
Abstract
Study Design
Single-center retrospective cohort study
Objectives
To evaluate inpatient MME administration associated with different lumbar spinal fusion surgeries
Methods
Patients ≥18 years of age with a diagnosis of Grade I or II spondylolisthesis, stenosis, degenerative disc disease or pars defect who underwent one-level Transforaminal Lumbar Interbody Fusion (TLIF) or one-level Anterior Lumbar Interbody Fusion (ALIF) or Lateral Lumbar Interbody Fusion (LLIF) through traditional MIS, anterior-posterior position or single position approaches between L2-S1. Outcome measures included patient demographics, surgical procedure and approach, perioperative clinical characteristics, incidence of ileus and inpatient MME. Statistical analysis included one-way ANOVA with a post-hoc Tukey Test and Kruskal–Wallis Test with post-hoc Mann–Whitney test. MME was calculated as per the Centers for Medicare and Medicaid Services and previous literature. Significance set at P < .05.
Results
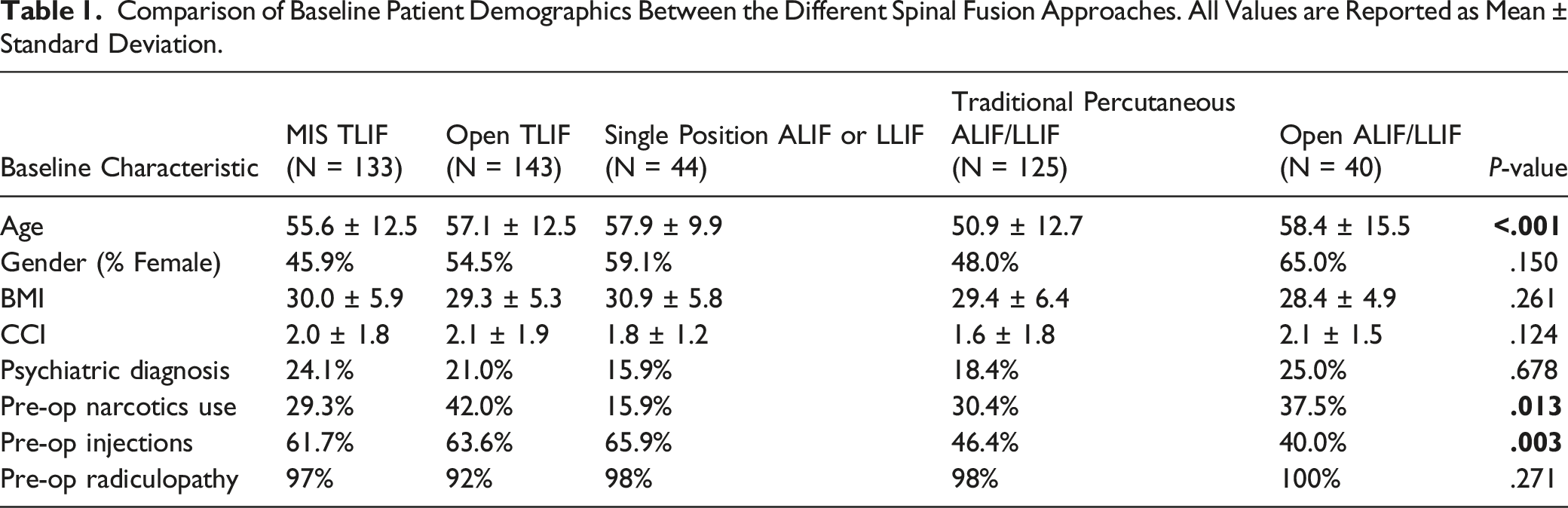
Mean age differed significantly between MIS TLIF (55.6 ± 12.5 years) and all other groups (Open TLIF 57.1 ± 12.5, SP ALIF/LLIF 57.9 ± 9.9, TP ALIF/LLIF 50.9 ± 12.7, Open ALIF/LLIF 58.4 ± 15.5). MIS TLIF had the shortest LOS compared to all groups except SP ALIF/LLIF. Total MME was significantly different between MIS TLIF and Open ALIF/LLIF (172.5 MME vs 261.1 MME, P = .044) as well as MIS TLIF and TP ALIF/LLIF (172.5 MME vs 245.4 MME, P = .009). There were no significant differences in MME/hour and incidence of ileus between all groups.
