
Abstract
Study Design:
This is a technique paper describing minimally invasive, navigated, percutaneous pedicle screw fixation of the cervical spine. In addition, we include a retrospective feasibility analysis of our initial experience with 27 patients undergoing this procedure.
Objective:
The purpose of this study is to describe the technique of MIS navigated percutaneous cervical pedicle screw instrumentation and to report our initial experience.
Methods:
This is a retrospective review of 27 patients undergoing MIS navigated percutaneous posterior cervical pedicle screw fixation at 2 institutions. We describe the technique and report the radiographic outcomes and all intraoperative and postoperative complications.
Results:
A total of 27 patients underwent MIS navigated percutaneous pedicle screw fixation. Indications included odontoid fracture, subaxial fracture dislocations and burst fracture, pathological fracture, and degenerative spondylosis. There were no nerve root or vascular injuries. There were no spinal cord injuries. Two screws required repositioning intraoperatively, and 1 patient required reoperation for symptomatic malpositioned screw.
Conclusions:
MIS navigated percutaneous posterior pedicle screw fixation can be performed safely. These constructs are biomechanically superior with neurovascular complication rates comparable to traditional lateral mass screw technique. While the current indications for this technique are relatively limited, the evolution of MIS cervical decompression techniques as well as navigation and robotics will provide an expanded role for percutaneous cervical pedicle screw instrumentation.
Introduction
The history of posterior cervical spine fixation includes a broad range of instrumentation techniques. This includes sublaminar wiring, lateral mass fixation, translaminar fixation, and open pedicle screw fixation.1-4 Each of these techniques has its advantages and limitations as it relates to biomechanical strength, exposure morbidity, and the ability to achieve concomitant decompression. Posterior cervical fixation poses several challenges when compared to thoraco-lumbar fixation, including smaller cervical vertebrae as well as the proximity of spinal cord, nerve root, and vertebral artery. These anatomic constraints require precise instrumentation placement. Accordingly, adoption of minimally invasive surgery (MIS) in the cervical spine, with the exception of decompression with minimally invasive laminoforaminotomy, has lagged behind the thoracolumbar spine. 5 Recent advancements in intraoperative imaging, navigation, and robotic technology have facilitated the development of safe and efficacious MIS posterior cervical fixation. 6
Cervical pedicle screws are biomechanically superior to traditional lateral mass screw fixation. 7 Pedicle screw fixation is the standard of care in the thoracic and lumbar spine, but cervical pedicles are smaller in size with a smaller medullary diameter increasing the difficulty of pedicle screw placement. 8 Additionally, pedicle breach of just a few millimeters can result in encroachment on the vertebral artery, nerve root, or spinal cord.9,10 Lastly, cervical pedicles have an extreme lateral to medial trajectory, up to a mean C5 pedicle medial angulation of 46 degrees. 8 This medial to lateral angle requires a wide and morbid exposure to perform traditional open cervical pedicle screw fixation. This exposure results in significant wound morbidity due to the denervation and atrophy of the paraspinal musculature and disruption of the posterior ligamentous complex.
The O-arm imaging system was introduced in 2006 (Medtronic, Minneapolis, MN). The O-arm provided the first mobile, intraoperative cone beam computed topography (CT) navigation capability. The efficiency and accuracy of instrumentation placement with the O-arm has facilitated adoption of intraoperative navigation.11,12 MIS percutaneous cervical pedicle screw fixation can be performed safely due to advances in intraoperative imaging efficiency and the accuracy of modern spinal navigation systems. These technical advances reduce the risk to adjacent neurovascular structures. Performing this technique percutaneously circumvents the drawback of the morbidity of traditional open cervical pedicle screw placement.
Methods
This is a retrospective review of 27 patients who underwent MIS navigated percutaneous cervical pedicle screw fixation. This represents a consecutive series of patients at 2 separate institutions with 3 surgeons. No patients undergoing percutaneous pedicle screw placement were excluded from the study. All patients had a minimum of 3-month follow-up. Each patient had either 2D or 3D post-operative imaging and serial radiographs.
