
Abstract
Study Design
Retrospective comparative study.
Objective
This multicenter European study aimed to compare the accuracy, complication rates, and incidence of revision surgery associated with three distinct cervical pedicle screw (CPS) insertion techniques: freehand, navigation-assisted (Loop-X/O-arm), and patient-specific 3D-template guided approaches. The primary endpoint was to provide evidence to support decision-making in cervical spine instrumentation.
Methods
A retrospective, observational study analyzed prospectively collected data from 97 adult patients who underwent posterior cervical fusion with CPS between January 2019 and August 2024. Screw accuracy was assessed using intraoperative or postoperative CT scans, according to the Gertzbein–Robbins classification. Intraoperative and postoperative complications were systematically evaluated.
Results
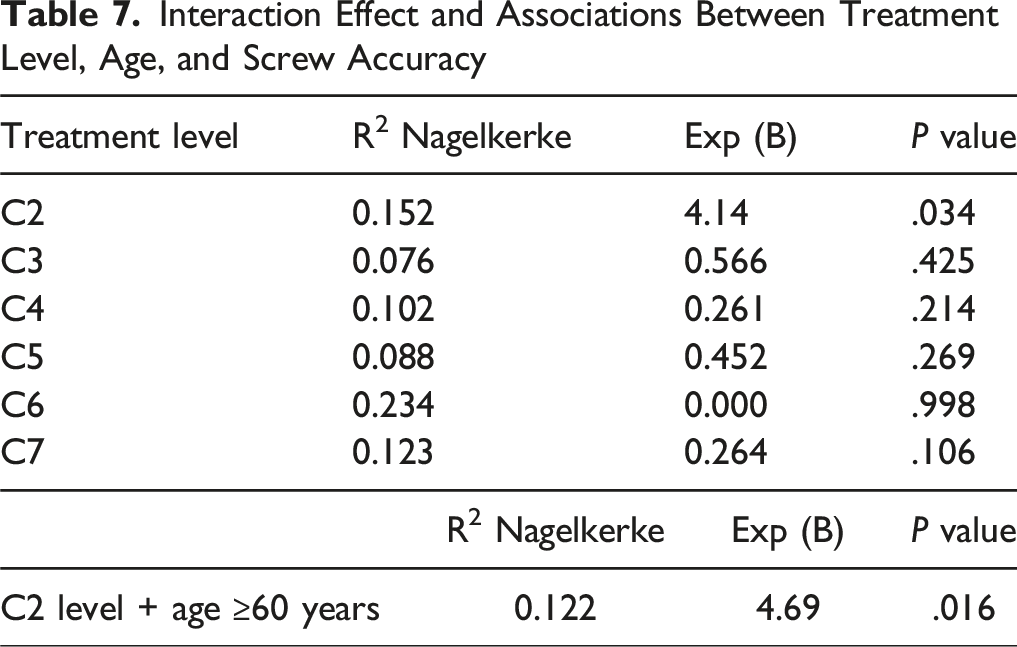
A total of 369 CPS were implanted, with an overall accuracy (Grade A/B) of 90.7%. Patient-specific 3D-templates yielded the highest accuracy (97.7% of grade A/B screws), significantly superior to navigation-assisted (85.5%) and freehand (80.0%) techniques (P < .001). The lowest accuracy was observed at the C2 level (79.4%; P < .001). Patients over 60 years of age undergoing surgery at the C2 level had a 4.7-fold increased likelihood of suboptimal (Grade > B) screw placement (P = .016). The overall rate of intraoperative and postoperative complications was significantly higher in the freehand and navigation-assisted groups (P < .05).
Conclusion
CPSs are safe and effective for cervical fusion, with acceptable complication rates. Patient-specific 3D templates offer superior accuracy and fewer complications, but its applicability is limited in urgent cases. Navigation provides good accuracy, but is associated with higher costs and potential technical inconveniences. Technique selection should consider surgeon expertise, resources, and patient-specific factors.
Introduction
Cervical spine complex anatomical and biomechanical characteristics pose significant challenges for safe and effective pedicle screw placement. Morphological variability and small size of cervical bodies and pedicles make it difficult to identify reliable anatomical landmarks, and damage to the surrounding neurovascular anatomical structures may lead to severe complications. 1 Despite these risks, cervical pedicle screws (CPS) offer superior biomechanical stability compared to other posterior fixation techniques making them the preferable choice in managing cervical spine disorders. 2 However, the technical complexity of CPS insertion underscores the need for advanced techniques to enhance accuracy and safety.
Several techniques have been developed to improve CPS placement accuracy. The traditional freehand technique heavily relies on the surgeon’s experience and fluoroscopic guidance, but is associated with higher rates of screw misplacement, especially in challenging anatomical scenarios. 3 Computer-assisted navigation systems, such as those utilizing intraoperative 3D fluoroscopy (eg, O-arm or Loop-X technologies) or region-matching computed-tomography (CT) navigation systems, assure real-time guidance based on imaging. However, accuracy may be compromised by reference array displacement or anatomical shifts during surgery. Patient-specific 3D-printed templates represent an innovative technique, offering an anatomically tailored tool for screw guidance based on preoperative CT imaging. These templates have demonstrated high accuracy and minimal intraoperative variability, though their use is limited in emergency cases due to production times. 4
Although many studies have examined the accuracy and safety of CPS insertion techniques, existing literature presents a wide range of reported outcomes, and comparative data remain inconsistent. 5 Nevertheless, clinical outcomes, revision rates, and complication profiles also play critical roles in evaluating these technologies. The objective of this multicenter European study is to compare the accuracy, complication rates, and revision surgery incidence associated with three different CPS insertion techniques — freehand, navigation-assisted, and three-dimensional (3D)-template guided — in a clinical setting. The aim is to enrich existing data to support evidence-based decision-making and improve patient safety in cervical spine instrumentation.
