
Abstract
Study Design
Retrospective analysis.
Objectives
To evaluate resolution of radiculopathy in one-level lumbar fusion with indirect or direct decompression techniques.
Methods
Patients ≥18 years of age with preoperative radiculopathy undergoing single-level lumbar fusion with up to 2-year follow-up were grouped by indirect and direct decompression. Direct decompression (DD) group included ALIF and LLIF with posterior DD procedure as well as all TLIF. Indirect decompression (ID) group included ALIF and LLIF without posterior DD procedure. Propensity score matching was used to control for intergroup differences in age. Intergroup outcomes were compared using means comparison tests. Logistic regressions were used to correlate decompression type with symptom resolution over time. Significance set at P < .05.
Results
116 patients were included: 58 direct decompression (DD) (mean 53.9y, 67.2% female) and 58 indirect decompression (ID) (mean 54.6y, 61.4% female). DD patients experienced greater blood loss than ID. Additionally, DD patients were 4.7 times more likely than ID patients to experience full resolution of radiculopathy at 3 months post-op. By 6 months, DD patients demonstrated larger reductions in VAS score. With regard to motor function, DD patients had improved motor score associated with the L5 dermatome at 6 months relative to ID patients.
Conclusions
Direct decompression was associated with greater resolution of radiculopathy in the near post-operative term, with no differences at long term follow-up when compared with indirect decompression. In particularly debilitated patients, these findings may influence surgeons to perform a direct decompression to achieve more rapid resolution of radiculopathy symptoms.
Keywords
Introduction
Lumbar radiculopathy has significant effects on individual quality of life and can severely hinder day-to-day activity. 1 The etiology of radiculopathy is of variable pathology and includes both non-compressive causes such as schwannomas, as well as compressive causes such as herniated nucleus pulposus or foraminal stenosis. 2 As such, radiculopathy is one of the most common symptoms of patients presenting to orthopedics with studies finding that 3%–5% of the American population suffers with lumbar pain.3,4 Some patients improve with conservative symptom management, but many do not improve and often elect to undergo surgical management to address their radicular symptoms.
Single level fusion with direct decompression is a well-accepted treatment in addressing lumbar radiculopathy, yet studies have found that patients undergoing fusion with direct decompression have similar outcomes to those receiving direct decompression alone.5,6 Indirect decompression is an increasingly common alternative in the treatment of radiculopathy and may represent reduced risk as compared with direct decompression, since indirect decompression does not involve resection of compressing tissue, though there is a general paucity of literature comparing outcomes following indirect decompression with other interventions.7,8
Continued resolution of the preoperative symptom complex is especially important in surgical patients, given the risks associated with surgery. In this regard, analysis at long term follow-up is essential to help determine what procedure may better suit a given patient population, particularly with pathology such as disc herniation having significant potential for recurrence. There are few studies examining long term patient outcomes after undergoing single-level fusion with or without direct decompression. The purpose of this study was to compare and evaluate symptom relief in patients experiencing radiculopathy undergoing lumbar fusion with indirect or direct decompression techniques. Specifically, we examined clinical symptoms of radiculopathy, pain, and motor scores at 3, 6, 12, and 24 months postoperatively for patients undergoing surgical single-level direct or indirect decompression.
Materials and Methods
Study Design and Inclusion Criteria
This study is a retrospective review of surgical patients presenting to a single academic institution from October 2012 to January 2021 with Institutional Review Board approval. We retrospectively identified adult patients (≥18 years) with preoperative radiculopathy who underwent elective one level lumbar interbody fusion after failing conservative management. All included patients underwent fusion for radiculopathy with concomitant instability, severe foraminal stenosis in which direct decompression alone would be insufficient to alleviate boney stenosis, or severe stenosis such that the amount of decompression was felt to lead to instability. As with any patient who presents with radiculopathy, one of the primary goals of the surgery was to address the radiculopathy.
Group Construction
Patients were grouped into either direct decompression or indirect decompression groups based on procedure type. Direct decompression included patients undergoing either anterior lumbar interbody fusion (ALIF) or lateral lumbar interbody fusion (LLIF) with posterior direct decompressive procedure as well as all patients undergoing transforaminal lumbar interbody fusion (TLIF). Direct decompressive procedure was defined as any decompressive procedure including microdiscectomy, laminectomy, laminotomy, or foraminotomy. Indirect decompression group included ALIF and LLIF patients without direct decompressive procedure.