Patients were selected at the discretion of the treating surgeon. Considerations included the necessity for posterior fixation if used in combination with an anterior procedure, necessity for posterior decompression, cervical pedicle size, vertebral artery anatomy, or significant alignment issues. In addition, wound morbidity risk factors such as diabetes and renal disease were considered. Once the decision to pursue percutaneous screw fixation was made, there were no instances where percutaneous fixation was abandoned in favor of open fixation. This was a case series of our initial experience and no patients were excluded that received percutaneous pedicle screws. Informed consent was obtained from all patients. This study was approved by the Atrium Health Institutional Review Board.
Technique
This MIS navigated percutaneous screw technique can be employed for placement of subaxial cervical pedicle screws as well as C2 pars or pedicle and C1 lateral mass fixation. The surgical prep and positioning for these patients is identical.
The patient is placed in Mayfield headframe and secured to a Jackson table in a neutral, prone position with a cervical management system. The posterior neck is prepped and draped sterilely. It is important to prep and drape very wide on the neck due to the unusually lateral position of the percutaneous incisions (Figure 1A). In addition, taping the shoulders down can better facilitate access to this area.
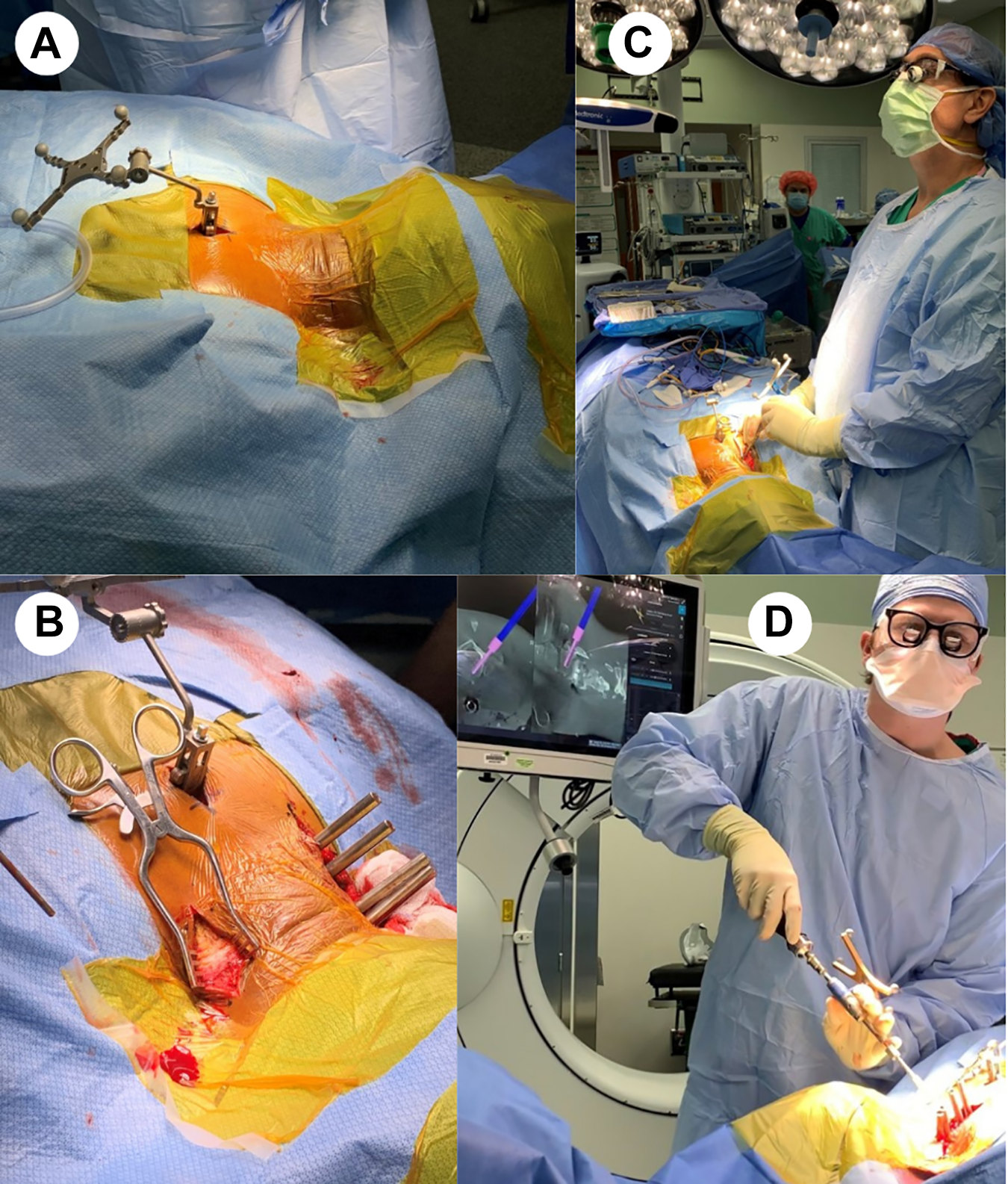
Navigated, MIS cervical pedicle screw technique.
