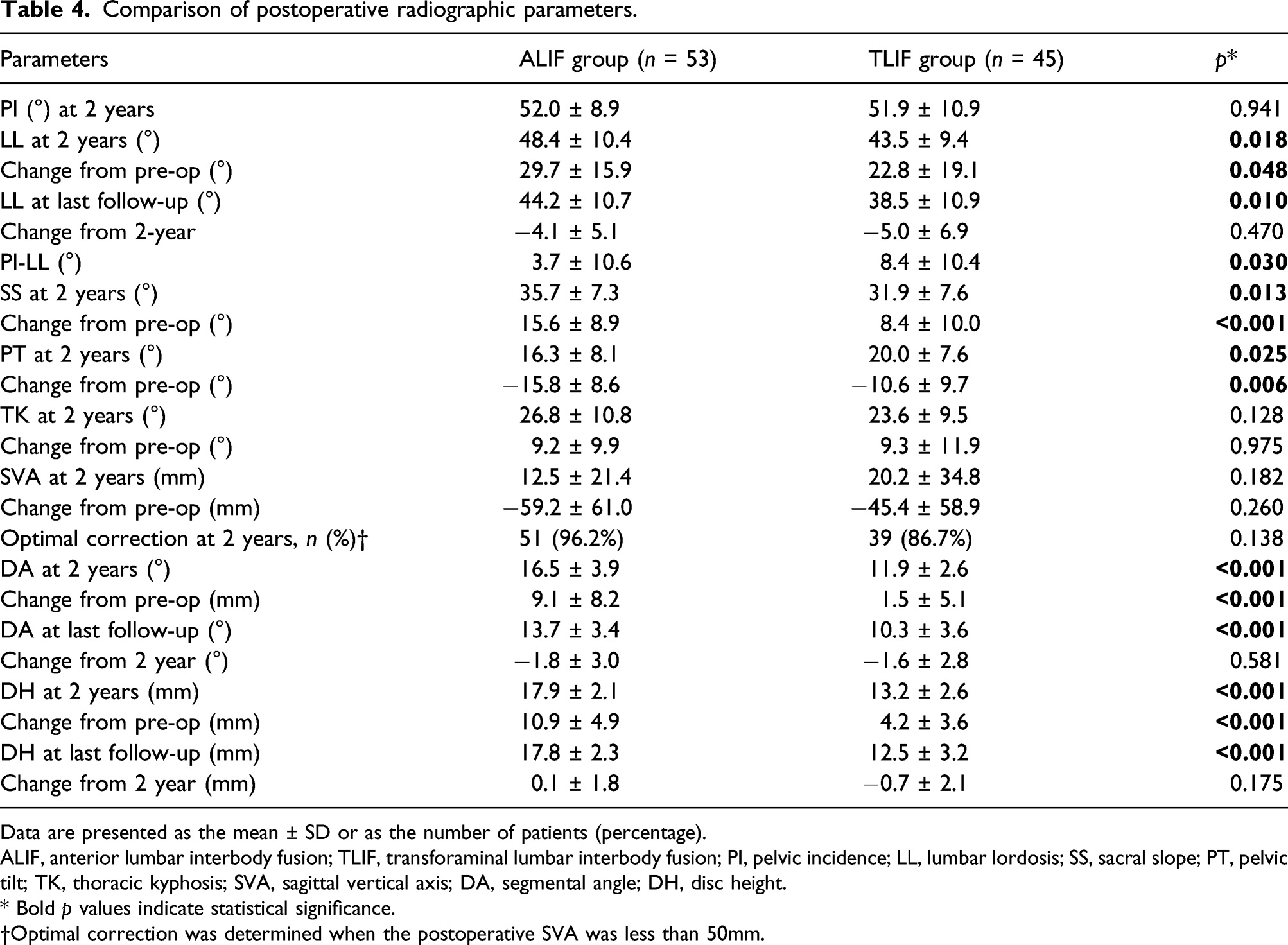
Data are presented as the mean ± SD or as the number of patients (percentage).
ALIF, anterior lumbar interbody fusion; TLIF, transforaminal lumbar interbody fusion; PI, pelvic incidence; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; TK, thoracic kyphosis; SVA, sagittal vertical axis; DA, segmental angle; DH, disc height.
* Bold p values indicate statistical significance.
†Optimal correction was determined when the postoperative SVA was less than 50mm.