Data Collection and Outcome Measures
Patient demographics, radiologic and clinical characteristics, and outcomes were sourced from patient records. Demographic data included sex, age at surgery, body mass index (BMI), and Charlson Comorbidity Index (CCI). Radiologically, preoperative lumbar magnetic resonance imaging (MRI) was obtained for all patients. Central canal diameter was measured in millimeters using axial plane MRI at the lumbar level where the interbody device was placed. Clinical outcome measures included postoperative resolution of radiculopathy as reported by patients, visual analog score (VAS), lower extremity motor strength exams, and postoperative complication rate. The visual analog score is the most widely used patient-reported measure of pain intensity in the context of lumbar back pain. 9 A composite VAS score, representing the average of low-back and leg VAS scores at each timepoint was used. Motor strength was evaluated using the Medical Research Council Manual Muscle Testing Scale (0-5 grading). Radiculopathy resolution was classified into 3 groups: Full, Partial, or No Resolution. No resolution at respective follow-up timepoints was representative of no improvement from preoperative level of radicular symptoms as noted in the provider note. Partial resolution was noted if the visit note at respective follow-up timepoints noted some level of improvement relative to preoperative symptoms. Full radiculopathy resolution was representative of follow-up visit note indicating complete resolution of preoperative radiculopathy.
Surgical data included operative time, durotomy rate, intraoperative complications, and estimated blood loss (EBL). Intraoperative complications included neuromonitoring (loss of somatosensory evoked potential (SSEP) or motor evoked potential (MEP)), attending anesthesiologist halting or stopping surgery, incidence of massive transfusion protocol, or incidence of fracture. Complications in the 90-day period included cardiac, neurologic, pulmonary, ileus, airway edema, superficial or deep infection, urinary complications, and mechanical complications. Perioperative complications and length of stay (LOS) were recorded from the discharge note. A review of provider notes through 90 days postoperatively was conducted to analyze returns to the operating room within 30 and 90 days.
Statistical Analysis
Analysis was conducted using IBM Corporation SPSS Statistics for Windows, Version 25.0 (Armonk, NY; IBM Corporation). Groups were propensity-score-matched to account for intergroup differences in age. Independent sample t-tests, chi-square analyses, and logistic regressions were used where appropriate with significance set at P < .05.
Results
Patient Sample and Demographics
We identified 195 patients undergoing direct decompression and 58 patients undergoing indirect decompression during the study period. Propensity score matching was conducted to account for a significant difference in age at time of surgery between both groups, resulting in a final cohort of 116 patients (58 direct and 58 indirect). Mean age of the direct decompression group was 53.9 ± 12.9 years with 67.2% of the sample being female. The average BMI was 30.3 ± 5.9 with mean CCI being 1.97 ± 2.01. Mean age of the indirect decompression group was 54.6 ± 12.6 years with 61.4% of the sample being female. The average BMI was 30.0 ± 6.3 with mean CCI being 2.1 ± 2.03.
Demographic Data.
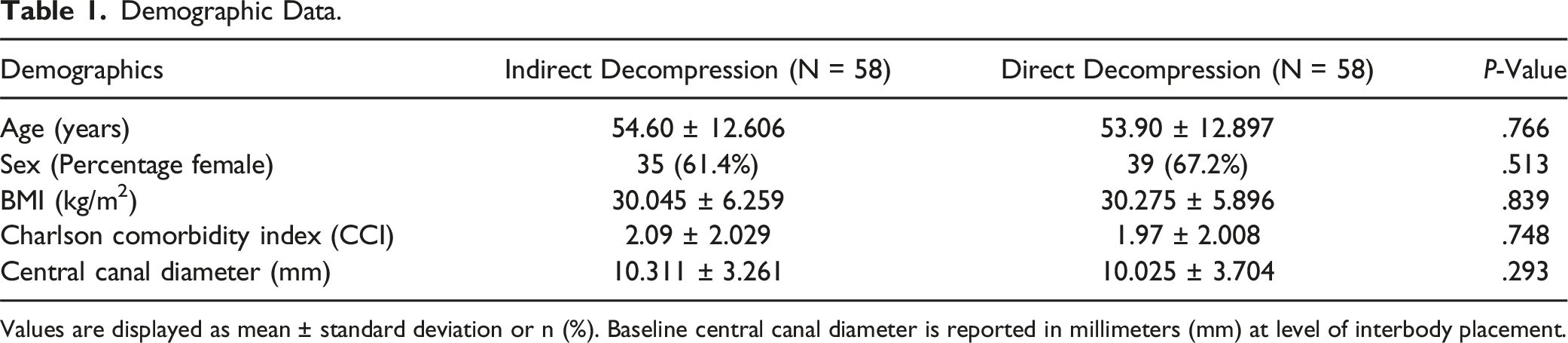
Values are displayed as mean ± standard deviation or n (%). Baseline central canal diameter is reported in millimeters (mm) at level of interbody placement.