A small 2 cm incision is then made at the spinous process of the lower instrumented vertebrae (LIV) minus 1. Subperiosteal dissection is performed and the spinous process clamp is placed and attached to the reference frame. Intra-op imaging is obtained with O-arm cone-beam CT. The navigated wand is used to determine the lateral skin entry point along the trajectory of the targeted cervical pedicles. Skin marker is used to connect these entry points into a straight line. The skin incision is made based on the individual patient anatomy based on pedicle trajectory. On average, the skin incisions are approximately 5 cm off the midline. Local anesthetic (0.5% Marcaine with epinephrine) is injected. The skin is opened down to the superficial cervical fascia and a small self-retaining retractor is placed (Figure 1B). Multiple percutaneous stab incisions can also be performed but we have found it cosmetically favorable to use one superficial skin incision and perform separate fascial stab incisions.
A combination of blunt dissection and monopolar electrocautery is used down to the lateral mass. Navigated wand and navigated drill are used to confirm appropriate entry point and trajectory. A high-speed drill with an MH80 matchstick drill bit is then advanced into the lateral mass along the trajectory of the pedicle. The drill is then advanced to the midpoint of the pedicle under navigation (Figure 1C). A 3.0 navigated power tap is then advanced through the pilot hole and into vertebral body. Screw size is determined using the navigation software. The navigated wand can be used as a pedicle probe to reassure there has been no breach. A navigated screwdriver is then used to place a cervical pedicle screw with reduction tower in the subaxial spine (Proficient Minimally Invasive System, PROMIS; Spine Wave, Shelton, CT) (Figure 2) or C1 lateral mass and C2 pars fixation (Figure 1D).
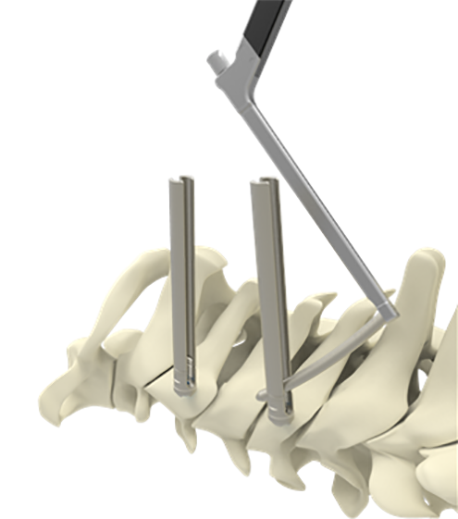
Proficient minimally invasive system, PROMIS; spine wave, shelton, CT.
All screws are placed bilaterally prior to rod placement to avoid introducing any alignment change that could affect navigation accuracy. Rods are then placed percutaneously through the reduction towers and tested to insure capture of each tulip head. Locking caps are placed and final tightened. The rod length can typically be visualized to confirm placement through the most cephalad screw. Final post-instrumentation imaging is then performed with intra-operative CT or 2D fluoroscopy.
