
Abstract
Study Design:
Network meta-analysis of randomized controlled trials.
Objectives:
Lumbar spondylolisthesis is a common indication for spinal fusion. Lumbar interbody fusion (LIF) is popular method to achieve arthrodesis, but previous syntheses usually used head-to-head comparison of 2 surgical methods, and no of them pooled analysis with high-quality. This network meta-analysis of randomized controlled trials was carried out to simultaneously compare fusion techniques in the treatment of lumbar spondylolisthesis.
Methods:
Three databases were searched for randomized controlled trials (RCTs) on this topic. After critical appraisal, fusion rate, overall adverse events, operative time, Oswestry Disability Index, and pain were extracted for analysis. We conduced network meta-analysis using contrast-based method. Primary outcomes were reported as risk ratio (RR) with 95% confidence interval (CI).
Results:
Fifteen RCTs (n = 992) met our eligibility criteria. The RCTs treated patients posterolateral fusion (PLF), posterior LIF (PLIF), transforaminal LIF (TLIF), minimally invasive (MIS) TLIF, extreme lateral LIF (XLIF), and circumferential fusion. The pooled estimate showed that circumferential fusion led to significantly higher fusion rate than PLF (RR = 2.15, 95%CI:1.41–3.28), PLIF (RR = 2.11, 95%CI:1.38–3.22), TLIF (RR = 2.13, 95%CI:1.39–3.27), MIS-TLIF (RR = 2.13, 95%CI:1.35–3.35), and XLIF (RR = 2.01, 95%CI: 1.25–3.22). Moreover, circumferential fusion exhibited the best balance in probability between fusion rate and adverse event rate. No evidence showed inconsistency or small-study effect in the results.
Conclusions:
Collectively, circumferential fusion might be worth to be recommended because it exhibits the best balance between fusion rate and overall adverse event. PLF is still an inferior procedure and requires shorter operative time.
Keywords
Introduction
Lumbar spondylolisthesis is a common adult spinal disorder.1-3 Although many patients are asymptomatic and lumbar spondylolisthesis is found incidentally,4,5 the disease can lead to low back pain and radicular pain. Most of the patients can be managed conservatively with spinal brace, drugs, physical therapy, and epidural steroid injection. 6 However, patients with refractory symptoms who do not respond well to the abovementioned treatments still require surgical managements. Among the surgical procedures indicated for spondylolisthesis, spinal fusion after neural element decompression is the standard technique. This procedure has been used for a long period and demonstrates satisfactory outcome.7,8 Many options are available to perform lumbar spinal fusion, and posterolateral fusion (PLF) has been considered the gold standard for decades.9,10 Lumbar interbody fusion (LIF) with bone grafts or cages became popular recently. The proposed benefits of interbody fusion include restoration of spinal alignment, indirect decompression of the neural foramen, and increasing fusion rate.11,12 Anterior LIF (ALIF), posterior lumbar interbody fusion (PLIF), and transforaminal interbody fusion (TLIF) are proved to be effective methods.13-15
Recently, many minimally invasive surgical (MIS) procedures were introduced, such as MIS-PLIF, MIS-TLIF, and oblique LIF (OLIF). These MIS are associated with minor trauma to the bone and soft tissue, lesser blood loss, and shorter hospital stay, but their safety and efficacy are still unclear.16-19 Despite the surgical techniques in the treatment of lumbar spondylolisthesis, a high-quality, pooled evidence on the topic is still lacking. Thus, this network meta-analysis of randomized controlled trials (RCTs) was carried out to compare fusion techniques in the treatment of lumbar spondylolisthesis. To the best of our knowledge, this is the first network meta-analysis focusing on the surgical methods to treat lumbar spondylolisthesis.
Methods
This systematic review with network meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for reporting methods and results. The primary eligibility criteria of studies were as follows: (a) enrolled patients with lumbar spondylolisthesis, (b) treated patients LIF techniques, and (c) employed an RCT design. The exclusion criteria of studies were as follows: (a) recruited patients with spondylolisthesis and other disk disorders without stratification, (b) compared fusion procedures with decompression alone without fusion, (c) did not compare LIF technique to surgical intervention or other LIF technique, and (d) had gray literature without details about methods and results.
Data Sources
Databases of Embase, PubMed (including MEDLINE), and Web of Science were searched for potential references using the following relevant terms: spondylolisthesis, PLIF, TLIF, lateral LIF, extreme lateral LIF (XLIF), OLIF, and ALIF. To increase sensitivity, the Boolean operator “OR” was applied to combine relevant terms of fusion techniques, and the Boolean operator “AND” was used to identify intersection of search results of spondylolisthesis and fusion techniques. The primary search strategy of fusion techniques for spondylolisthesis was built in PubMed. Although the search strategy did not use any filters for publication year, age, sex, journal category, or language, we restricted studies to human by using the Boolean operator “NOT” animal [MeSH Terms: noexp]. The final search was done in April 2020 (Supplementary File 1).
Evidence Selection
To identify potential references from the databases, 2 authors imported references into EndNote software X9 for further screening. They independently screened and checked titles and abstracts for eligibility. Then, they retrieved the full texts for further review. All team members made the final judgment of the evidence selection if the 2 authors had inconsistency in choosing articles.
Data Extraction
The 2 authors also independently extracted and double-checked information and data from each trial. They listed the first author’s family name, publication year, study region, fusion technique, age, sex, spondylolisthesis type, and disease grade. They extracted events, sample size for fusion rate and overall adverse event, and mean, standard deviation, and sample size for operative time, Oswestry Disability Index (ODI) score, and pain score from the included RCTs. Overall adverse event in the included trials mainly involved nerve injury, infection, cage migration, dura tear, screw loosing, and screw breaking. If the trials presented percentage for fusion rate or adverse event, these events were converted according to the sample size.