Materials and Methods
This study was conducted following the Guidelines for Good Clinical Practice and the Declaration of Helsinki (2002) of the World Medical Association. Written informed consent was obtained from all the patients for each diagnostic and surgical procedure.
This multicenter, retrospective, observational study analyzed prospectively collected data from adult patients who underwent posterior cervical fusion with pedicle screws between January 2019 and August 2024. The surgical techniques included in the study were: freehand, navigation-assisted, and customized 3D template-assisted approaches.
Patients were selected using the following criteria: (1) age equal to or greater than 16 years; (2) indication for C2–C7 cervical fusion for pathologies causing cervical spine instability, including degenerative, oncologic, infectious, inflammatory, or cervical deformity conditions; (3) patients receiving intra or postoperative 3D CT examination; and (4) follow-up period of at least 6 months. The exclusion criteria were as follows: (1) previous surgery on the cervical spine; (2) incomplete medical data in the review case; (3) and other cervical fusion techniques than CPS.
All surgical procedures were performed by experienced spine neurosurgeons from the Molinette-CTO University Hospital of Turin (Italy), Städtisches Klinikum Karlsruhe (Germany), and Hôpital Européen Georges-Pompidou – Paris (France).
Surgical Techniques – Freehand
The target vertebra was identified using both anterior and lateral fluoroscopic guidance. A midline posterior longitudinal incision was then made at the surgical site, followed by subperiosteal dissection of the paraspinal musculature to expose the anatomical landmarks necessary for pedicle screw placement. Screw dimensions (type and length) were selected based on the vertebral body size and pedicle diameter. The optimal entry point and trajectory were determined under fluoroscopic visualization in both planes. A pilot hole was subsequently created, and upon confirmation of cancellous bone contact with a ball-tip probe, the appropriate tap was introduced. Pedicle screws of the predetermined specifications were then inserted and secured with connecting rods. Decompression or additional surgical procedures were performed as indicated.
Surgical Techniques – Navigation
The Loop-X® Mobile Imaging Robot (© 2025 Brainlab AG, Munich, Germany) is a self-moving, intraoperative cone-beam (CB) CT imaging system that aims to enhance the precision of the spinal navigation. It features a gantry opening of 121 cm, allowing flexible patient positioning in prone, supine, or lateral orientations. Its imaging capability is non-isocentric, enabling off-centered image acquisition. It is further equipped with a dynamic collimation technology focuses on the region of interest, thereby reducing exposure to surrounding tissues and minimizing the patient’s overall radiation dose. Loop-X offers a standard 3D scan volume of 25 cm in length and diameter, usually exceeding that of conventional C-arms. The 3D field of view (FOV) can be scaled from a minimum of 3 × 3 cm to a maximum of 48 x 25 cm. Extended 2D FOV provides X-ray images up to 25 × 60 cm, with automated image stitching in both 2D and 3D for wider and longer views. The screws are inserted following a previously designed trajectory, which will be confirmed with the final Loop-X-scan, allowing to waive a postoperative CT-scan.
On the other hand, the O-arm navigation system is a CT-based navigation system that scans the spine during surgery. This system creates images of the spine in both 2D and 3D, allowing visualization from every angle in real time. The reference array is typically affixed to a spinous process cranial to the intended instrumentation level. An initial O-Arm spin is performed using a high-dose radiation protocol to ensure acquisition of high-resolution intraoperative images. These images are subsequently transferred to the station navigation system, and the accuracy of image registration is confirmed using bony anatomical landmarks, most commonly the midline of the spinous processes. Pedicle screws are placed under guided navigation, which facilitates precise determination of entry points, screw dimensions, and trajectories. A navigated pedicle probe is utilized to create a channel through the pedicle into the vertebral body. The tract is palpated using a ball-tipped probe to assess cortical integrity, followed by tapping with a navigated instrument. After a second palpation to reconfirm the integrity of the tract, the pedicle screw is inserted using a navigated screwdriver. Throughout screw insertion, intraoperative neuromonitoring is continuously observed for any changes suggestive of neural compromise.
Surgical Techniques – Patient-specific 3D-Templates
Eligibility for CPS surgery using customized 3D templates was carefully evaluated on a high-resolution volumetric preoperative cervical CT scan to exclude any unfavorable anatomy for pedicle trajectories. A pedicle transverse angle >45°, a pedicle outer width <3.5 mm, and the absence of adequate intrapedicular cancellous bone were considered exclusion criteria for this surgical technique.