There is a theoretical concern for decreasing accuracy with increasing distance from the reference frame. To minimize this, it is best to instrument furthest away from the reference frame and work toward it. This allows for placement of the furthest pedicle screw (and potentially the least accurate) before introducing additional risk of navigation inaccuracy (micromotion of the spine, inadvertent bumping or shifting of the reference frame, etc). In addition, this sequence provides the most efficient workflow, preventing the previously placed reduction towers from interfering with the navigated instruments.
C1-2 Fixation
C1 lateral mass and C2 pedicle screws are placed with a cranial reference frame placed onto the Mayfield attachment. Special care must be taken to avoid moving the OR table after O-arm images are obtained as this may introduce inaccuracy due to shift of the body in relation to the reference from which is rigidly fixed to the Mayfield.
Percutaneous C1 screws do not require sacrificing the C2 nerve root. Similar to the open technique, the screws can be placed with smooth a smooth shank to avoid C2 nerve root irritation. Avoiding the significant venous plexus to access the C1 lateral mass is an advantage of this percutaneous technique.
Results
Twenty-seven consecutive patients underwent MIS navigated percutaneous cervical pedicle screw instrumentation between January 2015 and May 2020 at 2 separate institutions. Indications for operation included Type II odontoid fracture, burst fracture, fracture dislocation, degenerative spondylosis, and pathological fracture from infection or tumor.
This study included 15 men and 12 women. The mean age was 63.5 years. The mean follow-up was 16.7 months (minimum 3 months, maximum 24 months). Eleven patients (41%) underwent an anterior decompression prior to posterior MIS fixation. Sixteen patients received posterior MIS fixation alone with or without decompression. Two patients (7%) required screw revision intraoperatively after imaging revealed pedicle breach. This included one C2 screw with a superior breach of the pars and one C5 screw which breached the pedicle medially. Both screws were repositioned without issue and without postoperative sequela. One patient (4%) required reoperation for screw repositioning after a patient was found have radicular shoulder pain due to foraminal stenosis from breach of the C5 pedicle. This screw was removed and the patient made a full neurological recovery. There were no reported spinal cord injuries, nerve root injuries, or vertebral artery injuries. In addition, there were no surgical site infections recorded in this series.
Case Study
A sixty-nine-year-old male presents with a C5 metastatic pathological burst fracture and myelopathy. CT of the cervical spine reveals a lytic fracture with posterior element involvement (Figure 3B and 3D). MRI of the cervical spine demonstrates ventral spinal cord compression (Figure 3A). The patient underwent a C5 corpectomy with an integrated static corpectomy cage and anterior plating (Figure 3C). Given the lytic involvement of the posterior elements, the patient undergoes supplemental posterior cervical fixation with C3-C7 percutaneous, navigated pedicle screw fixation. Figure 3A demonstrates the final intraoperative fluoroscopic image with screw reduction towers in place. Figure 3B and C show the AP and lateral upright postoperative films. The patient does not require a brace postoperatively and incisions are closed with adhesive skin glue (Figure 3D). Figure 4 demonstrates accurate placement of all 8 cervical pedicle screws, including bilateral 4.2 mm x 28 mm screws placed at C3 (Figure 5).