Quality Assessment
All included RCTs underwent quality assessment, and the 2 authors evaluated the risk of bias by using the Cochrane Risk of Bias Tool. It is a common tool for RCT appraisal and covered randomization generation, allocation concealment, blinding (we mainly assessed blinding of patients and assessor because this topic cannot blind to surgeon), incomplete outcome data, selective report, and other source of bias. We reported overall risk of bias according to rules as follows: (a) if any bias was high risk, overall risk of bias should be high risk; (b) if any bias was unclear and no high risk of bias, overall risk of bias was unclear; and (c) if all bias were low risk, overall risk of bias was low risk. Discrepancy on risk of bias appraisal was resolved by discussion.
Data Synthesis and Analysis
In this study, the primary outcomes were fusion rate and overall adverse event rate (dichotomous variables); thus, risk ratio (RR) was used to present pooled estimate. Secondary outcomes were operative time, ODI score, and pain score (continuous variables). Pooled operative time and ODI were presented in weighted mean difference (WMD), while standardized mean difference (SMD) was used for pooled estimate of pain score because of the heterogeneity of scales used for pain measurement across RCTs. We also presented 95% confidence interval (CI) with effect sizes.
Most outcomes, except pain score, were pooled using contrast-based network meta-analysis, and inconsistency and small-study effects were assessed. We chose the design-by-treatment interaction model to detect inconsistency because 2-arm and 3-arm trials were included in our synthesis and co-contributed to network meta-analysis. Adjusted funnel plot and Egger’s regression intercept with centralized effect size and standard error were used to analyze small-study effect. Moreover, we conducted surface under the cumulative ranking (SUCRA) to clarify the probability of successful fusion and adverse events among PLF, PLIF, TLIF, MIS-TLIF, XLIF, and circumferential fusion. The SUCRA showed the probability of each fusion technique in ranking hierarchy and demonstrated a value of the surface under the line of cumulative ranking with mean rank. When the SUCRA value of a fusion technique was close to 1, the fusion technique had a higher probability of having better outcome. An optimal fusion technique ideally has well-balanced probabilities of higher fusion rate and lower adverse event rate; we further presented cluster plots using the SUCRA values of the fusion rate and overall adverse events. Moreover, meta-regression of proportion of isthmic lumbar spondylolisthesis was conducted under consistency model for testing the effect of subtype of lumbar spondylolisthesis on the pooled result. Thus, option “regression” was used under command “network meta” in STATA.
Because pain score data was only available from trials comparing PLF and PLIF, a network meta-analysis was unnecessary. Pain score was pooled by using pairwise meta-analysis according to the DerSimonian and Laird method. We presented I-square to understand heterogeneity among the pooled trials. When the I-square was higher than 50%, the pooled estimate of the pain score was heterogeneous. All the abovementioned analyses were carried out by STATA version 14 (StataCorp LP, College Station, Texas).
Results
We found 3832 references, which was composed of 3831 references from Embase (k = 1496), PubMed (k = 1067), and Web of Science (k = 1268). Other references were found by reviewing the reference lists of relevant studies. We used the function “Find duplicates” in EndNote software to remove duplicates (k = 1222). Irrelevant references were routed out after screening of the title and abstract (k = 2567), and we retrieved full texts for the remaining references (k = 43). Finally, 16 references from15 RCTs met our eligibility criteria, and all of them were included in this synthesis (Figure 1).18,20-34
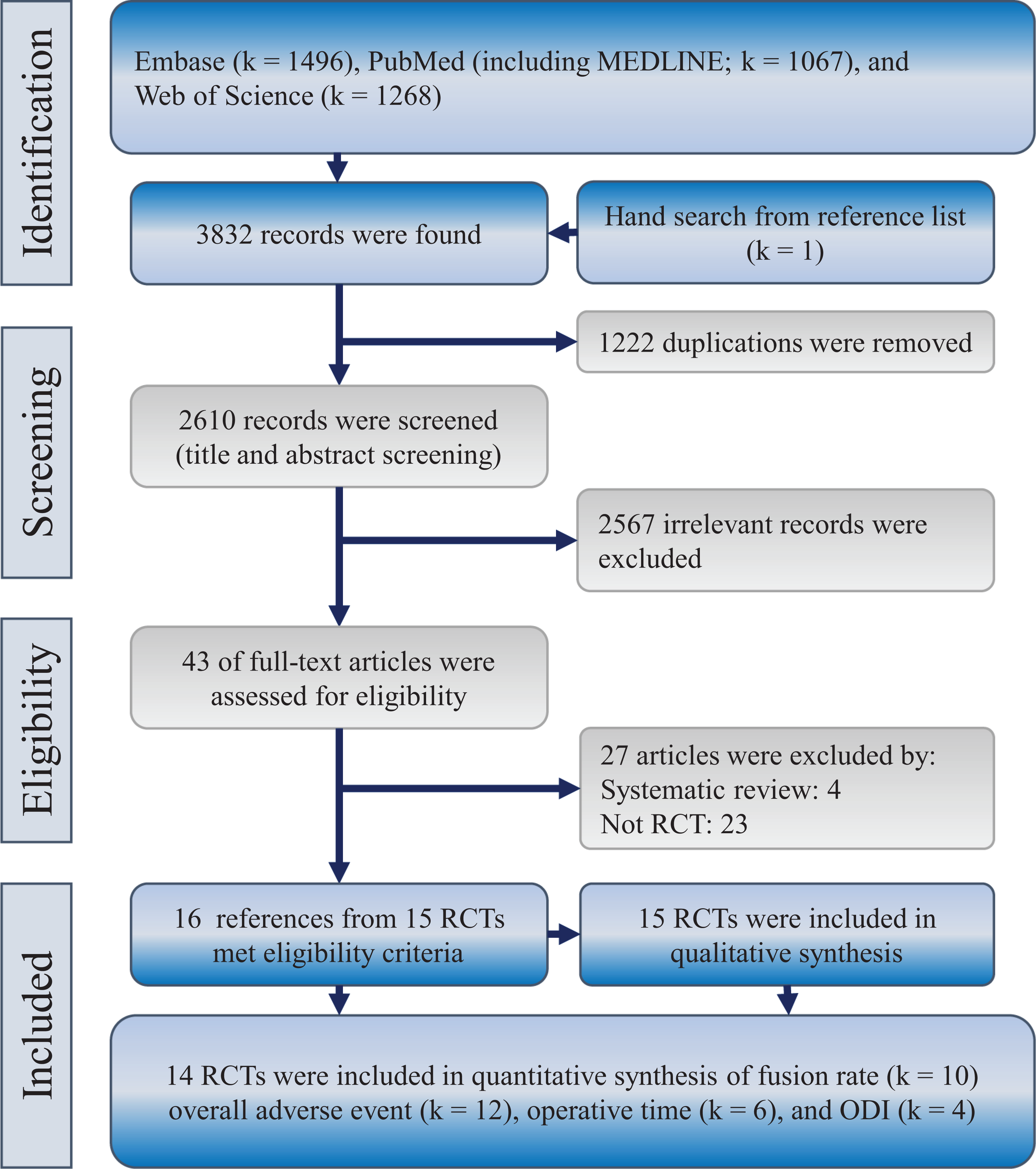
Flowchart of this systematic review with network meta-analysis of prospective studies. ODI, Oswestry Disability Index; RCTs, randomized clinical trials.