Conclusion
Patients undergoing MIS TLIF had lower inpatient opioid intake compared to TP and SP ALIF/LLIF, as well as shorter LOS compared to all groups except SP ALIF/LLIF. Thus, it appears that the advantages of minimally invasive surgery are seen in minimally invasive TLIFs.
Keywords
Introduction
The ongoing opioid epidemic plaguing the United States will continue to progress unless a thorough examination of current medical opioid administration and prescribing practices is conducted and acted upon. Of the 70 630 drug overdose deaths in the United States in 2019, 70% involved an opioid. 1 Prescription opioids are commonly dispensed for chronic pain, a condition reported by 126.1 million Americans in 2012. The highest-volume prescribers of opioids are classically primary care providers, internists, dentists and orthopedic surgeons. 2 Typically, opioid abusers access hydrocodone- and oxycodone-containing medications from legitimate prescriptions written for themselves or family members/friends. 2 Around 80% of illegal opioid use starts with legitimately prescribed opioids. 3 This further necessitates proper tracking and monitoring of opioid prescribing and administration. If current opioid prescribing practices continue unchecked, these patterns of abuse and misuse will continue to exert ill effects at the national and global level, driving high incidence of opioid-related fatalities which are not limited to a single country, culture, race or socioeconomic status. 4
Recent data has shown that chronic back pain has become a major driver of opioid consumption. 3 It affects more than 26 million Americans between the ages of 20 and 64 years, and it is the leading cause of disability for those under 45 years of age. 5 Lumbar fusion surgery is the most common spinal fusion surgery intended to relieve this chronic back pain, radiculopathy, and/or claudication to improve quality of life. 3 Between 2001 and 2010, there were more than 3.5 million spinal fusion procedures performed, 6 and the rate of surgery for lumbar degenerative disc disease has increased 2.4-fold. 7 Though these procedures may provide pain relief adequate to discontinue chronic opioid use, the immediate post-operative period is marked by surgical pain which is also often managed with opioid analgesics. Higher costs of lumbar fusion surgery have been attributed to opioid-related complications such as an increased length of stay (LOS), respiratory depression, ileus, urinary retention, nausea and vomiting, 3 despite the fact that studies have shown there is no strong scientific evidence opioids are effective for chronic non-cancer pain. 4
As medicine and technology continue to advance, there have been more options for a minimally invasive spine surgery. There have been reported benefits of MIS Transforaminal Lumbar Interbody Fusion (TLIF) over traditional Anterior Lumbar Interbody Fusion (ALIF) and Lateral Lumbar Interbody Fusion (LLIF) procedures such as a decreased LOS, lower blood loss, and improved patient-reported outcomes. 7 However, little is known about differences in post-operative inpatient pain management and associated opioid administration among different spinal fusion approaches. In order to evaluate whether MIS may also be associated with less postoperative pain and potentially lower opioid consumption as compared to traditional approaches, this study aims to provide a high-level assessment and comparison of the amounts of opioids consumed during a post-operative hospital stay after different lumbar spinal fusion surgeries. We hypothesize that MIS TLIF will have a lower associated inpatient opioid consumption as compared to traditional ALIF and LLIF procedures.