Surgical planning was based on the preoperative high-resolution CT scan using dedicated software (MySpine Surgical Planning Report, Medacta, Rancate, Switzerland) to identify the optimal screw entry point, trajectory, and dimensions. Each template was customized and patient specific. Both monolateral and bilateral templates were available, according to the surgeon’s preference. Accurate removal of soft tissue from the bony landmarks, without damaging the bone, was mandatory to ensure optimal adherence of the templates to the dorsal vertebral surface. Sterile, customized 3D models of the vertebrae of interest were available during the surgical procedure to confirm the exact locations of the CPS entry points, allowing real-time verification of template interlocking and orientation.
Outcome Measures
Baseline characteristics such as gender, age, pre-operative diagnoses were collected from the included cases. All patients underwent a high-resolution cervical spine CT scan with 3D multiplanar reconstruction, performed intraoperatively or within the first postoperative day, to assess the accuracy of screw trajectories in the axial, sagittal, and coronal planes. Screw accuracy was evaluated using the Gertzbein–Robbins 6 classification, based on the extent of pedicle cortical breaches, when present. Grade A/B screws were defined as completely intrapedicular or exhibiting a cortical breach <2 mm, respectively. Grades C, D, and E corresponded to cortical breaches of 2-4 mm, 4-6 mm, and >6 mm, respectively. Accuracy was analyzed both by surgical technique, regardless of vertebral level, and by vertebral level, regardless of surgical technique.
Intraoperative complications were systematically evaluated and included vertebral artery (VA) injury, pedicle fracture during screw insertion, need for intraoperative screw revision due to mispositioning as identified during surgery, and dural tear. Postoperative complications were assessed both during hospitalization and during follow-up of at least 6 months. These included wound infection, radiculopathy—defined as either radicular pain or new-onset neurological deficit—pseudoarthrosis, and the need for revision surgery due to screw mispositioning.
Statistical Analysis
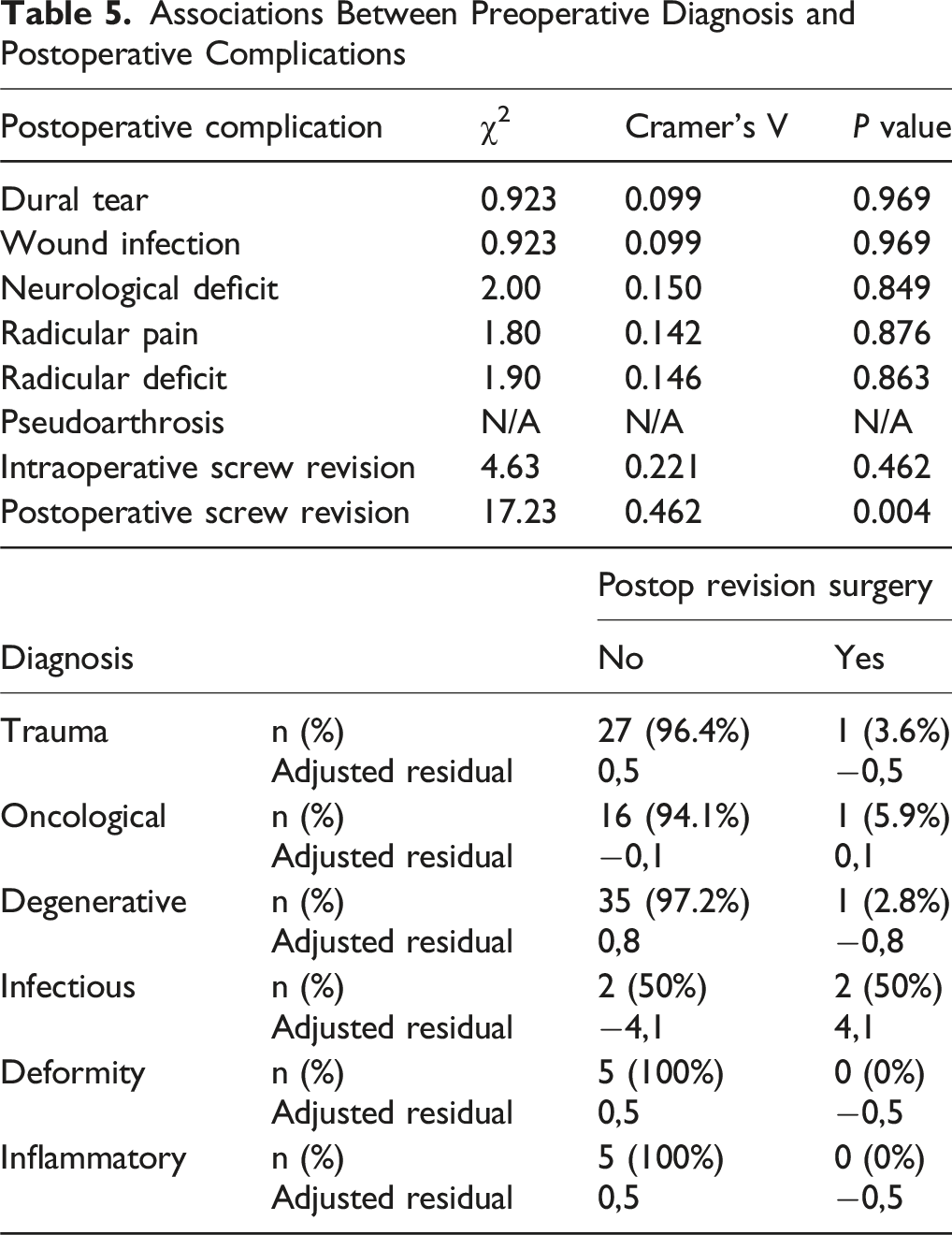
Descriptive statistics were presented as mean and standard deviation for continuous variables, and as frequency and percentage for categorical variables. The association between two categorical variables was assessed using the Chi-Square test, complemented by Cramér’s V index to interpret the strength of the association. To identify specific cells with stronger associations between the examined categories, standardized adjusted residuals were calculated. A residual value greater than ±2.5 indicates a significant deviation from the expected frequency: values >2.5 signify an excess of observed cases, whereas values <−2.5 indicate a deficit.