Characteristics and Quality of Included Studies
This synthesis included 15 RCTs from China (k = 3),23,27,34 Egypt (k = 1), 20 France (k = 1), 22 India (k = 1), 28 Iran (k = 4),21,24-26 Japan (k = 1), 18 Korea (k = 1), 30 Romania (k = 1), 33 Turkey (k = 1), 31 and USA (k = 1),29,32 between 2005 and 2019. These studies recruited 992 patients with lumbar spondylolisthesis. The patients underwent PLF, PLIF, TLIF, MIS-TLIF, XLIF, and circumferential fusion. Beside of traditional PLF and minimal invasive procedures, combination surgical strategy such as circumferential fusion were investigated, wherefore the present study also included RCTs that implemented circumferential fusion on spondylolisthesis. For broader definition, even TLIF with PLF and posterior instrumentation can be considered circumferential fusion although a specific definition of circumferential fusion is usually considered ALIF with posterior instrumentation. Circumferential fusion in the present synthesis involved combination of TLIF and PLF. The mean age in each study arm ranged from 41.4 to 68.2 years according to the available information. Further information about gender, type of spondylolisthesis, and grade are presented in Table 1. Most trials seemed to be high risk of bias due to inappropriate blinding to patients or assessor; and no trial was low risk of bias.
Characteristics of the Included Randomized Controlled Trials.
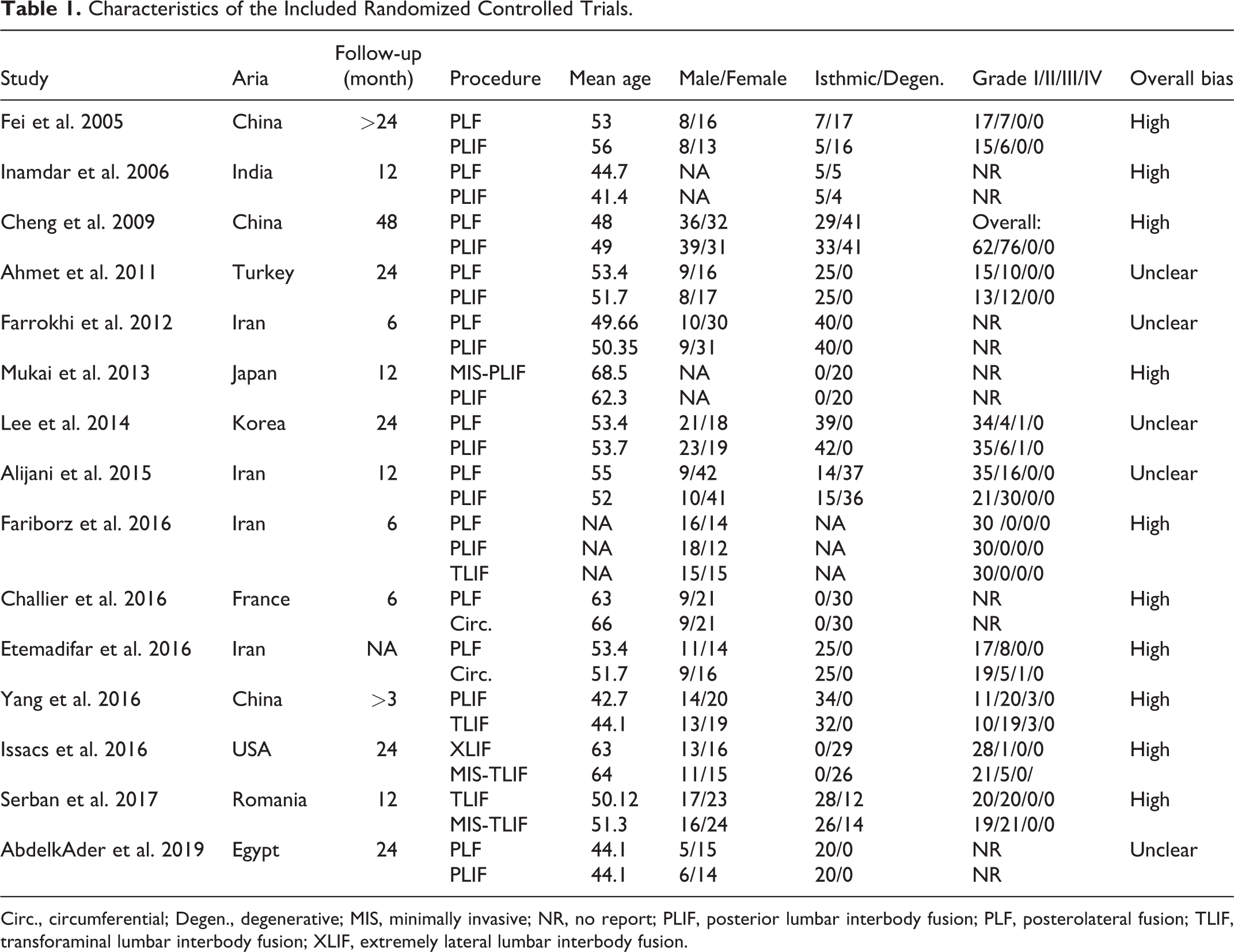
Circ., circumferential; Degen., degenerative; MIS, minimally invasive; NR, no report; PLIF, posterior lumbar interbody fusion; PLF, posterolateral fusion; TLIF, transforaminal lumbar interbody fusion; XLIF, extremely lateral lumbar interbody fusion.