Discussion
In long fusion surgery, including the sacrum for ASD, one should pay special attention to the L5-S1. Because the junction is anatomically weak and the long arm lever causes great moment, the L5-S1 segment is always vulnerable to mechanical complications, such as pseudoarthrosis or metal failure.8-12 Numerous studies have confirmed the preventive effects of combined spinopelvic fixation with anterior support against these mechanical complications at the L5-S1.11, 17-19, 25, 28 Unlike a number of studies on the role of pelvic fixation, there is little literature studying the interbody fusion method for anterior column support at L5-S1 in long fusion surgery. Thus, we carried out a comparative study between ALIF and TLIF at the caudal segment, focusing on fusion and mechanical failures.
A better fusion rate is one of the hypothetical advantages of ALIF over TLIF surgery by preparing disc space more thoroughly under direct visualization and by affording a larger cage. In contrast, in the present study, CT revealed that the proportion of fusion grade 3 was significantly higher in the TLIF group (88.9%) than in the ALIF group (69.8%). However, as there are differences between the two patient groups other than the surgical approach, it is difficult to simply compare the fusion rate.
First, the materials and volume of the bone graft were different between the two techniques. Only allogenic bone grafts, such as bone chips and DBM, were used in ALIF surgery, while morselized autologous bone grafts from the lamina or facet joints were used in addition to allogenic bone grafts in TLIF surgery.
The volume of the bone graft is related to disc space fulfillment. The bone graft volume is usually smaller in ALIF than in TLIF. However, the ALIF cage is usually larger than the TLIF cage, so the intervertebral disc space coverage or fulfillment of the cage and bone graft might not differ significantly between the two groups. The second reason could be the difference of the cage material. The cages used for ALIF surgery were made of PEEK, while the cages for TLIF were made of titanium. The usefulness of PEEK and titanium cages for spinal fusion remains debatable. It is known that the PEEK cage is equivalent to that of the elastic modulus of bone, which can prevent cage subsidence and promote fusion, and studies have reported a higher fusion rate than titanium. 29 30 However, in the case of animal studies or in vitro studies, there are studies related to the disadvantages of PEEK cage in relation to fusion. Some authors have reported that PEEK cages limit direct cell adhesion on PEEK implant surfaces, resulting in fibrous tissue surrounding the implant surface. 31 32 In comparison with titanium, it was also observed in PEEK that suppression of osteoblastic differentiation of mesenchymal stem cells and activation of inflammatory response was seen. 33 34 Moreover, recent studies have reported that titanium cages are more effective than PEEK cages in achieving a solid interbody fusion. Nemoto et al. 35 studied CT data from 50 patients who underwent one-level TLIF, using local bone graft materials, and reported that the titanium cage group showed a higher fusion rate than the PEEK cage group. According to a study by Lee et al., 25 based on CT scans, fusion rates after L5-S1 interbody fusion were higher in patients in whom a titanium-made ALIF cage had been used than in those patients with PEEK-made ALIF cages.
Third, the disc height after interbody fusion surgery was greater and significantly more increased in the ALIF group than in the TLIF group; the DH at 2 years was 17.9 mm for the ALIF group and 13.2 mm for the TLIF group (Table 3). Solid fusion after interbody fusion surgery can be achieved when the fusion masses from both endplates meet each other within the cage or around the cage. Therefore, a taller cage or disc height is disadvantageous for achieving solid fusion because of the lengthening of the distance between the fusion mass from the endplates meeting together. In this study, 16 (30.2%) out of 53 patients in the ALIF group showed nonunion, most of whom had locked pseudoarthrosis (15 patients). Locked pseudoarthrosis indicates failure of the fusion masses to meet inside the cage. Therefore, the authors thought that increased disc height caused by tall cages during ALIF surgery probably increases the risk of nonunion, especially in the form of locked pseudoarthrosis.
Our study showed that ALIF has more advantages over TLIF in terms of segmental lordosis restoration. However, the fusion rate of ALIF was lower than that of TLIF. These results did not make us use the TLIF procedure only in ASD surgery. First, we should find a way to increase the fusion rate after ALIF. ALIF using BMP might be one of the solutions, which is well known as a strong fusion enhancer.36, 37 However, we did not use BMP in this study because its use has not yet been approved for lumbar interbody fusion surgery in our country. If the safety issues are resolved, BMP can be considered for ALIF surgery to obtain a solid fusion. ALIF with posterior fusion might be a solution to overcome the disadvantage (less fusion rate) of ALIF at L5-S1. Second, there are clinical considerations for each individual case, such as vessel anatomy, previous abdominal surgery, and obesity.