Surgical Characteristics and Outcomes
Surgical Characteristics.
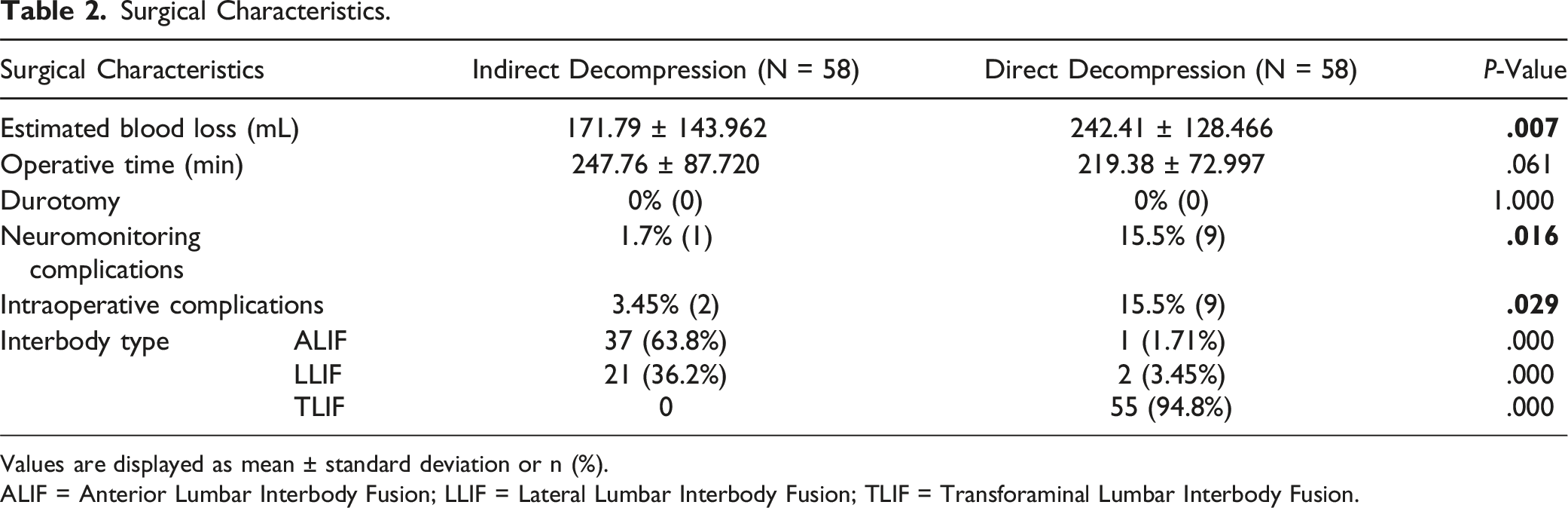
Values are displayed as mean ± standard deviation or n (%).
ALIF = Anterior Lumbar Interbody Fusion; LLIF = Lateral Lumbar Interbody Fusion; TLIF = Transforaminal Lumbar Interbody Fusion.
Patients undergoing direct decompression experienced significantly greater blood loss (242.4 ± 128.5 v 171.8 ± 143.9, P = .007) relative to indirect patients. No differences were observed between direct and indirect groups for length of stay (3.2 ± 1.5 v 3.4 ± 1.6, P = .434), operative time (219.4 ± 72.9 v 247.8 ± 87.7, P = .061), or durotomy rate (.0 v .0, P = 1.00). Direct patients had higher rates of intraoperative neuromonitoring changes (1.7% (1) v 15.5% (9), P = .016) (Table 2). Other intraoperative complications included one indirect case in which the left facet screw head broke off.