Primary Outcome
The primary outcomes were fusion rate and overall adverse event rate. A total of 10 RCTs contributed to a 6-node network meta-analysis of the fusion rate (Figure 2A).20,22,23,25,28-31,33,34 The network involved 783 cases with spondylolisthesis treated by PLF (n = 273), PLIF (n = 292), TLIF (n = 102), MIS-TLIF (n = 59), XLIF (n = 27), and circumferential fusion (n = 30). Pooled result showed that with PLF as the reference, PLIF (RR 1.02, 95% CI 0.96 to 1.09), TLIF (RR 1.01, 95% CI 0.93 to 1.10), MIS-TLIF (RR 1.01, 95% CI 0.85 to 1.20), and XLIF (RR 1.07, 95% CI 0.87 to 1.33) did not lead to significant difference (Figure 3A). Moreover, no significant difference was found among PLIF, TLIF, MIS-TLIF, and XLIF. However, circumferential fusion presented significantly higher fusion rate than PLF (RR 2.15, 95% CI 1.41 to 3.28), PLIF (RR 2.11, 95% CI 1.38 to 3.22), TLIF (RR 2.13, 95% CI 1.39 to 3.27), MIS-TLIF (RR 2.13, 95% CI 1.35 to 3.35), and XLIF (RR 2.01, 95% CI 1.25 to 3.22). These results were also observed in the SUCRA (Supplementary File 2). Design-by-treatment interaction model did not show significant inconsistency in the network meta-analysis of the fusion rate (Chi-square = 1.39; P = 0.50; Supplementary File 3). Funnel plot (Figure 4A) and Egger’s test showed that small-study effect was not significant in the pooled estimate of the fusion rate (t = −0.10, 95% CI −0.85 to 0.78; Supplementary File 4). Subtype of lumbar spondylolisthesis did not show statistical significance in the consistency model of fusion rate (Supplementary File 5).
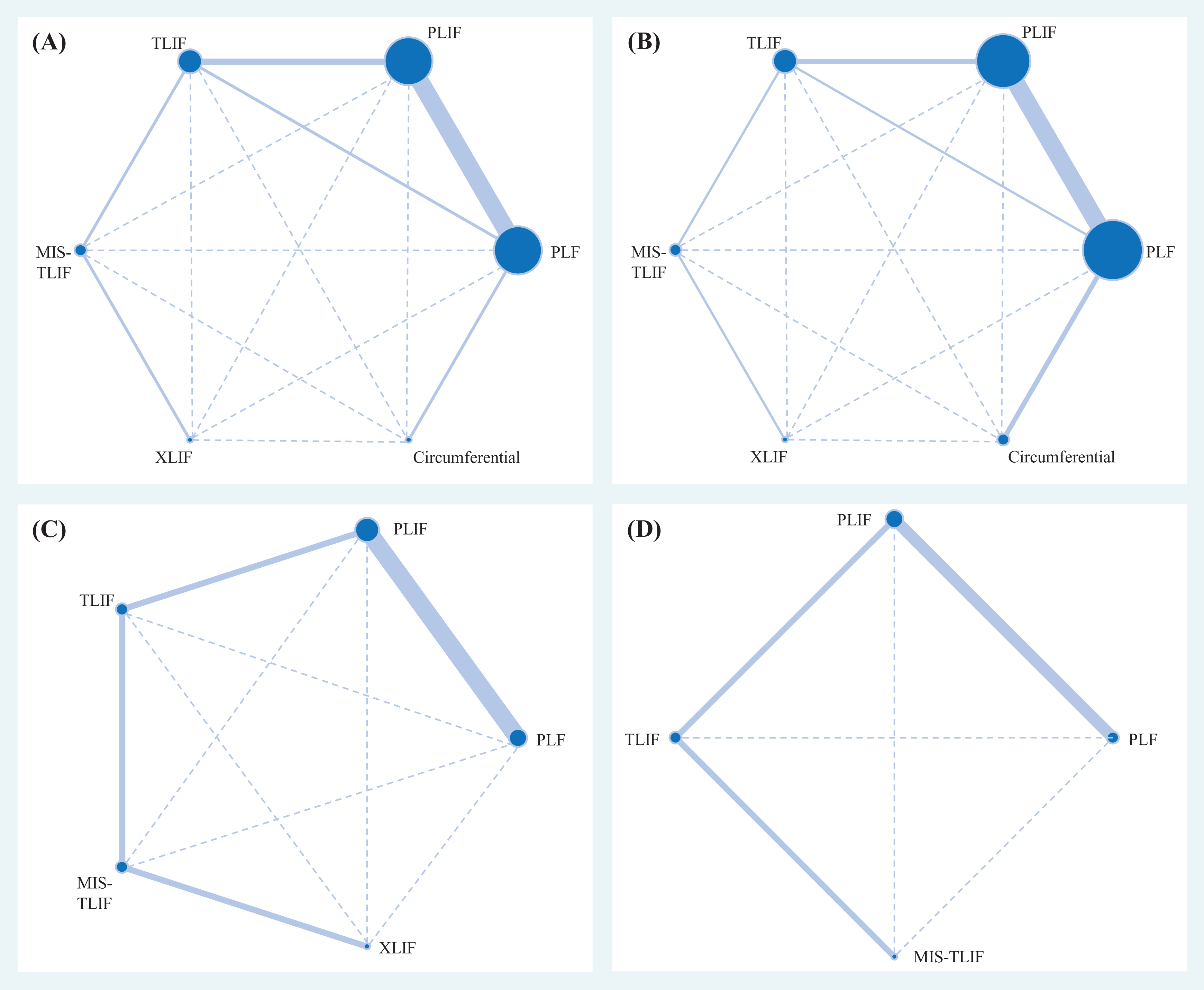
Network geometry of the consistency model of (A) the fusion rate, (B) overall adverse event, (C) operative time, and (D) Oswestry Disability Index. CI, confidence interval; MIS, minimally invasive, PLF, posterolateral fusion; PLIF, posterior lumbar interbody fusion; TLIF, transforaminal lumbar interbody fusion; XLIF, extremely lateral lumbar interbody fusion.