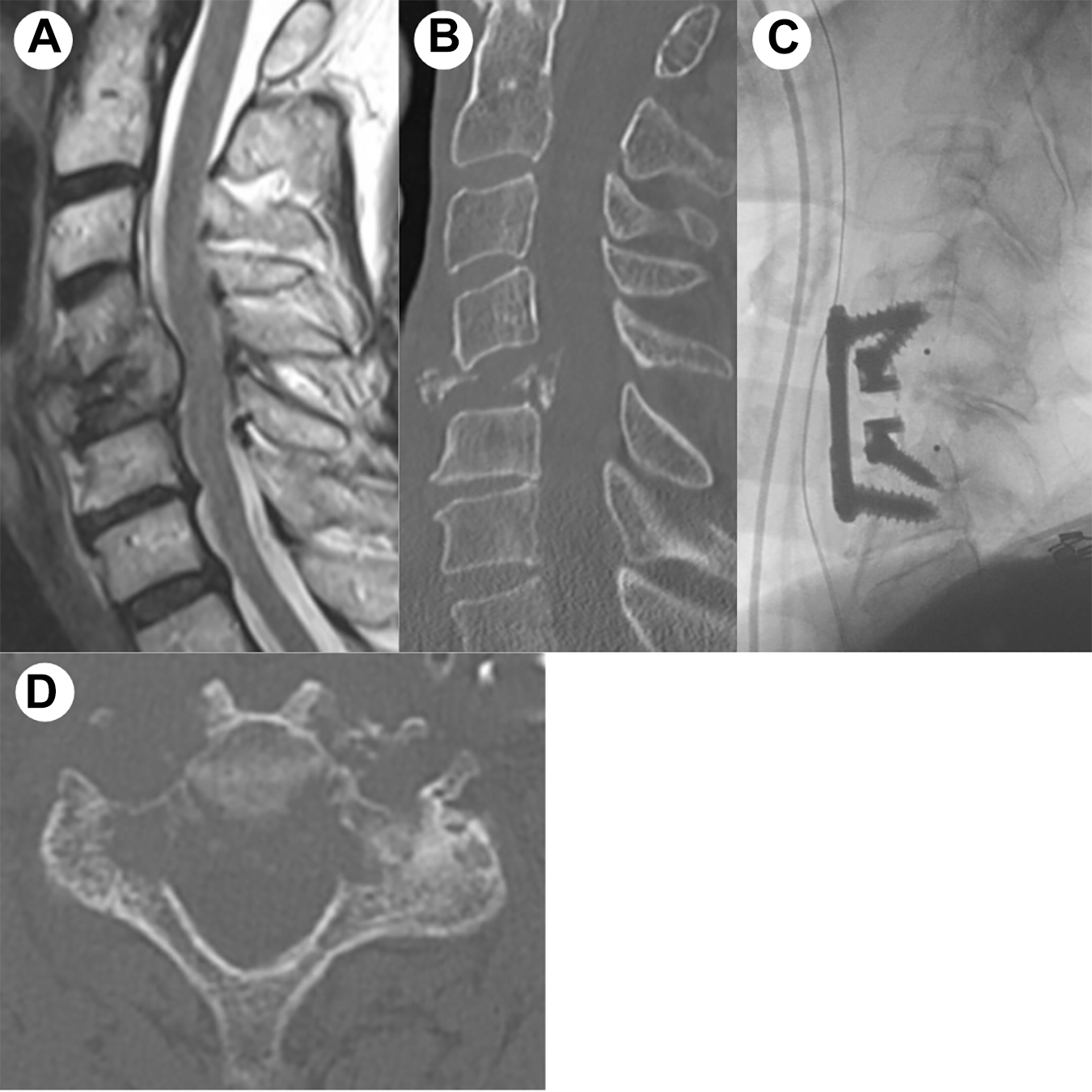
Case study-C5 pathological burst fracture.