Postoperative Surgical Characteristics.
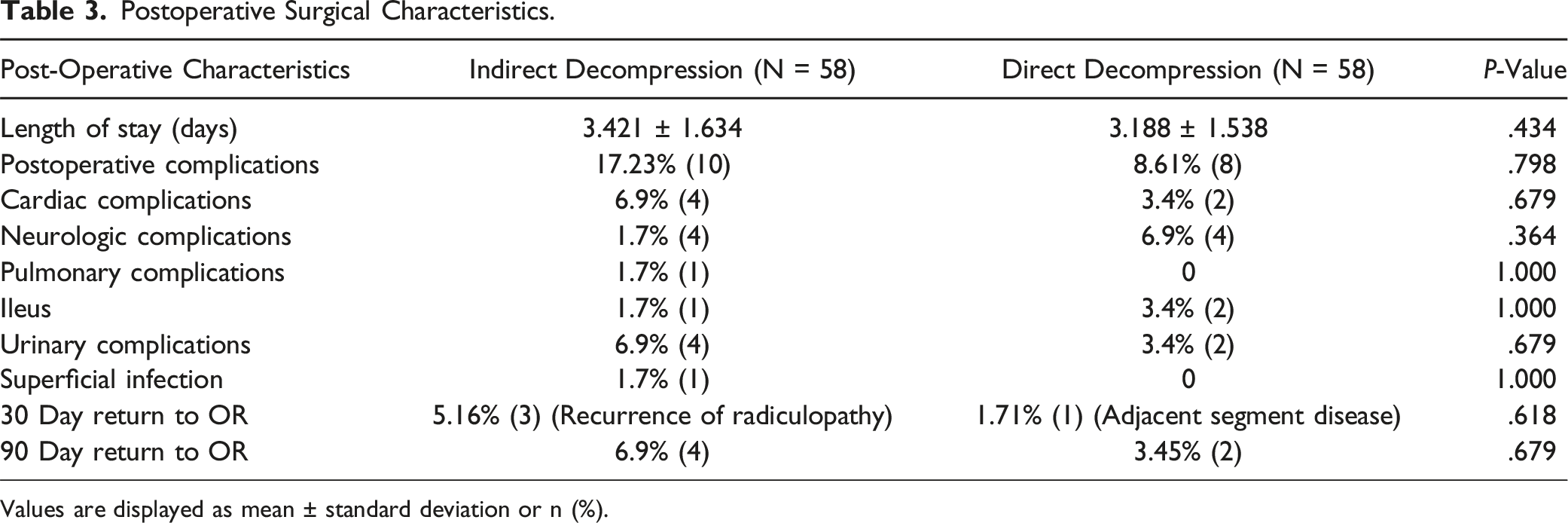
Values are displayed as mean ± standard deviation or n (%).
Radiculopathy Resolution and Change in Motor Function
Postoperative Resolution of Radiculopathy.
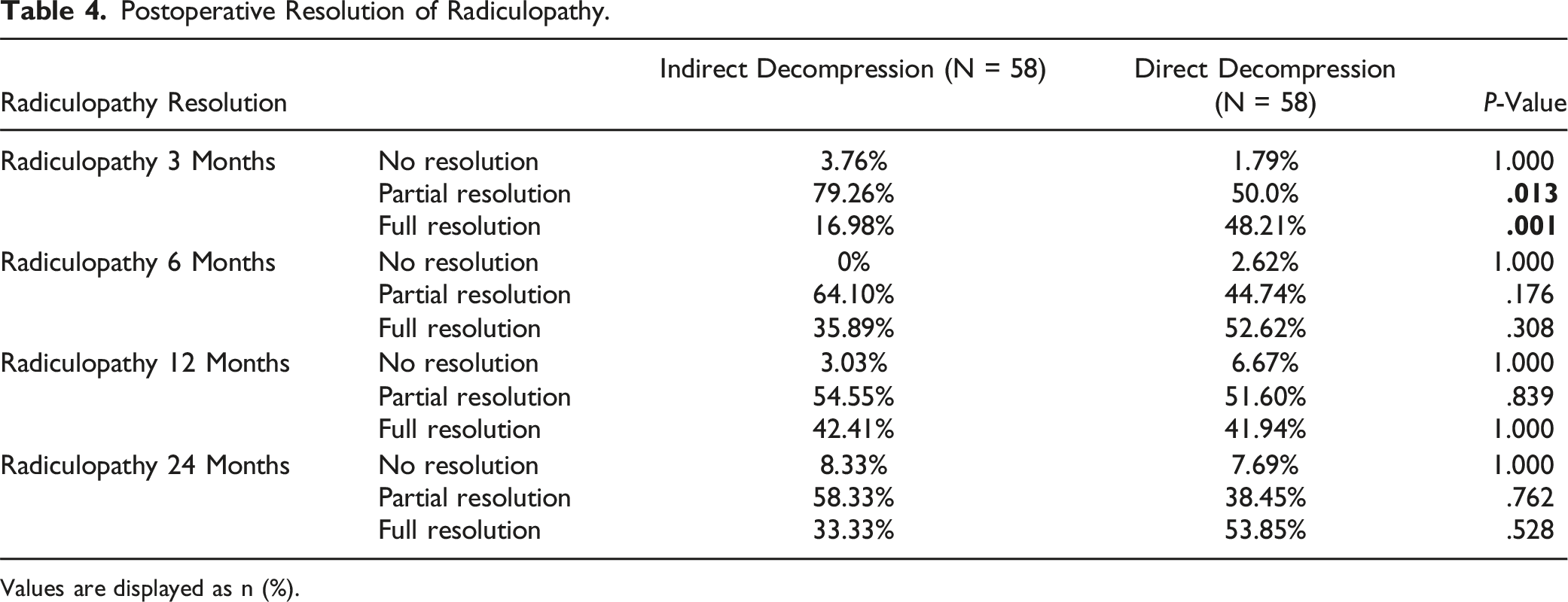