Materials and Methods
Study Design and Inclusion Criteria
This study is a retrospective cohort study conducted at a single, large, urban, academic institution. The included patients are adults (≥18 years-old) who underwent primary one-level ALIF, LLIF or TLIF between 2012 to 2020, and who had been diagnosed with Grade I or II spondylolisthesis, lumbar spinal stenosis, severe degenerative disc disease or pars defect. All procedures were primary elective surgeries. Patients were excluded for higher-grade spondylolisthesis diagnosis and significant comorbidities including cancer, systemic bone, or joint diseases, and active or recent drug or alcohol abuse.
The patient cohort was categorized based on surgical approach. The TLIF cohort was divided into Minimally Invasive (MIS) TLIF and Open TLIF. Both ALIF and LLIF procedures were divided into Single Position (SP), Traditional Percutaneous (TP) or Open groups. Single Position procedures indicate that the patient was operated on in the lateral decubitus position, which avoids having to change patient positioning during the procedure as per convention. TP and Open ALIF and LLIF procedures differ from the SP procedures because they involve an anterior approach in the supine position followed by a posterior approach in the prone position; the TP and Open approaches differ from each other in that the Open procedures involve ALIF/LLIF with a flip followed by posterior decompression with instrumentation and fusion. SP ALIF and SP LLIF procedures were combined into one group (SP ALIF/LLIF). This was also done for the TP ALIF and LLIF patients (TP ALIF/LLIF) and the open ALIF and LLIF patients (Open ALIF/LLIF) to create cohorts for traditional percutaneous and open approaches as well.
This study was approved prior to data collection by the New York University Grossman School of Medicine Institutional Review Board under IRB #18-00668. It was approved for a Waiver of Consent, granting exemption from informed consent requirement, due to the retrospective nature of data collection.
Data Collection and Outcome Measures
Patient demographics, clinical characteristics, and outcomes were extracted from electronic medical records. Demographics included patient age, gender, BMI, and CCI. Additional characteristics included history of a psychiatric diagnosis of mood disorder or anxiety disorder, pre-operative narcotic use, pre-operative injection administration, and patient-reported radiculopathy. Pre-operative injection administration is defined as a patient who received a lumbar epidural steroid injection to help alleviate back or leg pain. Psychiatric diagnoses include depression, anxiety, panic disorder, and bipolar I disorder. Surgical factors included operative time, estimated blood loss, and fusion level. Postoperative outcomes included length of stay, incidence of ileus, total oral Morphine Milligram Equivalents (MME), Total MME/Hour, daily averages of opioid administration, total patient-controlled analgesia (PCA) received and average daily non-opioid medication administrations. MME calculations were made in accordance with conversion factors set forth by the Centers for Medicare and Medicaid Services and prior literature.8,9
Statistical Analyses
Descriptive tests were applied to compare demographics and clinical characteristics. One-way ANOVA with post-hoc Tukey Test was used to compare continuous variables between patients who received different lumbar spinal fusion procedures. Kruskal–Wallis and Mann–Whitney tests were performed to demonstrate differences in categorical variables between all the groups. All statistical analyses were conducted using IBM SPSS (version 25). Significance was defined as P < .05 for all analyses.
Results
Baseline Characteristics
Comparison of Baseline Patient Demographics Between the Different Spinal Fusion Approaches. All Values are Reported as Mean ± Standard Deviation.
Perioperative Characteristics
Comparison of Perioperative Characteristics Between the Different Spinal Fusion Approaches. All Values are Reported as Mean ± Standard Deviation.