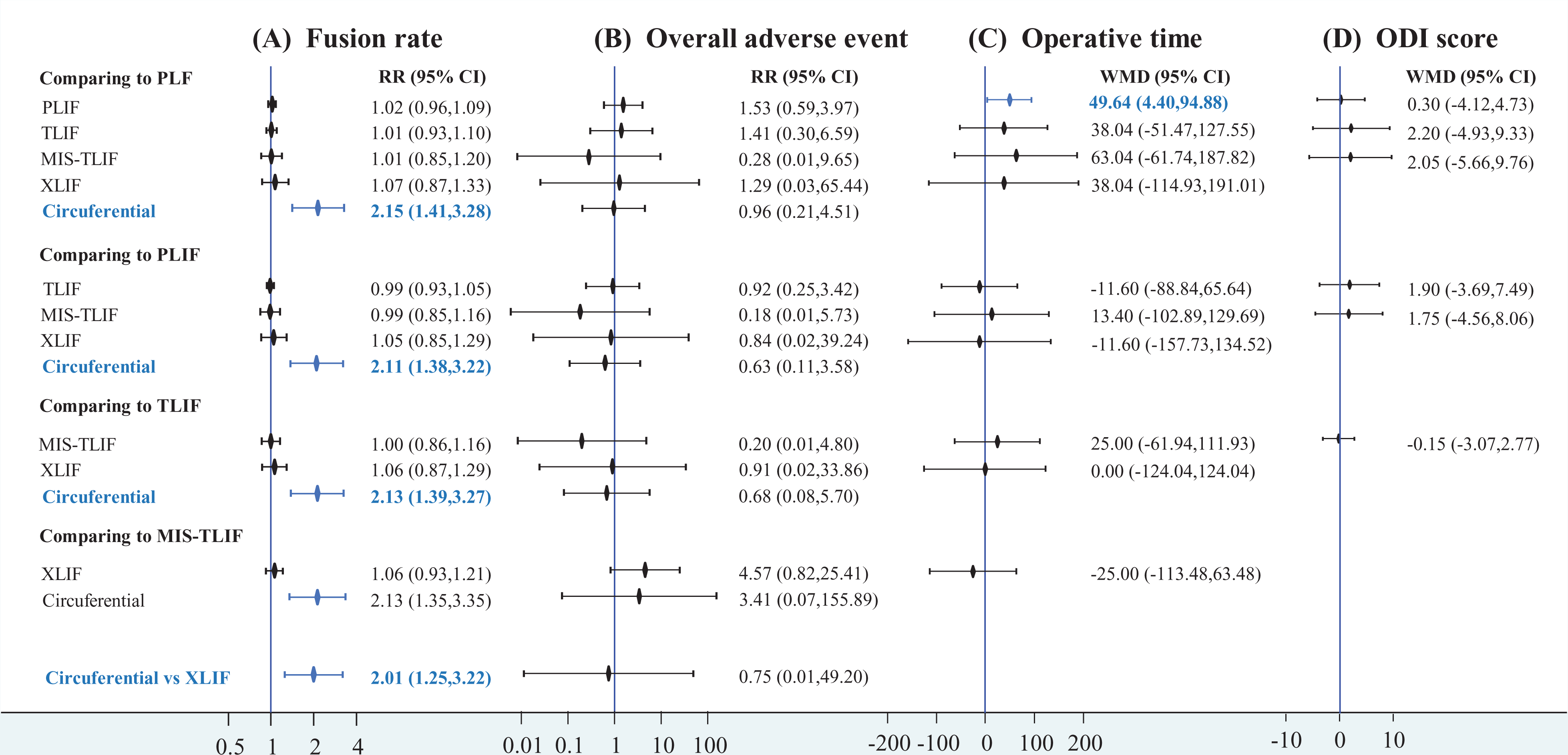
Forest plots of (A) the fusion rate, (B) overall adverse event, (C) operative time, and (D) Oswestry Disability Index. CI, confidence interval; MIS, minimally invasive, PLF, posterolateral fusion; PLIF, posterior lumbar interbody fusion; RR, risk ratio; TLIF, transforaminal lumbar interbody fusion; XLIF, extremely lateral lumbar interbody fusion.