Values are displayed as n (%).
Visual Analog Scale Score.

Values are displayed as mean ± standard deviation or n (%).
Postoperative Characteristics of Motor Function.
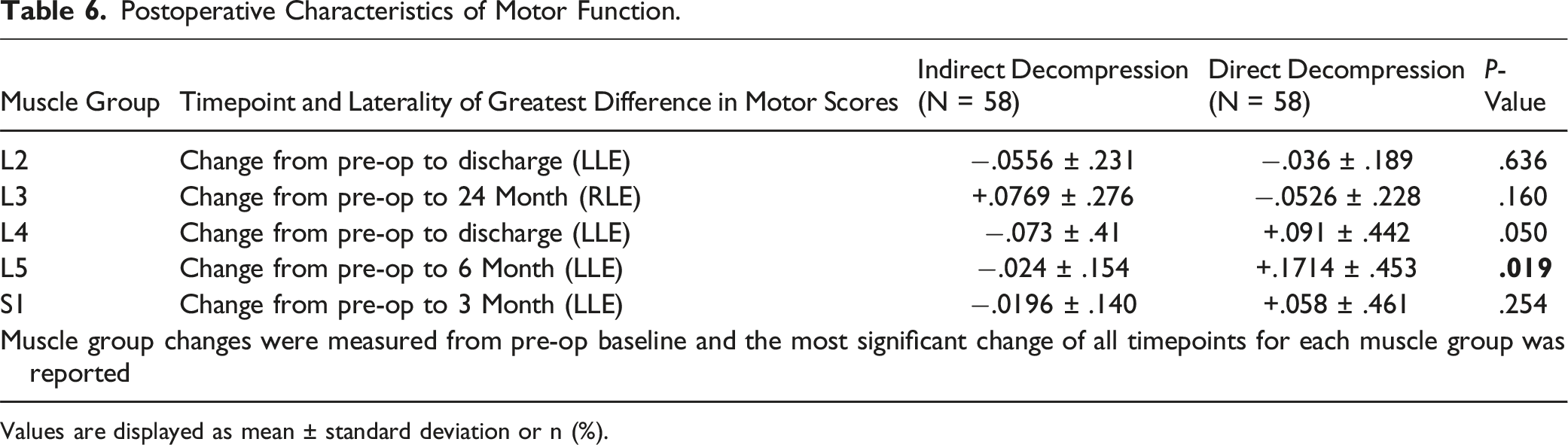
Values are displayed as mean ± standard deviation or n (%).
