
Abstract
Introduction:
Computer-assisted navigation (CAN) is a well-established tool in spinal instrumentation surgery. Different techniques – each with specific advantages and disadvantages – are used in the cervical spine.
Methods:
A structured summary of different spinal navigation techniques and a review of the literature were done to discuss the advantages and disadvantages of specific navigation tools in the cervical spine.
Results:
In cervical spine surgery, CAN increases the accuracy of pedicle screw placement, reduces screw mispositioning and leads to fewer revision surgeries. Due to the mobility of the cervical spine, preoperative CT followed by region matching or intraoperative CT are recommended.
Conclusions:
CAN increases pedicle screw placement accuracy and should be used in spinal instrumentation for the cervical spine whenever possible.
Introduction
Computer-assisted navigation (CAN) is a well-established tool in spinal instrumentation surgery. It was developed to improve the safety and accuracy of pedicle screw placement while eliminating the need for intraoperative X-ray. Registration of pre- and/or intraoperative spinal imaging data with the intraoperative anatomy provides the surgeon with immediate visual feedback, as the planned position of the pedicle screw can be visualized embedded in the patient’s imaging. Thereby, complications potentially associated with mispositioning of the screws, such as revision surgeries, instability, implant failure, or new neurological deficits are supposed to be reduced. 1 In the cervical spine, the accuracy of pedicle screws is even more important than in the thoracolumbar spine, as pedicles are smaller and even the slightest deviation from the ideal trajectory will either lead to damage of the spinal cord (in case of a too medial screw position) or to injury of the vertebral artery (in case of a too lateral screw position). Consequently, the use of CAN is essential in the cervical spine. 2,3 Apart from screw positioning, CAN is also employed in spine tumour surgery, permitting an optimized extent of resection through image guidance while reducing trauma by smaller surgical exposure. 4,5
This article illustrates the advantages and disadvantages associated with the use of CAN in the cervical spine. Different CAN systems are discussed based on a review of the literature.
Different techniques of CAN
Apart from different navigation hard- and software systems, CAN can also be categorized based on the timing and modality of imaging.
Preoperative CT imaging
Preoperative CT imaging can be used for intraoperative navigation. It requires registration of the imaging data with the in-situ anatomy. For this, after exposure of the region of interest, a point-by-point sampling of predefined anatomical landmarks, e.g. the surface of the lamina of a vertebra, is done with a navigation probe. The digital representation of that surface is then matched (registered) with the corresponding surface detected semi-automatically within the preoperative CT scan by the navigation software (‘region matching’, see Figures 1 and 2). 2 –6
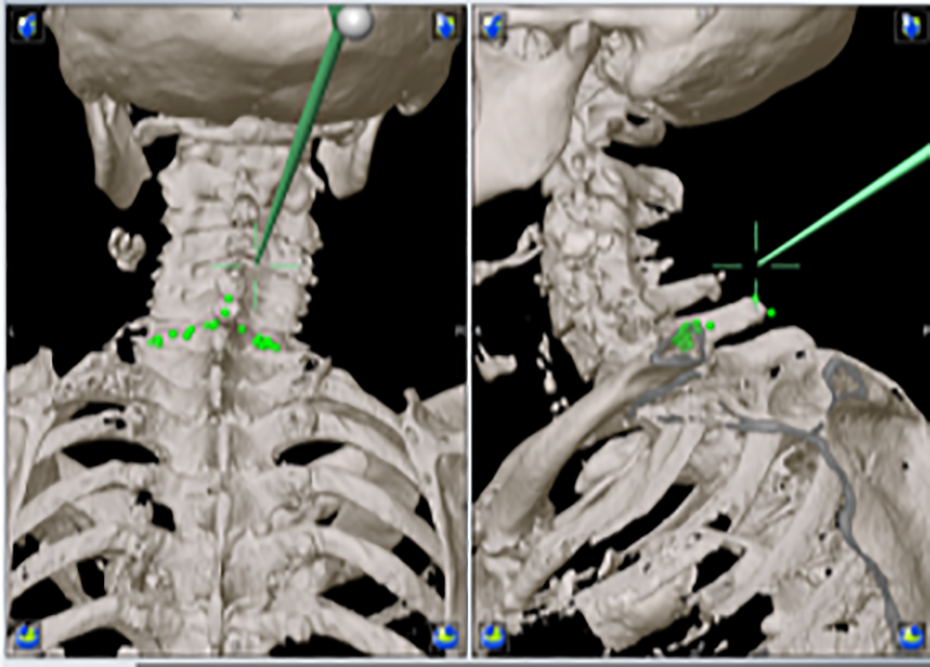
Point-by-point sampling of the C7 lamina for preoperative CT region matching registration (from Meyer and Ryang 7 ).

CT region matching-based placement of a pedicle screw. The projection of the current drill guide trajectory onto the axial (bottom left) and sagittal (bottom right) imaging planes as well as the probe’s view (top right) permits ideal positioning of the screw (from Meyer and Ryang 7 ).
A major advantage of this technique is the high quality of the preoperative CT scan. Given that at the cervical spine, pedicles are relatively small and relevant structures that are to be preserved are close (e.g., vertebral artery, spinal cord), the best possible imaging quality should be employed. Moreover, since there is no need for intraoperative imaging prior to instrumentation, this method potentially reduces operative time. This benefit may be counteracted by the fact that, due to the differences between positioning in the OR vs. positioning during the preoperative CT, every spinal level has to be registered individually before pedicle screw placement when using region matching. However, this is not really a disadvantage of the method: Since every screw insertion potentially leads to relative movements between individual vertebrae due to the high mobility of the cervical spine, re-registration is usually also required when using intraoperative imaging for navigation in the cervical spine, and in this case, this even requires additional imaging scans and thus leads to higher radiation exposure of the patient.