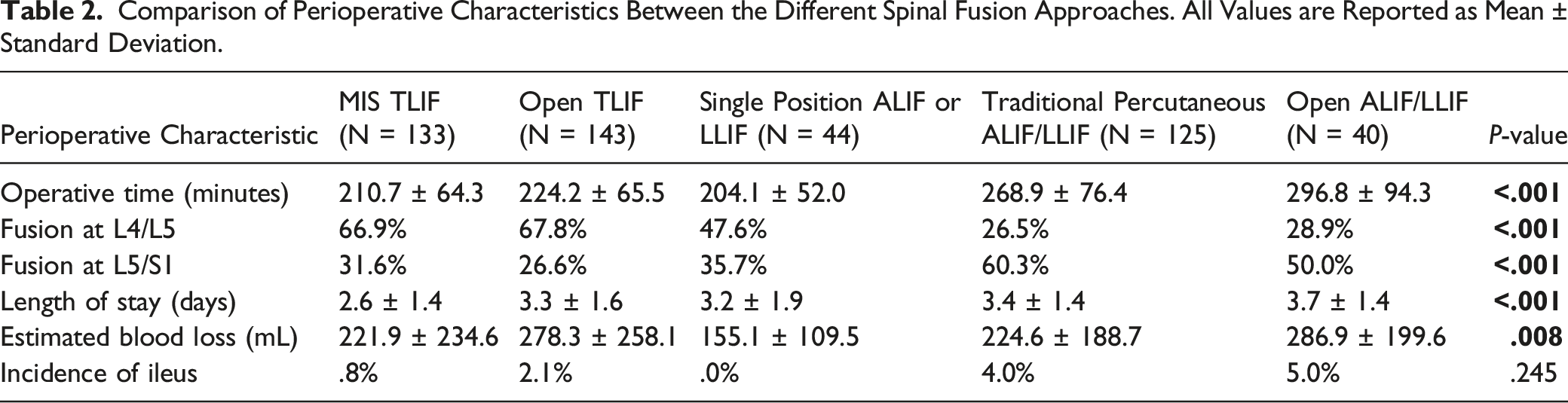
Additionally, there were differences among the groups in terms of how many procedures took place at the L4/L5 level (P < .001) and L5/S1 level (P < .001) as shown in Table 2. Further evaluation of the number of procedures that took place at the L4/L5 level revealed that there were differences between MIS TLIF and TP ALIF/LLIF(66.9% vs 26.5%, P < .001), MIS TLIF and Open ALIF/LLIF(66.9% vs 28.9%, P < .001), Open TLIF and TP ALIF/LLIF(67.8% vs 26.5%, P < .001), and Open TLIF and Open ALIF/LLIF(67.8% vs 28.9%, P < .001). Differences in percentage of procedures performed at the L5/S1 level occurred between MIS TLIF and TP ALIF/LLIF(31.6% vs 60.3%, P < .001), Open TLIF and TP ALIF/LLIF(26.6% vs 60.3%, P < .001), Open TLIF and Open ALIF/LLIF(26.6% vs 50.0%, P = .045), and SP ALIF/LLIF and TP ALIF/LLIF(35.7% vs 60.3%, P = .006).
Opioids in MME
Comparison of Total Daily Doses Between the Different Opioids for the Different Spinal Fusion Approaches. All Values are Reported as Mean ± Standard Deviation.