Differences in the distribution of a quantitative variable across groups with more than two categories were evaluated using the Kruskal-Wallis test. To identify optimal cut-off points for quantitative variables, the Receiver Operating Characteristic (ROC) curve analysis and Youden’s J statistic were applied. Statistical significance was defined as a P-value ≤.05. The effect of a single independent variable on a binary dependent variable was assessed using univariate binary logistic regression. To evaluate the impact of multiple independent variables on a binary dependent outcome, a multivariate logistic regression model was employed. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA) and Jamovi (Version 2.3).
Results
Study Population
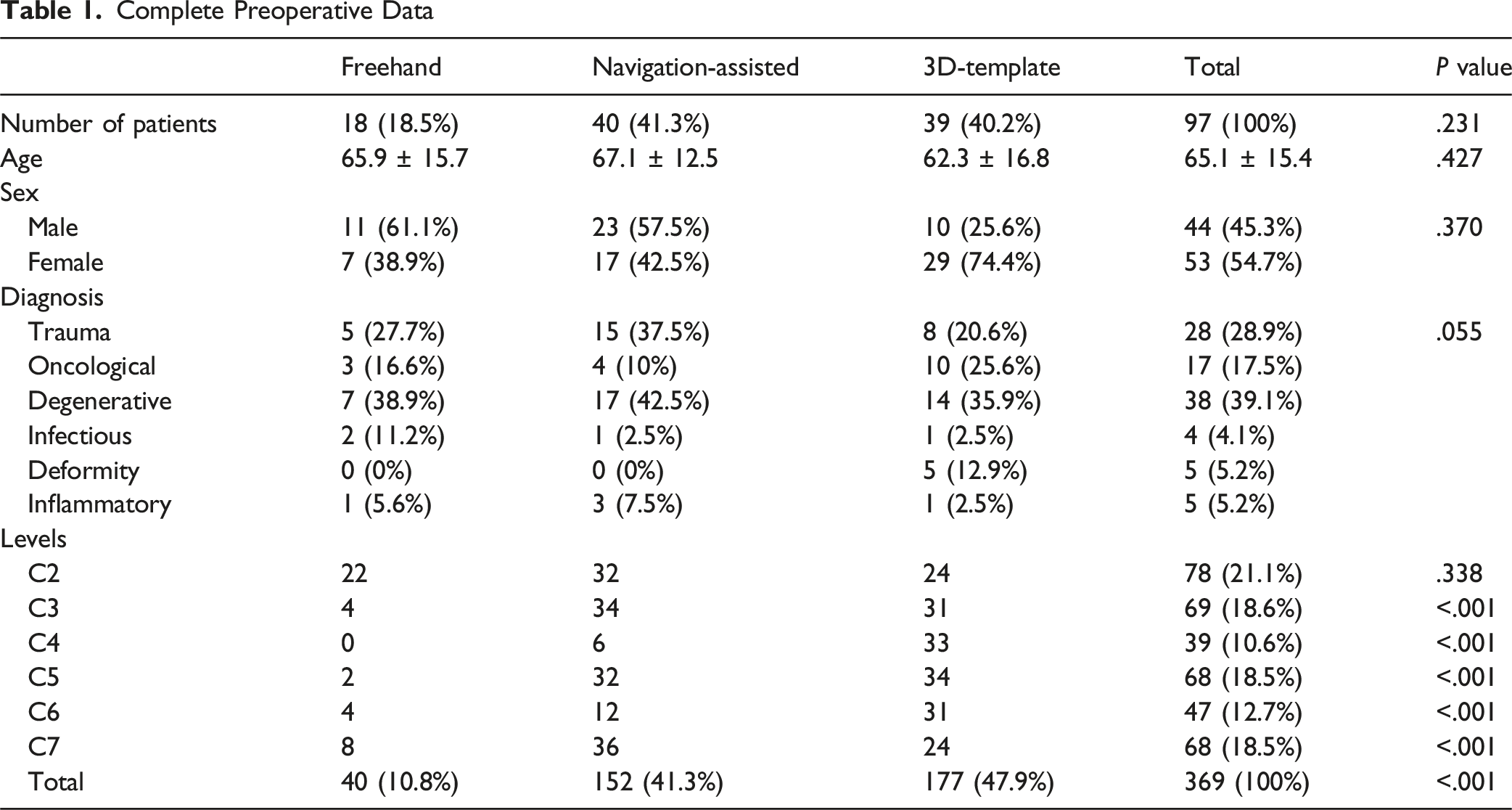
A total of 97 patients met the inclusion criteria and were evaluated. The mean age at the time of surgery was 65.1 ± 15.4 years, with no significant differences between groups. The most frequent preoperative diagnoses were degenerative (39.1%), traumatic (28.9%), and oncological (17.5%) conditions, accounting for 85% of the indications for CPS surgery. No significant differences were found in the distribution of preoperative diagnoses among the groups (P = .055).