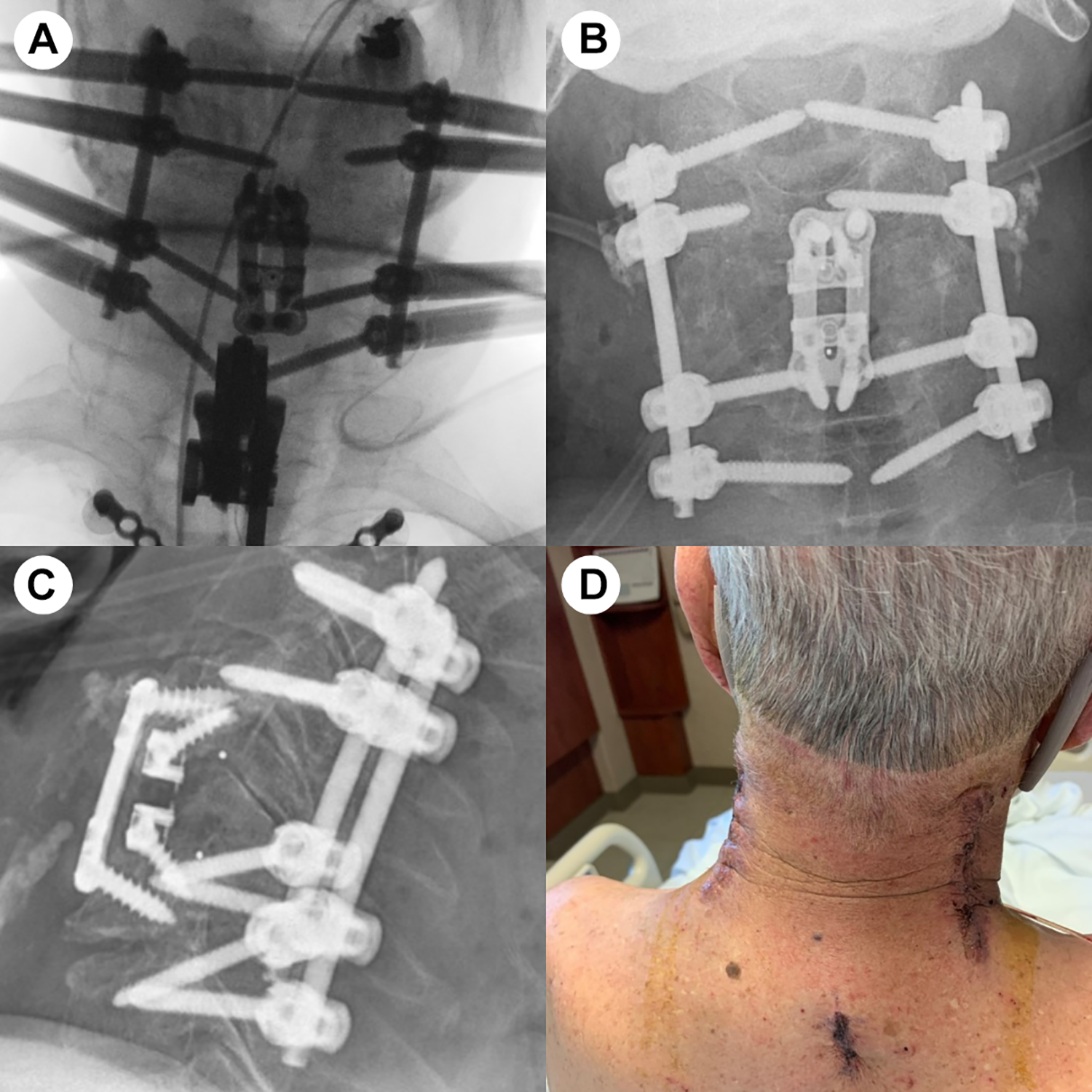
Case study-postoperative.
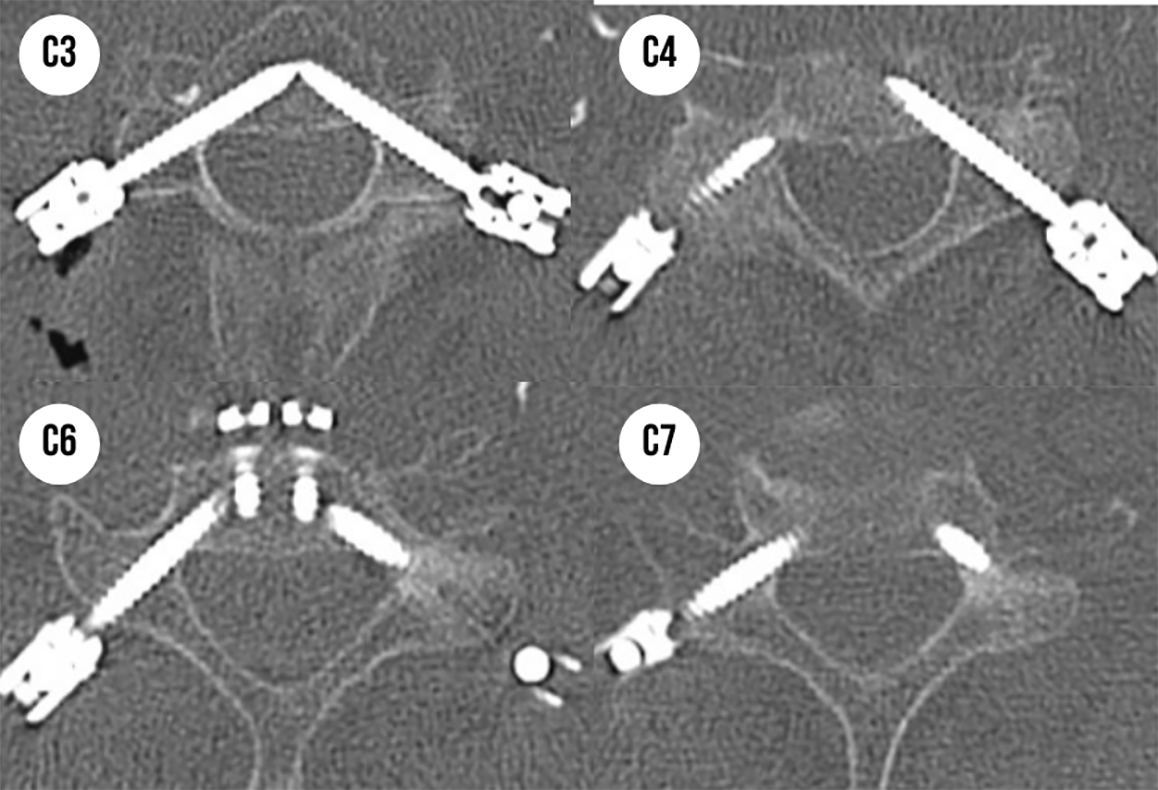
Case study-accuracy of cervical pedicle screw placement.
Discussion
This paper provides a technical description of an MIS navigated percutaneous posterior cervical pedicle screw technique and reports our initial clinical experience. The primary surgeons in this study each have over 5 years of experience with navigation and minimally invasive techniques.
Cervical pedicle screws provide significant biomechanical strength in comparison to traditional lateral mass screws. Lateral mass screws typically measure to be 3.5 mm in diameter with a length of 12 mm or 14 mm. Subaxial cervical pedicle screws can often accommodate screw diameters of 4.2 or 4.5 mm and lengths of 26, 28, or 30 mm. A cadaveric study by Johnston et al found that the pullout strength of a cervical pedicle screw was 4 times stronger than a lateral mass screw. 7 In addition, they noted that the mechanism of failure in the lateral mass screws was screw pullout from the bone versus complete fracture of the pedicle from the vertebral body in the pedicle screw cohort. 7
This biomechanically superior method of posterior cervical fixation has not been widely adopted due to the significant approach related morbidity and technical challenge of placing using the traditional open technique. With recent advancements in intraoperative imaging and minimally invasive techniques, these robust constructs can be utilized using a navigated, percutaneous minimally invasive technique. Additionally, this MIS technique preserves the posterior muscular neck stabilizers and musculoligamentous posterior tension band, further adding to stability, reducing postoperative neck pain, and wound morbidity. The benefit of these muscle and ligamentous sparing MIS techniques have been well described in the lumbar spine. 13