Although the fusion rate was lower in the ALIF group than in the TLIF group, the metal failure rate did not differ between the two groups. Kaplan–Meier survivorship analysis also showed a similar probability of no metal failure between the two groups. In the literature, the failure rates at the L5-S1 after iliac fixation were reported to be 4.9% by Kuklo et al., 12 7.5% by Tsuchiya et al., 11 11.9% by Cho et al., 24 and 12.0% by Guler et al. 38 The failure rates reported in this study (17.0% for ALIF group and 13.3% for TLIF group) are slightly higher than those reported in previous studies. The relatively higher metal failure rates in this study may be explained by the relatively longer follow-up durations in the current study (mean 57.7 months) than in the others.12, 24, 38 Another reason may be that some of the previous studies included not only long segment fusion surgery but also short fusion surgery for treating high-grade spondylolisthesis.11, 12
In this study, we noticed that not all patients with metal failure had been diagnosed as nonunion on CT scan. Four patients with metal failure in each group were diagnosed with fusion on 2-year CT scanning. One of our cases (Figure 5) showed bilateral rod fracture after the postoperative 2-year CT proved L5-S1 solid fusion. This means that fusion strength, even after interbody fusion, might not be enough to endure repetitive stress on the metal rod. 39 In this study, revision surgery was considered for only one patient who had bilateral L5-S1 rod fractures after ALIF surgery and had persistent back pain. Thus, the revision surgery rate among the patients with metal failure was low, at 6.7% (one out of 15 patients). A similar result was reported in a recent study. In Adogwa’s study, they reported that revision surgery was required in 14 (51.9%) out of 27 patients with metal failure in the TLIF cohort and in four (36.3%) of 11 patients with metal failure in the ALIF cohort. 28 Daniels et al. 39 found that 38 (9.5%) of 402 patients with radiographically apparent solid fusion suffered a broken rod, suggesting the radiographically apparent fusion mass may not be strong for repetitive mechanical stress in a long-term period. Another study reported rod fracture despite a CT scan showing fusion among spinal tumor patients after total en bloc spondylectomy. 40
Although radiographic outcomes were not the first aim of this study, the evaluation of radiographic parameters cannot be left out because one of the strong advantages of ALIF is its greater capacity to restore sagittal balance.1, 20 As expected, in this study, the values at 2 years and their changes in critical sagittal parameters such as LL, PI-LL, SS, and PT were significantly greater in the ALIF group than in the TLIF group. Although the ALIF group showed superior results in the sagittal parameters, the differences in values were not much larger, with an LL difference of approximately 5°, LL change difference of approximately 6°, and SS difference of about 4°. These differences could be within the range of measurement errors. Therefore, other fusion techniques above the L5-S1 segment and proper rod bending to achieve the optimal sagittal alignment should also be considered important to achieve the planned sagittal alignment goal in addition to L5-S1 interbody fusion techniques.
This study has several limitations. First, there was a time gap between the CT study and the final follow-up. It is our routine practice to perform CT scans at 2 years postoperatively. Subsequently, CT scans are not routinely performed unless there are metal failures. Thus, we cannot guarantee the fusion of L5-S1 in cases of no metal failure when nonunion was diagnosed on 2-year CT scan. However, previous studies have stated that pseudoarthrosis is mainly observed six to 9 months postoperatively and bony arthrodesis is mostly completed by 6 months postoperatively.41, 42 Hence, we believe that the absence of a CT study after 2 years would not be an issue. The second limitation may be the lack of long-term follow-up. In this study, most patients with metal failure had unilateral rod fractures with intact contralateral rods. These patients have a potential risk of developing bilateral rod fractures, which may be related to new symptoms or revision surgery. Thus, a long-term follow-up is necessary. Third, additional surgical supplements, such as the use of cobalt chrome rods or multirod fixations, were not used in this study. Therefore, the incidence of nonunion or metal failure may have been rated higher in this study. Fourth, the present study was retrospective and had limitation of potential bias, although the data used were collected consecutively. Last, there were some major differences related to fusion rate between two patient groups other than surgical approaches, including 1) the materials and volume of bone graft, 2) cage material (PEEK and titanium), and 3) disc height after interbody fusion surgery, as discussed earlier in the manuscript. However, clinically, it is difficult to compare the two surgical procedures (ALIF vs TLIF) under the same conditions.
Conclusion
TLIF showed a better fusion rate than ALIF with PEEK cage at the L5-S1 segment after long instrumented fusion for ASD. The capacity to restore sagittal parameters was greater in the ALIF group than in the TLIF group. However, there were no differences between the groups in terms of metal failure rate, revision surgery, or clinical outcomes.
Footnotes
Author Contributions
Authors’ contributions: SJP conceptualized and designed the work. They also drafted the manuscript. JSP drafted the work and analyzed the data set, and CSL interpreted the data. KHL conceptualized or designed the study. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The need for approval was waived by the IRB file No. 2021-04-006.