Complete Preoperative Data
Postoperative Outcomes: CPS Accuracy
Cervical Pedicle Screw Accuracy According to Surgical Technique and Treatment Level
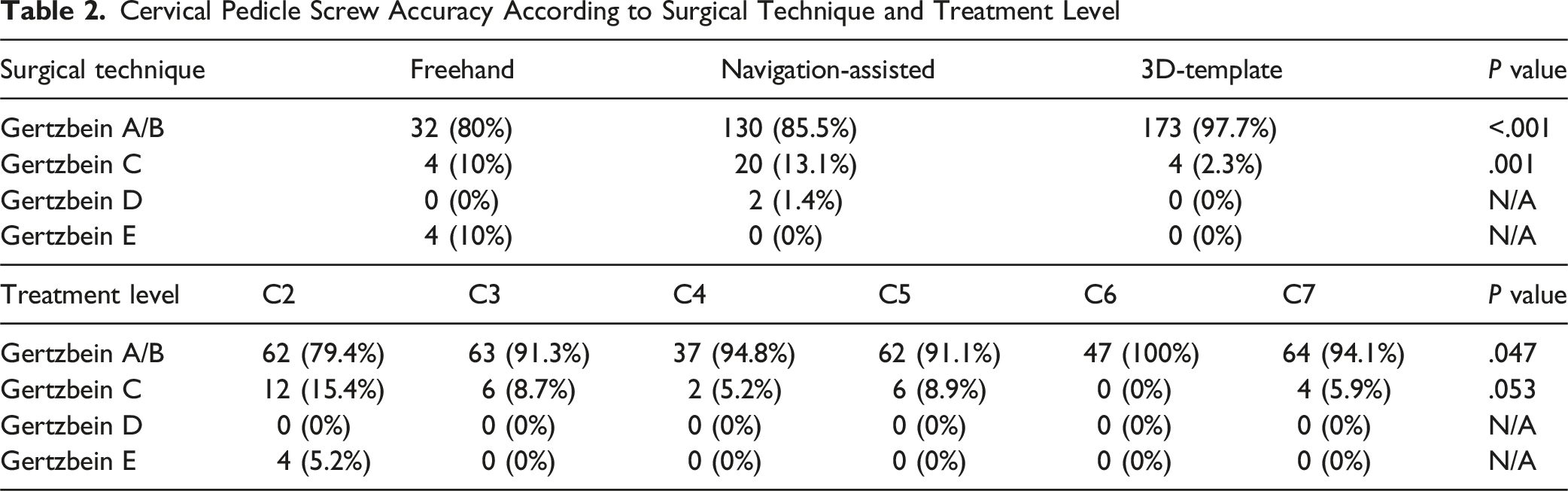
When considering surgical technique, the highest accuracy was achieved in the group treated using 3D-templates, with an overall rate of grade A and B screws of 97.7%. Moderate to severe cortical breaches were reported in 2 CPSs (1.4%) in the navigation-assisted group and in 4 CPSs (10%) in the freehand group. When considering treatment levels, the highest accuracy was achieved at the C6 level (100%), with grades A and B obtained in more than 90% of cases from C3 to C7. The lowest accuracy was observed at the C2 level, with an overall rate of grades A and B of 79.4%. No moderate cortical breaches were reported in any group, while severe breaches were documented in 4 CPSs (5.2%) in the freehand group.
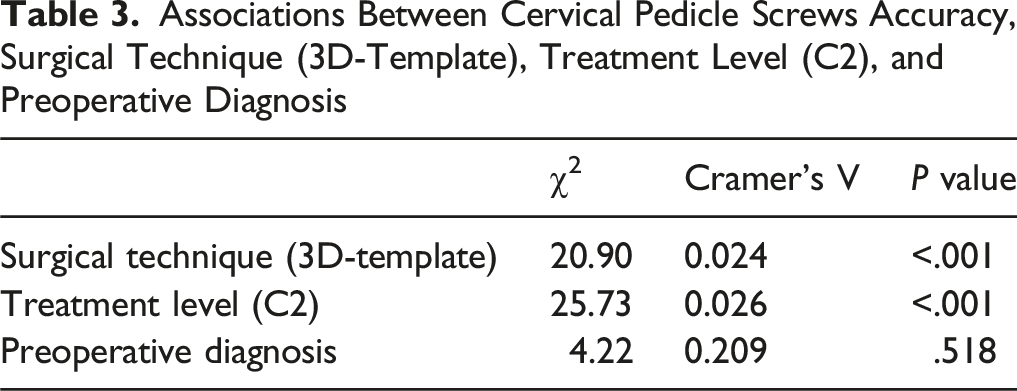
Associations Between Cervical Pedicle Screws Accuracy, Surgical Technique (3D-Template), Treatment Level (C2), and Preoperative Diagnosis
Postoperative Outcomes: Complications
Intraoperative and Postoperative Complications Associated With Each Surgical Technique
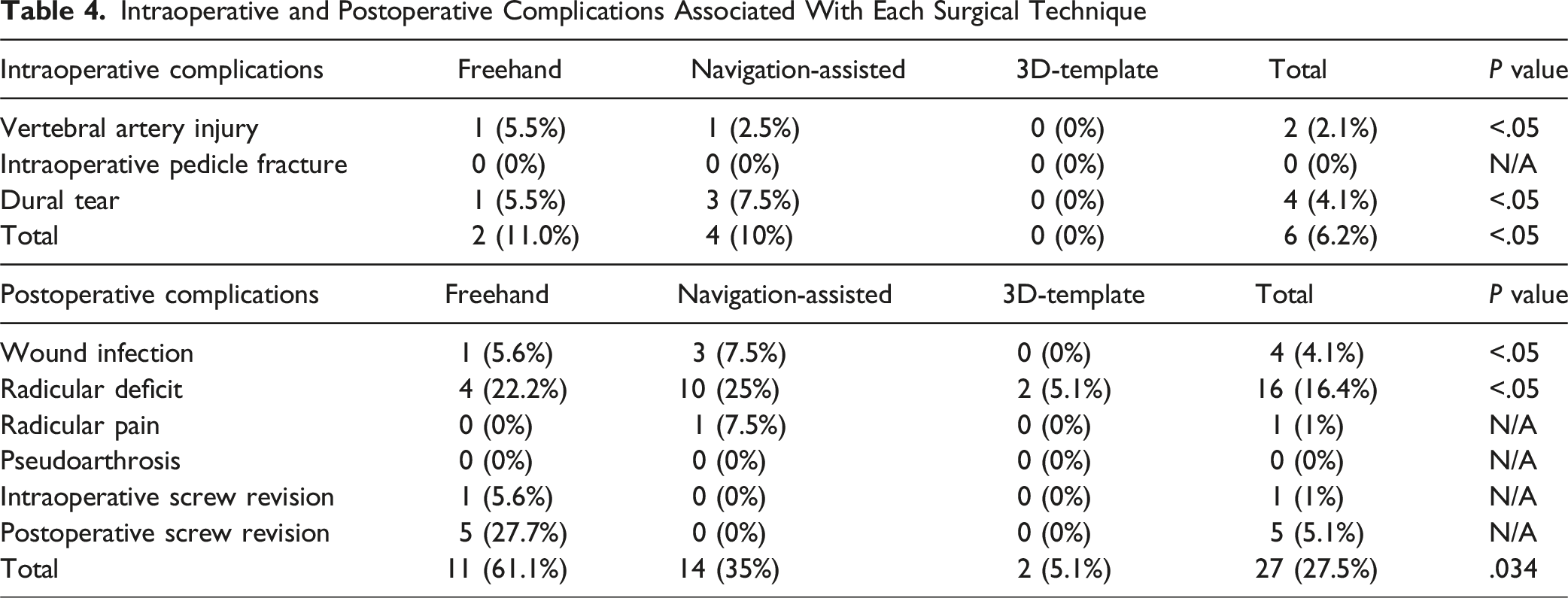
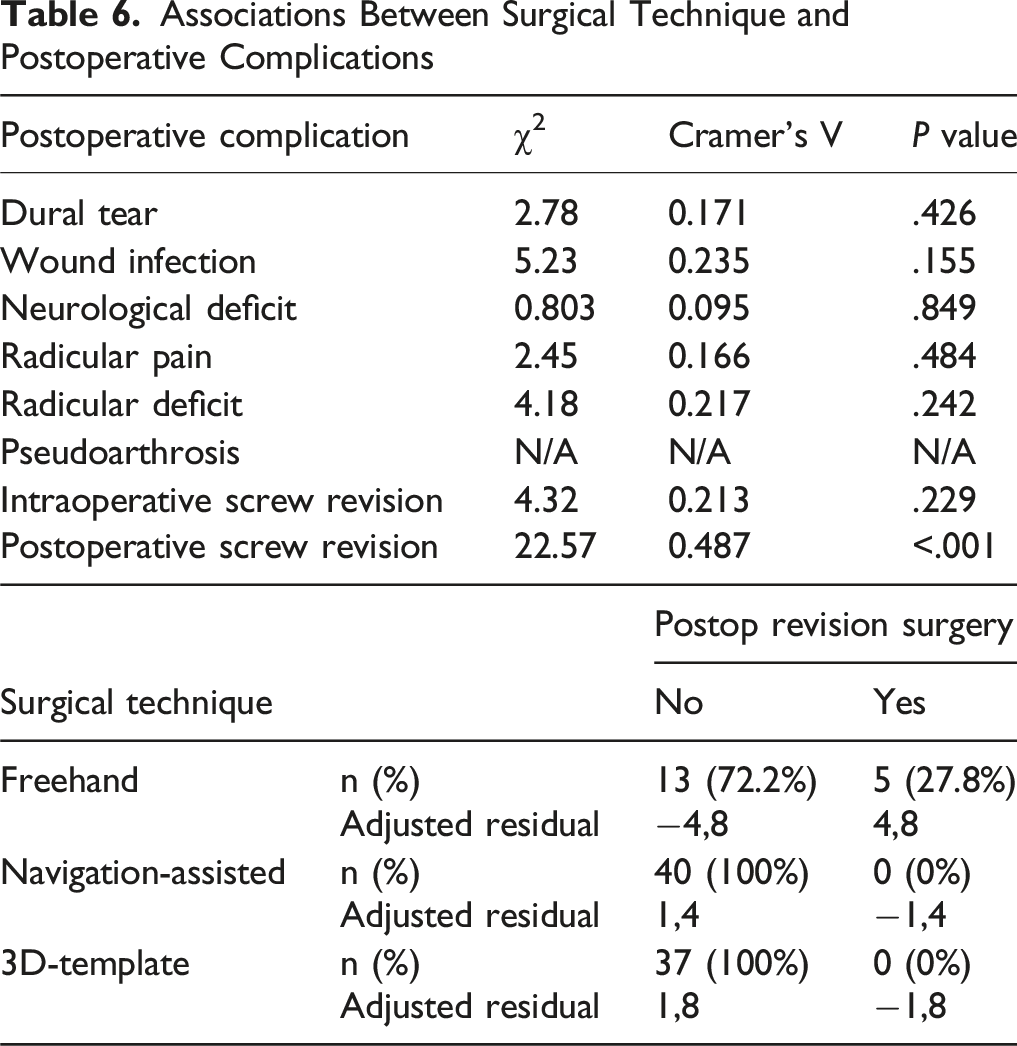
No cases of pseudoarthrosis were reported in any group. A total of 4 wound infections (4.1%) were reported: 1 (5.6%) in the freehand group and 3 (7.5%) in the navigation-assisted group. Only one case of persistent postoperative radicular pain was documented in the navigation-assisted group. No intraoperative or postoperative screw revision surgeries were reported in the 3D-template or navigation-assisted groups. Revision surgery was required only in the freehand group, with intra- and postoperative revision rates of 5.6% and 27.7%, respectively. The overall rate of postoperative complications was significantly higher in the freehand and navigation-assisted groups compared to the 3D-template group (P = .034).
Associations Between Preoperative Diagnosis and Postoperative Complications
Associations Between Surgical Technique and Postoperative Complications
Postoperative Outcomes: Impact of Preoperative Characteristics
Interaction Effect and Associations Between Treatment Level, Age, and Screw Accuracy
Discussion