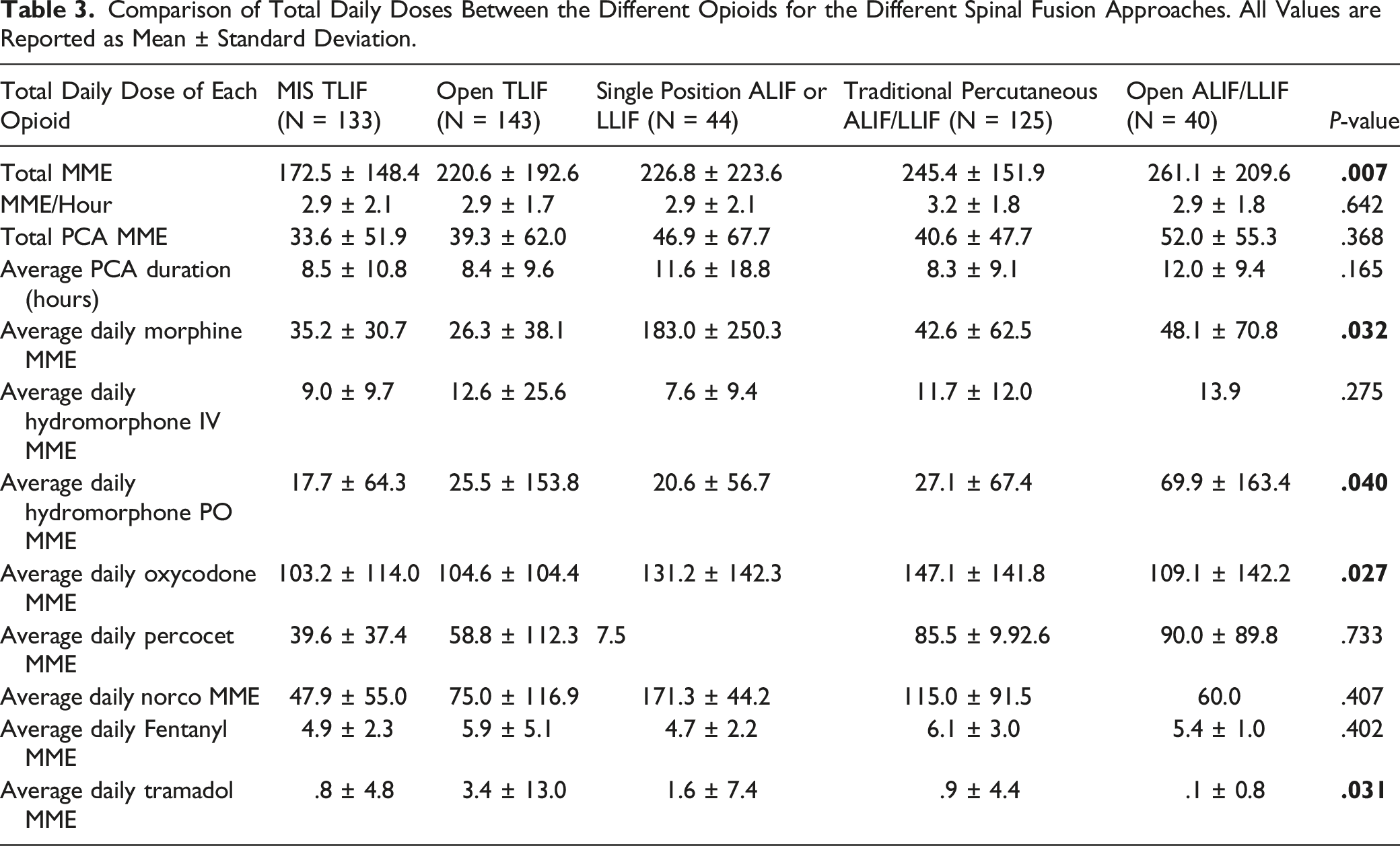
There were differences in inpatient consumption of different types of opioids, also shown in Table 3. These differences were administration of morphine (P = .032), oral hydromorphone (P = .040), oxycodone (P = .027), and tramadol (P = .031). A post-hoc Tukey test revealed that SP ALIF/LLIF had a larger inpatient consumption of morphine compared to MIS TLIF (P = .031), Open TLIF (P = .012), and TP ALIF/LLIF (P = .034). Open ALIF/LLIF had a larger inpatient consumption than MIS TLIF of oral hydromorphone which approached significance (5.7 MME vs 19.9 MME, P = .060). It was also found that TP ALIF/LLIF had significantly higher inpatient consumption of oxycodone compared to Open TLIF (147.1 MME vs 104.6 MME, P = .043) and compared to MIS TLIF (147.1 MME vs 103.2 MME, P = .038). Further analysis showed that the difference in daily tramadol between Open TLIF and MIS TLIF patients approached significance (3.4 MME vs .8 MME, P = .060).