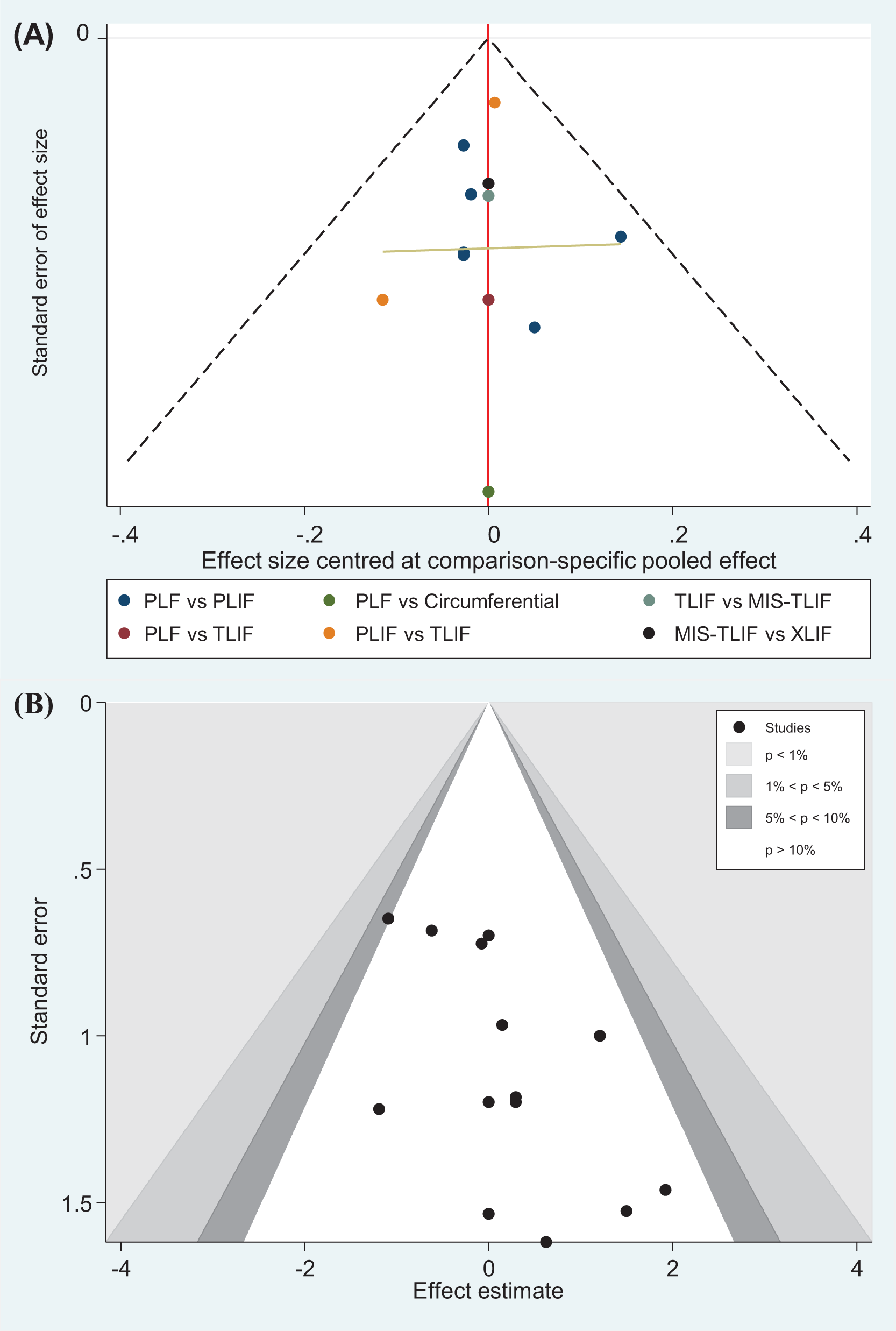
Funnel plots of (A) the fusion rate and (B) overall adverse event. MIS, minimally invasive, PLF, posterolateral fusion; PLIF, posterior lumbar interbody fusion; TLIF, transforaminal lumbar interbody fusion; XLIF, extremely lateral lumbar interbody fusion.
Another primary outcome was safety of fusion techniques, and 12 RCTs formed a 6-node network meta-analysis of the overall adverse event (Figure 2B).20,22-25,27-31,33,34 The network involved 878 cases with spondylolisthesis treated by PLF (n = 322), PLIF (n = 313), TLIF (n = 102), MIS-TLIF (n = 59), XLIF (n = 27), and circumferential fusion (n = 55). Although no significant difference existed among the 6 fusion techniques (Figure 3B), some pooled estimates raised clinical concerns. For instance, some estimates showed RR >1.5 or <0.5. To foster understanding on the safety of the 6 techniques, we performed SUCRA, and MIS-TLIF had the highest probability in preventing adverse event (mean rank = 1.9; SUCRA = 82.6), followed by PLF (mean rank = 3.2; SUCRA = 55.2), circumferential fusion (mean rank = 3.3; SUCRA = 53.3), XLIF (mean rank = 4.0; SUCRA = 39.8), TLIF (mean rank = 4.1; SUCRA = 37.8), and PLIF (mean rank = 4.4; SUCRA = 3.13; Supplementary File 6). Design-by-treatment interaction model showed no significant inconsistency in the network meta-analysis of the overall adverse event (Chi-square = 0.06; P = 0.97; Supplementary File 7). Egger’s test indicated that the pooled estimate may be affected by the small-study effect (t = 2.58, 95% CI 0.24 to 2.86), but Begg’s test showed no significance (z value = 1.75, P = 0.09; Supplementary File 8). Moreover, contour-enhanced funnel plot depicted that the possibly missed trial is found on upper right of the funnel plot, and this situation is not a typical asymmetry of small-study effect (Figure 4B). Trend and direction of comparison of PLIF and PLF did not affected after proportion of isthmic lumbar spondylolisthesis put into consistency model although the proportion showed statistical significance in the consistency model of adverse event rate (Supplementary File 9).
We further explored the balance of effect and safety among PLF, PLIF, TLIF, MIS-TLIF, XLIF, and circumferential fusion by cluster plots of the fusion rate and overall adverse (Figure 5). Circumferential fusion exhibited the best balance when we restricted to 2 clusters, and it still showed better balanced probability between fusion rate and adverse event rate when the optimal number of clusters was 3 with clustering gain of approximately 460.53. However, only 2 trials used circumferential fusion, and it was only compared with PLF. Therefore, circumferential fusion should be recommended with caution for patients with lumbar spondylolisthesis.