The results of this study demonstrated an overall CPS placement accuracy of 90.7%, regardless of the surgical technique employed, with an acceptable incidence of postoperative neurovascular iatrogenic injuries, comparable to previously published data.4,5 While sex and preoperative diagnosis did not impact postoperative outcomes, a significant association was observed between age and CPS accuracy at the C2 level in patients over 60 years of age. Overall, the results of this multicenter study confirm the safety and effectiveness of CPS in cervical spine fusion surgery, underscoring the advantages of emerging technologies in optimizing screw placement accuracy and improving postoperative outcomes.
CPS Accuracy – Patient-specific 3D-Templates
Overall, CPS placed using patient-specific 3D templates proved to be significantly more accurate than those placed using other techniques, achieving a grade A/B screw rate of 97.7%. These results are consistent with previously published case series reporting CPS accuracy rates ranging from 93% to 100%, based on completely intrapedicular placement or cortical breaches of <2 mm when using 3D-template technology.7-15
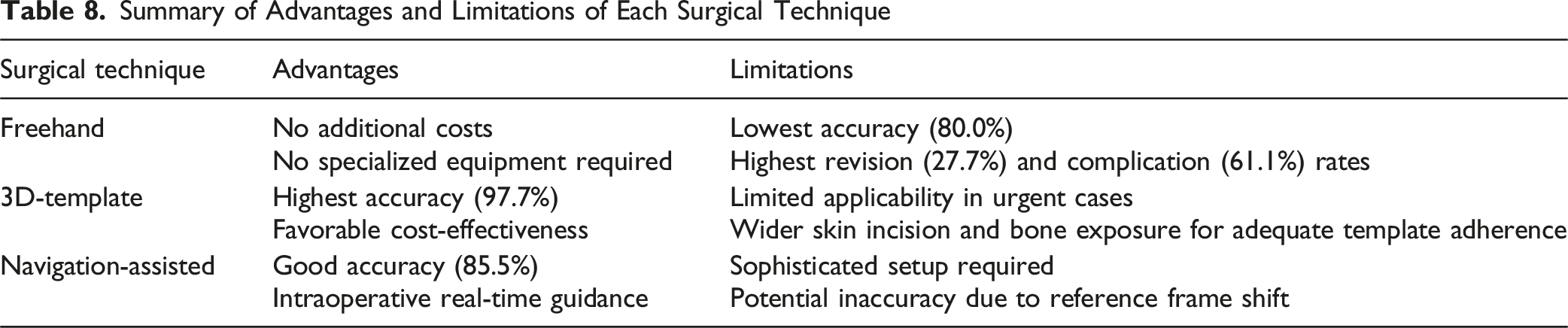
One of the key advantages of 3D templates lies in their ability to be securely fixed to the dorsal bony surface of the vertebrae. This provides a stable platform for surgical instrumentation and significantly reduces inaccuracies caused by vertebral body rotation during pedicle cannulation and screw placement. 7 Additionally, 3D templates are significantly less expensive than navigation-assisted technologies, optimizing cost-effectiveness and enhancing the applicability of this method across a broader range of healthcare settings. 16
Despite these advantages, 3D templates also present notable limitations. The manufacturing process of the patient-specific guides typically requires 7 to 10 working days, which restricts their use in urgent cases requiring immediate intervention. 7 Furthermore, adequate exposure of the bony surfaces to ensure optimal template fitting often necessitates more extensive dissection and retraction of the paravertebral muscles, potentially resulting in larger skin incisions. 17
CPS Accuracy – Navigation-Assisted Technologies
The rate of CPS classified as grade A/B in the group of patients operated on using navigation-assisted techniques was 85.5%, with 20 screws (13.1%) graded as C and 2 screws (1.4%) as D. The literature reports variable accuracy rates for CPS placement using CT-based navigation-assisted techniques, with pedicle breach rates ranging from 2.9% to 22.9%.18-22