As a downside of navigation with preoperative CT imaging, a vast surgical exposure of bone surfaces is required for registration which rules out percutaneous or minimally invasive techniques.
Intraoperative 3D-fluoroscopy
When intraoperative 3D fluoroscopy is used for navigation, a reference array is placed in situ and detected by the navigation software in the intraoperative images. 8 –10 This enables automatic registration and permits smaller exposure than required for region matching. As the staff can leave the operating room during the 3D scan, there is no radiation exposure, which is a substantial advantage compared to instrumentation surgery employing intraoperative X-ray. The different systems available come with different image qualities and sizes of the field of view. In general, both are inferior to intraoperative or preoperative CT, but some provide imaging quality that is sufficient even for the cervical spine in most cases. However, when the field of view and imaging quality must be maximized (e.g., severe osteopenia, obese patients, long cervicothoracic instrumentations), CT is the modality of choice.
Intraoperative CT
Intraoperative CT combines the advantages of automatic registration, high image quality and the largest field of view. 11,12 Moreover, radiation exposure can be completely eliminated for the OR personnel, although for the patients it is substantially higher than with 3D fluoroscopy. 13,14 Modern mobile CT units image the entire spine and pelvis with relatively low radiation exposure in one single scan, saving operative time compared to other intraoperative imaging systems. The high image quality also permits image-guided decompressions and tumour resections in addition to pedicle screw placements. However, these systems are currently very expensive, and therefore not yet widely used.
Benefits of CAN in surgery of the cervical spine
CAN holds numerous advantages for spinal instrumentation surgery. The safety of CAN and the increase of accuracy in screw placement associated with CAN have been widely accepted. 14 –17 There are many studies investigating the effect of different CAN techniques on screw placement accuracy specifically for the cervical spine (for an overview, see Table 1). Among these are several comparative studies showing that CAN significantly reduces the rate of misplaced screws compared to freehand placement. 18 –23 This advantage appears to be even more evident in the cervical spine than it is in the thoracic or lumbar spine. 16,26 and it has been found for the upper cervical spine 22,30 and the subaxial cervical spine 19,20 as well as for lateral mass screws and pedicle screws. 18,19,21 The latter is of special importance given that even though pedicle screws provide the benefit of increased primary stability in the cervical spine, 40 they are often omitted in favour of lateral mass screws due to the high risk for injury of adjacent structures (vertebral artery, dura/spinal cord) in freehand cervical spine pedicle screw placement. In fact, with CAN, this difference between lateral mass screws and pedicle screws may disappear: Operation times and rates of complications, such as vertebral artery injury, spinal cord injury and nerve root injury, were comparable for lateral mass screws versus pedicle screws in a study using surface matching navigation. 2
Overview of studies including screw type, misplacement rates and navigation technique.

* ioCT: intraoperative CT; FH: freehand placement; io3DFL: intraoperative 3D fluoroscopy; RM: region matching.
Only few studies directly compared different CAN techniques in the cervical spine (Table 1). Two studies compared preoperative CT/region matching with ioCT for pedicle screws, both supporting that ioCT is superior to region matching with regard to screw placement accuracy (misplacement rates of 0 vs. 4% and 3 vs. 6%, respectively). 22,23 Other studies using ioCT only or in comparison with freehand placement reported pedicle screw misplacement rates ranging between 2 and 12%. 1 7 –19,25,26 This appears to be slightly superior to intraoperative 3D fluoroscopy with pedicle screw misplacement rates ranging between 3 and 20% 27 –30,32 –38 ; direct comparisons, however, are lacking.
Regarding complication rates and patients’ outcomes using CAN in the cervical spine, a meta-analysis of 5,992 pedicle screws showed no neurological complications in the navigation group and a trend towards more complications in the non-navigation group. 41 Another meta-analysis found significantly lower complication rates associated with mispositioning of screws in the CAN group than in the freehand group. 16 The rate of revision surgeries due to screw mispositioning was shown to be significantly reduced with CAN in the thoracolumbar spine 42,43 ; studies investigating revision surgeries for screw mispositioning in the cervical spine are lacking.
Regardless of the spinal region, CAN also permits minimally-invasive and percutaneous pedicle screw placement. An accurate navigation eliminates the need for a large exposure of bony surfaces and/or the use of X-ray. Several studies including a prospective randomized controlled trial could show that radiation exposure of the surgeon during freehand pedicle screw placement is up to 10 times higher than with the use of navigation (intraoperative 3D fluoroscopy), which comes along with a decreased radiation exposure of the patient. 44,45
Furthermore, CAN enables image-guided tumour resections, aiding the surgeon in sparing relevant structures nearby and in minimizing the exposure. 4,5,46
As CAN is associated with a learning curve that has to be overcome, we and others have argued for a routine use of CAN in every case of spinal instrumentation. 47 –49
Conclusion
CAN is a useful tool in spinal surgery that potentially improves patient outcomes by increasing the accuracy of screw positioning. This is of particular importance in the cervical spine where delicate structures are close and mobility is high. CAN paves the way for safe and stable pedicle screw instrumentations of the cervical spine. It also leads to a reduced radiation exposure of the patient as well as the OR personnel and can support tumour resections and less invasive approaches for instrumentation surgeries. In order to overcome the learning curve, it is recommended to apply CAN not only for the most complex cases, but as part of daily routine.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.