Non-Opioid Use
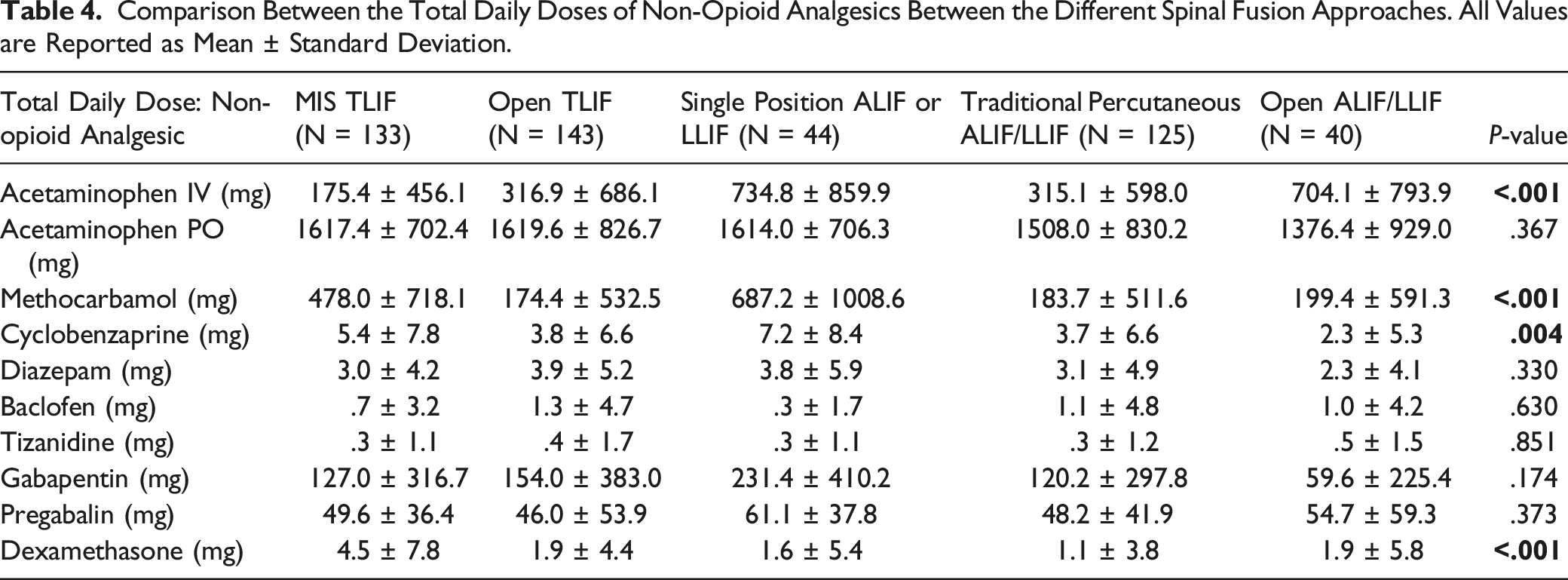
Comparison Between the Total Daily Doses of Non-Opioid Analgesics Between the Different Spinal Fusion Approaches. All Values are Reported as Mean ± Standard Deviation.
Discussion
Spine surgery is often highly associated with higher postoperative pain. 10 As minimally invasive approaches to spine surgery become more common, evaluating associated trends in opioid consumption during the inpatient stay may allow for a better understanding of how post-operative pain management differs by surgical approaches. However, there is a paucity of literature comparing inpatient narcotic use among different spinal fusion approaches. This study provides an analysis and comparison of inpatient opioid administration after a variety of surgical approaches to lumbar fusion.