The existing literature regarding cervical pedicle screw placement is primarily focused on open C2 and C7 pedicle screw placement, owing to their larger diameter.14,15-17 The largest true percutaneous cervical pedicle screw series was performed in 15 patients using a fluoroscopic technique. 18 Placement using fluoroscopy has significant limitations due to the necessity of K-wires and additional retractors19-21 We present the largest series of navigated percutaneous cervical pedicle screw fixation cases. 6
Safety Considerations
Surgeons have been reticent to perform subaxial pedicle screw fixation from C3 to C6 due to the proximity of surrounding neurovascular structures. Tomasino et al performed a cadaveric study and identified the vertebral artery to be on average 1.1 -1.7 mm from the lateral cortex of the pedicle. 9 In a separate cadaveric study, Xu et. al identified the nerve root to be on average 1.4 -1.7mmm caudal to the inferior margin of the pedicle. 10 Despite these concerns, the literature does not suggest a significant difference in neurovascular complication rate in cervical pedicle screw placement as compared to the lateral mass screw placement.15-17,22 In addition, there has been no reported spinal cord injury from cervical pedicle screw placement. Heller et. al reported a large series of 784 lateral mass screws placed with an overall neurovascular complication rate of 0.92% 22 Abumi et al reported a series of 712 fluoroscopic cervical pedicle placements with an overall neurovascular complication rate of 0.42% 15 We found a low rate of neurovascular complication in our series with only 1 patient (3.7%) suffering a temporary neurological symptom (pain) which resolved with screw removal. With the evolution of intraoperative navigation and robotics, the rate of neurovascular complication with percutaneous cervical pedicle screw placement should be comparable to lateral mass screw fixation. Additionally, the increased biomechanical strength as well as the potential for reduced wound morbidity, and preservation of musculoligamentous stabilizers associated with percutaneous cervical fixation provide incentive to consider this technique in select patients.