Although numerous studies have demonstrated improved CPS accuracy with navigation-assisted techniques, several challenges remain unresolved. 23 While generally accurate, intraoperative navigation systems such as O-arm or Loop-X can lead to screw misplacement. 24 In fact, in our cohort, three cases of major pedicle violation (≥2 and <4 mm) were observed, accounting for 2.8% of total cases, which can cause catastrophic complications. Despite the fixation of reference frames during intraoperative imaging, even minimal displacement of the frames during surgical manipulation can result in significant deviations in screw trajectories. Furthermore, the downward pressure applied to the vertebra during pedicle cannulation may induce ipsilateral vertebral body rotation, substantially increasing the risk of lateral pedicle breach and VA injury.19,22,25
This concern is particularly relevant for mid-cervical segments (C3–C5), which exhibit greater mobility compared to the more caudal cervical vertebrae (C6–C7) and the upper cervical vertebra (C2).16,26,27 In a study by Shin and colleagues, 28 the accuracy rate for screws placed at mid-cervical levels ranged from 83.3% to 85%, significantly lower than the 93.3%–100% accuracy observed for screws placed in the upper and lower cervical spine. The findings of the present study are consistent with these results, as 45% of screws with suboptimal accuracy were located at the C3–C5 levels.
CPS Accuracy – Freehand Technique
The overall accuracy of CPS placement using the freehand technique was 80%, with rates of grade C and E screws each accounting for 10%. Previous comparable studies reported accuracy rates ranging between 85.2% and 93.3%.29-32 Although the literature on the accuracy of freehand CPS placement is highly heterogeneous and variable, the results obtained in this case series appear to be slightly inferior to those previously published.
The lower accuracy associated with the freehand CPS technique is a well-documented issue in the literature. Despite the development of various surgical techniques and advancements in intraoperative fluoroscopy to monitor screw positioning, freehand CPS placement remains a surgical challenge. 23 The significant variability in anatomical landmarks among individuals complicates the identification of optimal entry points. Furthermore, in certain pathological conditions—such as degenerative cervical spondylosis and inflammatory spondylitis—bony landmarks may become unrecognizable. 33 Supporting this hypothesis, the results of the present study revealed a diagnosis of degenerative spondylosis in 50% of patients with screws graded higher than B on the Gertzbein scale.
Postoperative Complications
A total of 2 cases (2.1%) of iatrogenic VA injury due to lateral pedicle breach were reported: one occurred in the freehand group, involving screws placed at the subaxial level (C5–C7), and one in the navigation-assisted group, involving screws placed at the C2 level. No VA injuries were observed in the group of patients treated with 3D-templates.