Our results show that MIS TLIF is associated with a significantly lower total inpatient opioid consumption compared to TP ALIF/LLIF and Open ALIF/LLIF. However, when converted to a rate of MME/hour to account for differing LOS, we found similar rates of opioid consumption across all procedure types; thus, the decrease in MME consumed by MIS TLIF patients may be in part driven by a shorter associated inpatient LOS, rather than decreased pain. Data analysis from the present study showed that MIS TLIF similarly had a significantly shorter LOS compared to all other procedures except SP ALIF/LLIF. The shorter LOS associated with the MIS approach is well-supported by prior literature, which has shown better outcomes for both LOS and EBL, particularly for TLIFs. 11 Interestingly, our findings are discrepant with those reported by Hockley et al, who assessed inpatient MME and opioid usage after hospital discharge for MIS and Open TLIF procedures from 2014 to 2017 at the same study institution 7 . Their results showed that MIS TLIF procedures have lower total inpatient opioid consumption compared to Open TLIF (167 vs 255), whereas we found a non-statistically significant difference between total MME between MIS TLIF and Open TLIF (172.5 vs 220.6). 7 The discrepancy in statistical significance may be the result of differing institutional opioid prescribing protocols. At the present study institution, routine procedure is to use multimodal analgesia and consult the institution’s pain management team as necessary. Further inquiry into trends in opioid usage for these lumbar fusion approaches before and after implementation of this protocol is necessary to elucidate whether this is an intervening confounding factor; these studies are currently underway.
Another dynamic which may influence total and per hour inpatient opioid consumption is the utilization of patient-controlled analgesia (PCA), a protocol which allows the patient to deliver whenever they find it appropriate a physician-ordered dose of the analgesic in order to best control their pain. 12 At the study institution, PCA protocol is initiated in the immediate post-operative period; then, in the morning of post-op day 1, PCA is discontinued in favor of oral analgesics. Across all cohorts, patients in this study had similar duration of PCA as well as levels of opioid consumption during the PCA period. Though the literature suggests that PCA is associated with significantly higher opioid consumption, the benefit it provides to patients in terms of pain control is still unclear. Some studies have found that postoperative PCA, while associated with significantly more opioid consumption in the first 72 hours after lumbar spinal fusion surgery, still yields equal or worse postoperative pain scores compared to nurse controlled analgesia. 13 However, a contradicting study by McNicol et al found that, at the expense of higher opioid consumption, patients are more satisfied and have lower VAS pain intensity scores. 14 Further research is necessary to more fully characterize the role PCA has in post-operative pain management.
In addition to opioid consumption, we assessed consumption of non-opioid pain management medications during the post-operative inpatient period, which showed significant differences in the total amounts of IV acetaminophen, methocarbamol, cyclobenzaprine, and dexamethasone administered. Providing non-opioid analgesics alongside opioid analgesics has been put forth as a multimodal approach to post-operative pain management which may curtail opioid consumption while still providing adequate analgesia to the patient. 15 This approach has been found to better improve pain control, reduce hospital narcotic consumption, and provide better functional outcomes.15-17 Such multimodal approaches include combined use of opioid alternative medications such as steroids, gabapentinoids, local anesthetics, acetaminophen and other neuromodulatory pharmacologic agents.17,18 Though existing literature suggests the effectiveness of a multimodal approach, there is still a lack of literature demonstrating an optimal postoperative protocol. 15 The lack of evidence-based guidelines for an optimal multimodal approach may partially explain the differing rates of certain non-opioid analgesics observed in this study, as other factors such as surgeon preference, nursing assessment, and patient characteristics may drive decision-making instead.