Indications
The indications for percutaneous cervical instrumentation presented in this manuscript are relatively narrow. Severe traumatic cervical spine fractures, such as fracture-dislocations requiring combined anterior and posterior approaches, present a potentially ideal indication for this technique. Decompression and/or fracture reduction can be achieved with either traction or a limited anterior approach and, subsequently, combined with a robust posterior percutaneous fixation technique. Given the high prevalence of posterior wound morbidity in the spinal cord injury population, there may be a significant advantage associated with posterior percutaneous fixation in this population.
Patients with ventral compressive pathology requiring multi-level anterior cervical discectomy and fusion (ACDF) or anterior corpectomy can be supplemented with posterior fixation utilizing this technique. Patients with poor bony quality due to osteopenia, renal disease, infection, or diffuse oncologic processes are also potential candidates for robust supplemental MIS posterior fixation. This procedure can be performed immediately following the anterior procedure or staged in a delayed fashion.
Additional indications include neurologically intact patients with diffuse idiopathic skeletal hyperostosis (DISH) and unstable cervical fractures or patients with failed ACDF that require robust stabilization without decompression. Also, patients with atlanto-axial pathology, including Type II odontoid fractures, requiring surgical fixation are potential candidates for MIS C1-2 percutaneous fixation.
Arthrodesis
This technique is mostly relying on the arthrodesis of the anterior construct. In rare cases without significant ligamentous injury, some fractures heal successfully and be treated with just fixation. We have found it feasible to decorticate the lateral mass with the drill either under direct visualization or with navigation. In addition, we were able to place bone graft fibers through the incisions to perform arthrodesis.
Navigation Accuracy
Navigation accuracy is critical to successfully performing this technique. We did not experience any clinical significant accuracy issues as we moved further away from the reference frame as can sometimes occur in the thoracolumbar spine. Due to the closer proximity of cervical vertebrae, this did not result in a clinically noticeable difference while navigating in the cervical spine.
We have utilized a navigated electrocautery knife that allows for release of the cervical fascia layers. Since this corridor is being made along the axis of the screw placement, there is minimal soft tissue pressure on the instruments. This technique preserves the accuracy in the percutaneous technique compared to attempting to obtain this lateral angle with navigation in an open midline exposure where significant deflection by the soft tissue does occur and limits accuracy.
Conclusion
MIS navigated percutaneous posterior pedicle screw fixation can be performed safely. These constructs are biomechanically superior with neurovascular complication rates comparable to traditional lateral mass screw technique. Further clinical studies are needed to validate the potential advantages of this MIS technique compared to traditional open techniques. While the current indications for this technique are relatively limited, the evolution of MIS cervical decompression techniques as well as navigation and robotics will provide an expanded role for percutaneous cervical pedicle screw instrumentation. 23
Footnotes
Authors’ Note
The authors have no personal or institutional financial interest in the drugs, materials, or devices described in this article, except as follows: Domagoj Coric, MD: Spine Wave—consultant, royalties, direct stock ownership; and Medtronic—consultant, royalties. This study was approved by Atrium Health Institutional Review Board; Approval Number: 03-21-22E.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.