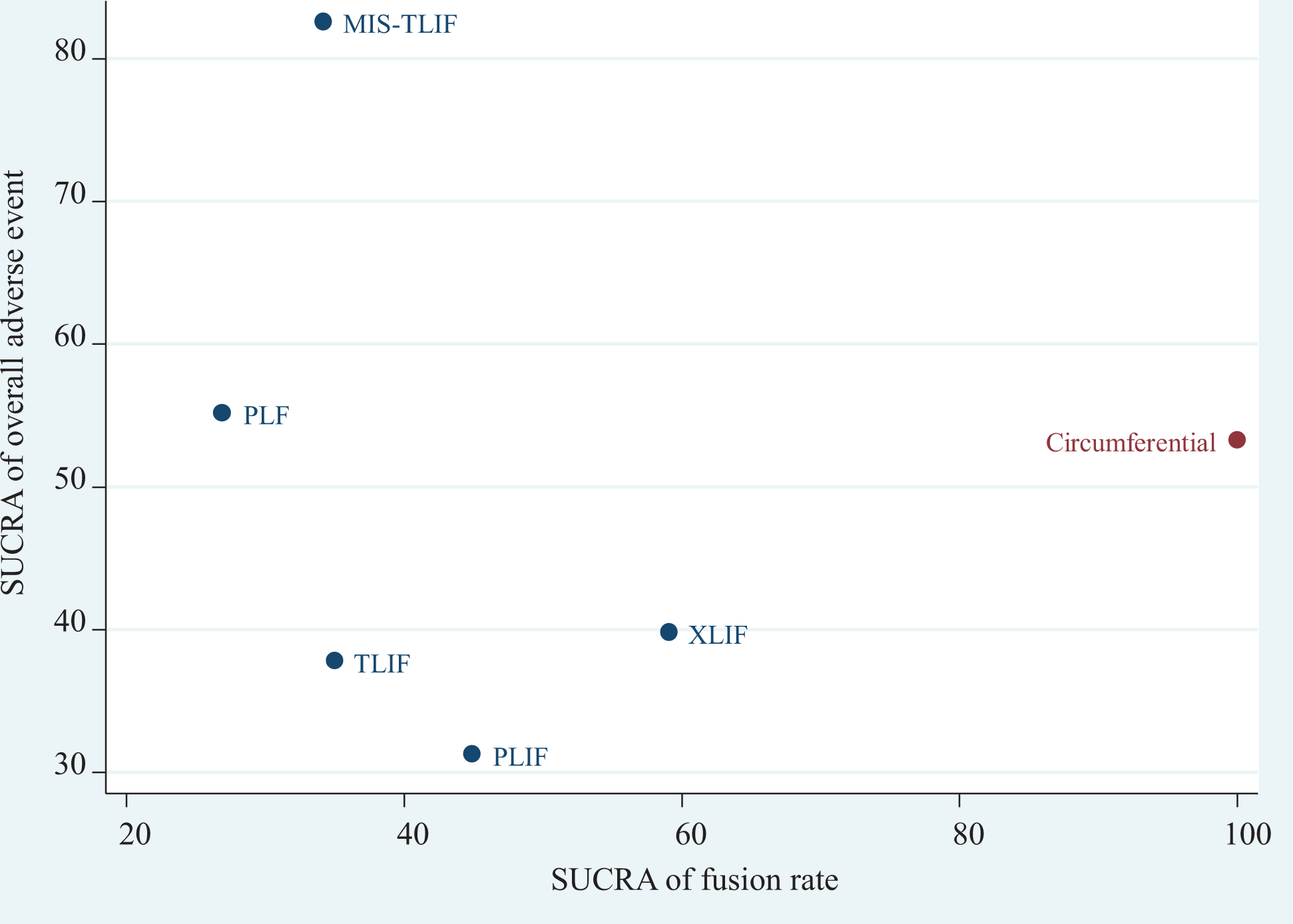
Cluster plot for the surface under the cumulative ranking of fusion rate and overall adverse event. MIS, minimally invasive, PLF, posterolateral fusion; PLIF, posterior lumbar interbody fusion; TLIF, transforaminal lumbar interbody fusion; XLIF, extremely lateral lumbar interbody fusion.
Secondary Outcome
The secondary outcomes were operative time, ODI score, and pain score. Six of the included RCTs (n = 347) reported operative time,27,29-31,33,34 and the data came from PLF (n = 59), PLIF (n = 128), TLIF (n = 76), MIS-TLIF (n = 65), and XLIF (n = 19) (Figure 2C). Pooled estimate of operative time showed that PLIF has longer operative time than PLF (WMD = 49.64, 95 CI% 4.40 to 94.88). TLIF, MIS-TLIF, and XLIF showed longer operative time than PLF, though the pooled estimates were non-significant (Figure 3C). Inconsistency test cannot be carried out because the available data did not form any loop. Funnel plot and Egger’s test showed that the small-study effect was not significant in the pooled estimate of operative time (t = −0.67, 95% CI −17.71 to 10.81; Supplementary File 10). Although proportion of subtype of lumbar spondylolisthesis showed statistical significance in the consistency model of operative time between PLIF and PLF, trend and direction of the comparison did not affected after the proportion put into the network meta-analysis model (Supplementary File 11)
Patients’ subjective outcomes were ODI, back pain, and leg pain. Data on ODI was available from 4 RCTs (n = 329),21,30,33,34 and the available data can form a 4-node network meta-analysis with PLF (n = 90), PLIF (n = 127), TLIF (n = 72), and MIS-TLIF (n = 40) (Figure 2D). The network meta-analysis showed no significant difference in the ODI between every pairwise comparison of fusion techniques (Figure 3D). Because there was no loop among the 4 fusion techniques, inconsistency test cannot be carried out. Funnel plot and Egger’s test showed that the small-study effect was not significant in the pooled estimate of ODI (t = −1.23, 95% CI −2.10 to 1.16; Supplementary File 12). Subtype of lumbar spondylolisthesis did not show statistical significance in the consistency model of ODI (Supplementary File 13). Pain score data was available for comparison of PLF and PLIF in 5 RCTs.20,26,28,30,31 All the 5 RCTs reported score for back pain (n = 271), and 4 of them presented leg pain (n = 251).20,26,30,31 Given the heterogeneity of scales to determine pain score across the trials, data was standardized in the meta-analysis. Pooled estimate showed no difference in back pain (SMD = −0.28, 95% CI: −0.82 to 0.25, I-square = 77.3%) and leg pain (SMD = −0.06, 95% CI: −0.19 to 0.31, I-square = 2.5%) between PLF and PLIF (Supplementary File 14).
Discussion
Key Findings
Our study revealed that circumferential fusion had the highest fusion rate among the procedures. For other approaches, no significant difference was found in the fusion rate or complications. However, MIS-TLIF showed a trend of lower complication rate.