IV acetaminophen in particular is a non-opioid analgesic which has been of interest for its effect on post-operative pain control. Hansen et al 19 demonstrated that higher doses of IV acetaminophen led to less resource use, lower costs, lower doses of opioids and improved discharge status of spine surgery patients compared to oral acetaminophen. 19 In contrast, this study shows the opposite effect: MIS TLIF patients had the lowest inpatient MME and the lowest IV acetaminophen, while SP ALIF/LLIF patients had the highest inpatient MME yet received the most IV acetaminophen. While this may be a true discrepant result, it could also be a result of differing amounts of other non-opioid analgesics such as dexamethasone and methocarbamol, which were significantly higher in the MIS TLIF group compared to the SP ALIF/LLIF group. Of interest, IV acetaminophen use after Open TLIF was greater than for MIS TLIF, though this difference was not statistically significant (316.9 mg vs 175.4 mg, P=.350). This might potentially explain the non-significant difference between total MME for MIS TLIF vs Open TLIF seen in prior evaluations of post-op opioid consumption at this institution. More standardized approaches to multimodal use of non-opioid analgesics may be necessary to more accurately assess the role of IV acetaminophen in post-operative pain management after lumbar fusion procedures.
In addition to total MME, the present study assessed the contribution of specific opioid analgesics to total opioid consumption. Hydromorphone, oxycodone, and tramadol differed significantly across the cohorts, with MIS TLIF showing lowest consumption of these medications. Of those that differed significantly, oral oxycodone had the largest contribution to the MME total in this study aside from opioid consumption during the PCA period. TP ALIF/LLIF had the largest amount of oxycodone consumed and MIS TLIF had the lowest. The significant role of oral oxycodone in post-operative pain management is likely due to its proven efficacy at offering great pain relief compared to other modalities of pain medications, especially when paired with acetaminophen. 20 For spine surgery in particular, Cheung et al 21 determined that compared to IV opioids, oral oxycodone provided better or comparable pain relief, while also not prolonging hospital stay and while decreasing drug costs. 21
The present study is not without limitations. As is the nature of retrospective studies, there are characteristics differing across cohorts which are unable to be controlled for, such as higher rates of surgery at L5-S1 for anterior procedures, varying rates of pre-operative narcotic and injection use, and small differences in approach among different surgeons. Additionally, though all included patients received analgesics according to the institution’s standardized opioid prescribing procedure, which involves multimodal analgesia and consultation with the institution’s pain management team, there may be some variation in dosing of both opiate and non-opiate pain management medications based on individual patient post-operative course, particular approach used for lumbar fusion, and surgeon and nurse assessment. Demographically, there were some significant differences in age, pre-operative narcotic use, and pre-operative injection use between approach cohorts. In particular, future prospective studies should assess the impact of quantified pre-operative narcotic use on tolerance affecting post-operative opioid needs. Despite these statistical discrepancies, these differences may not be clinically significant. The average age across all cohorts was in the 5th decade of life; a minority of patients across all cohorts reported pre-operative narcotic use, and pre-operative injection use hovered roughly around 50% across all cohorts. Specifically, pre-operative narcotic use in the MIS TLIF group was not significantly different compared to any other cohort. Future studies may benefit from a prospective design allowing for control of some of these variables.
Comparing drug administration for both opioid and non-opioid analgesics after lumbar fusion surgeries allows for a better understanding of rates of administration overall as well as for particular surgical approaches. Results from the present study as well as others may better enable the design of pain management protocols after spinal surgery to reduce the harmful effects of long-term opioid usage. The data from this study suggests that the MIS TLIF approach yields the lowest associated MME consumption, potentially mediated by a shorter associated inpatient stay as compared to other lumbar fusion approaches, rather than decreased pain inherently associated with the MIS approach to TLIF.
Conclusion
There remains much work to be done, especially in the field of orthopedic surgery, to bring an end to the opioid epidemic. This study adds to the body of knowledge regarding evidence-based opioid analgesic protocols that provide satisfactory pain control while limiting the harmful effects of opioid consumption. From this analysis, MIS TLIF procedures were shown to have lower inpatient MME than single position ALIF/LLIF and traditional percutaneous ALIF/LLIF, and comparable amounts to open TLIF and open ALIF/LLIF. Further prospective studies with larger sample sizes to evaluate pain scores and opioid consumption rates are necessary to solidify that there is a true difference between the groups in terms of opioid consumption after single-level lumbar spinal fusion surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.