Discussion
When considering spinal surgery for radicular symptoms, the use of indirect decompression vs direct decompression is an important consideration. Though both approaches have shown promise in decompressing the spinal elements, they each offer benefits and challenges respectively. The purpose of this study was to investigate whether one offers superior therapeutic advantage. Complications arising from these decompressions with fusions are often related to injury of the paraspinal musculature.
In this study, we compared indirect with direct decompression in the treatment of lumbar radiculopathy. After propensity score matching groups for age, direct decompression was shown to be more effective than indirect decompression in resolving preoperative radiculopathy in the short term (at 3 months post-op) with similar outcomes between groups in the longer term (6, 12, and 24 months post-op). Similarly, direct decompression was associated with significantly greater reduction in VAS score at 6 months post-op relative to indirect decompression; though no differences were noted for other follow-up timepoints through 2 years. Both our short-term and long-term findings are consistent with those of McKeithan et al, who analyzed direct and indirect surgical outcomes in lumbar spondylolisthesis in a large national sample, supporting the durability of our results. 10
Differences in motor score change from baseline through 2 years were significant only at 6 months for the L5 muscle group, with direct patients improving and indirect patients declining from baseline (P = .019). Estimated blood loss was higher in the direct decompression group, in line with previous studies. 11 There were no significant differences in central canal diameter or postoperative complications between groups.
Regarding operative time, indirect decompression time was approximately 27 minutes longer, though analysis revealed the difference to be insignificant (P = .061). This difference may be attributable to the greater proportion of ALIF patients within the indirect group, with the anterior approach having a greater operative time given the use of vascular assistance, though this finding differs from previous literature. 12
Our primary finding of direct decompression offering more rapid symptom resolution is supported by Khalsa et al’s 2019 study; which reported indirect lumbar decompression being associated with greater post-operative pain improvement in patients with lower pain levels at baseline. 13 In our study, direct group patients had significantly lower preoperative L5 motor scores (4.86 v 4.9) with higher VAS, though the difference in baseline VAS score only approached significance (6.59 v 5.56, P = .08) This greater symptomatology may have influenced surgeons to perform direct decompression for patients in their effort to provide the most optimal treatment. The lack of VAS significance may be an artifact of the study’s limited sample size.
The decrease in tibialis anterior (L5) motor function in indirect patients at 6 months relative to the positive change in direct patients is consistent with the literature which shows LLIF to be associated with a greater risk of neurologic complications relative to TLIF. 14 Sembrano et al. found LLIF to be associated with greater rates of postoperative motor weakness. 15
Empirically, ALIF, LLIF, and TLIF all have been reported to offer some level of stenosis correction and disc height restoration, though the techniques individually carry separate risks. 16 ALIF and LLIF do not involve direct neural retraction and spare the paraspinal muscles thereby reducing risk of both epidural and perineural fibrosis and can result in reduced degree of postoperative disability respectively.17–19 ALIF is associated with a risk of vascular injury given the extent of intraoperatively retracted vasculature. 20 Voyadzis et al reported no correlation of muscle dysfunction associated with length of retraction time in patients undergoing single-level LLIF. 21 As a pedicle-based approach, TLIF requires facetectomy with hemi-laminectomy as well as dural retraction and involves damage to the paraspinal musculature, increasing risk of neurologic injury and fibrosis as well as increasing postoperative degree of disability. 22
It is important to recall the indirect cohort was composed primarily of ALIFS and LLIFs while the direct group was primarily composed of TLIFs. This study’s focus on interbody fusions can help correlate the varying degrees of disc and foraminal height restoration associated with each interbody type with symptomatic improvement in patients. 23
This study is not without limitations. The decision of whether to perform indirect or direct decompression was taken at time of index surgery by the attending surgeon without a standardized treatment algorithm. The nonrandomized retrospective structure of the present study is a limitation. Further investigation is warranted to determine the profile of patients requiring posterior instrumentation with and without interbody devices.
Conclusion
This study found direct decompression to be associated with more rapid resolution of radiculopathy symptoms, with no differences in the long term as compared with indirect decompression. This finding serves to underscore the importance and utility of targeted intervention in patients experiencing lumbar radiculopathy and may influence surgeons to perform direct decompression in particularly debilitated patients so as to effect more rapid symptom resolution.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.