Spondylolisthesis is a common indication for spinal fusion after failed conservative treatment. According to Wiltse classification, spondylolisthesis can be further divided into 6 types, while the isthmic type and degenerative type are present in most of the patients. 35 Although the patient population and common anatomic location are different, the symptoms and management are similar. As a result, we did not analyze the outcome of these 2 types separately. On the contrary, we ruled out the articles that enrolled patients other than those with spondylolisthesis. Spondylosis, low back pain, spinal stenosis, and degenerative disk disease without spondylolisthesis are excluded from our study because there are fundamental difference between these degenerative disease and spondylolisthesis and there is a need to discuss then independently. Notably, Mukai et al. compared patients who underwent PLIF to MIS-PLIF. 18 Although the studies were enrolled by systemic review, we did not include the data into the pooled analysis because the definition of MIS-PLIF is unclear, which may cause confusion. Some authors defined MIS-PLIF using wound length, while others used preservation of paraspinal muscle attachment to differentiate it with traditional PLIF.18,36 Although only a proportion of the patients was grouped randomly, Sembrano et al. discussed XLIF in treating lumbar spondylolisthesis, 32 so we included the data in the pooled analysis.
In our review, the fusion rate is selected as the primary outcome in most studies. Some authors claimed that solid fusion is not related with better clinical symptoms,37-39 but other studies revealed that solid fusion may have inferior outcome accompanied with pseudoarthosis.40-42 In the present study, the circumferential fusion procedure can reach the highest fusion rate, while other approaches revealed similar fusion rate. This is in line with our expectation that combined PLF and interbody fusion can facilitate solid bony union. Unfortunately, the clinical outcome and operative time of circumferential fusion is not available for comparison; thus, we cannot determine whether the procedure is more time-consuming or superior to other techniques clinically. In addition to surgical method, many other factors may affect the success of fusion, such as the type of graft, patient age, comorbidities, smoking, and fusion levels. Despite these factors, the heterogeneity is acceptable throughout the study (I-square < 50%); thus, we believed that our conclusion is convincing. Another outcome is the postoperative complication rate. All procedures showed similar complication rate without significant difference, but SUCRA revealed higher recommendation for MIS-TLIF. Similar finding was mentioned in the study by Wu et al. and Khan et al.43,44 Khan et al. explained the phenomenon with surgeon learning curve and maturation of the technique. Generally, MIS is usually more technique demanding with a steeper learning curve than traditional open surgery. However, we believed that the surgeons who performed MIS-TLIF are experienced and familiar with the procedure. Thus, the conclusion can be applied only to mature operators who have sufficient experience of the approach. Among the procedures, PLF seems to be the most time-saving one because the procedure eliminates intervertebral disk removal, endplate preparation, and cage insertion.
Comparison With Previous Syntheses
In our literature review, many systemic reviews and meta-analysis discussed different fusion methods for spondylolisthesis separately. Ye et al. compared PLIF with PLF and showed higher fusion rate for PLIF, but their study included not only RCTs but also prospective and retrospective studies. 45 Cho et al. compared ALIF with other approaches simultaneously and concluded better restoration of spinal alignment with ALIF. However, the study did not discuss the fusion rate, and the quality of the evidence is not strong. 46 Kwon et al. found that circumferential fusion can achieve higher fusion rate than anterior or posterior procedure alone in the treatment of isthmic spondylolisthesis. 10 Liu et al. also concluded that circumferential fusion improves fusion rate compared with PLF and that the complication rate is comparable. 47 Our research also supports the use of circumferential fusion.
Limitation
This study has some limitations. First, we included 15 RCTs, yet only one RCT used XLIF and none of them discussed OLIF and ALIF. As a result, based on current evidence, we cannot give recommendation for these 2 procedures even though they showed promising result in non-RCT studies.48-50 With regard to LIF procedures, direct and guided strategies are discussed in recent years, while they are out of range of our study. Moreover, it seems to appear to be a lack of no randomized controlled trial on direct LIF or guided LIF for spondylolisthesis. They are worth further studies in the future. In addition to limitations on evidence of lumbar fusion techniques, outcome limitations should be declared. For primary outcome, fusion was varied by studies. Some studies used radiography, while others used dynamic view or CT to determine solid fusion. The finding of fusion rate might be not seriously affected by the definition, and heterogeneity of the pooled estimate is low (I-square = 0%) even though the tools for solid fusion are different in the included RCTs. For most secondary outcomes, the network analysis could not form a loop and decreased the reliability of the result. Most of the studies only reported short-term or mid-term results, and there are no data about complication after 5-year follow-up. In the future, high-quality RCTs with longer follow-up are still necessary. Besides, evidence on some clinical outcomes were insufficient, including operative time, hospital stay, and cost. These outcomes may also associate to lumbar fusion procedures since the techniques this study discussed can be done in one day or staged. Consequently, the clinical outcomes raise concerns in clinical practice. These ultimate outcome measures ought to be further assessed by studies in the future.
Conclusions
Collectively, the present evidence indicated that circumferential fusion might be worth to be recommended for lumbar spondylolisthesis management because it exhibits the best balance between fusion rate and overall adverse event. PLF is still an inferior procedure and requires shorter operative time than other procedures. To improve clinical practice, operative time, hospital stay, and cost should be evaluated in the future.
Supplemental Material
Supplemental Material, sj-pdf-1-gsj-10.1177_2192568221997804 - Effects and Safety of Lumbar Fusion Techniques in Lumbar Spondylolisthesis: A Network Meta-Analysis of Randomized Controlled Trials
Supplemental Material, sj-pdf-1-gsj-10.1177_2192568221997804 for Effects and Safety of Lumbar Fusion Techniques in Lumbar Spondylolisthesis: A Network Meta-Analysis of Randomized Controlled Trials by Yi-No Kang, Yu-Wan Ho, William Chu, Wen-Shiang Chou and Shih-Hao Cheng in Global Spine Journal
Footnotes
Authors’ Note
Conceptualization: Shih-Hao Cheng and Yi-No Kang; Data curation: Shih-Hao Cheng; Formal analysis: Yi-No Kang; Interpretation: Yi-No Kang, Yu-Wan Ho, Shih-Hao Cheng; Investigation: Yi-No Kang, Yu-Wan Ho, Shih-Hao Cheng; Methodology: Yi-No Kang; Supervision: Yu-Wan Ho, William Chu, Wen-Shiang Chou; Visualization: Yi-No Kang; Writing – original draft: Yi-No Kang, Shih-Hao Cheng; Writing – review & editing: Yu-Wan Ho, William Chu, Wen-Shiang Chou.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.