A recent systematic review by Ball et al 34 reported an incidence of VA injury ranging between 0.1% and 1.1%. These findings align with a previous review published by Wright et al, which reported a risk of VA injury of less than 0.5% per screw. 35 Although the present study showed a slightly higher incidence of iatrogenic VA injury compared to previously published data, none of the cases resulted in neurological sequelae or required surgical or interventional neuroradiological management.
Overall, this study demonstrated a relatively high rate of postoperative radicular deficit, reported in 5.1% to 25% of cases. It is important to note that none of these deficits were caused by direct injury from CPS but rather resulted from the decompressive surgical maneuvers required in each case or alternative causes. These findings are consistent with existing literature, which reports a <1% risk of radicular injury secondary to superomedial pedicle breach.36,37
Summary of Advantages and Limitations of Each Surgical Technique
Limitations
This study has several limitations that should be acknowledged. First, it presents the well-known limitations of a retrospective design, and the absence of randomization and a control group limits the ability to establish causality between the surgical techniques and outcomes. Second, as a multicenter study involving multiple surgeons with varying levels of experience and different surgical preferences, procedural heterogeneity may have influenced the results. While this reflects real-world practice and enhances external validity, it introduces variability that may affect the interpretation of the data. Lastly, while the number of C2 screws was comparable across all techniques, a significant imbalance was observed in the distribution of subaxial screws, with 3D-template and navigation-assisted techniques accounting for a substantially higher number of placements compared to freehand technique, thus limiting the generalizability of our findings regarding subaxial screw placement.
Conclusions
Overall, the accuracy of CPS was 90.7% regardless of the surgical technique used, with an acceptable incidence of neurovascular injuries comparable to existing literature. These findings confirm the safety and applicability of CPS in cervical fusion surgery.
The use of 3D templates resulted in significantly higher accuracy compared to other techniques, along with a favorable incidence of postoperative complications, confirming the advantages previously demonstrated in similar studies. Despite these advantages and the favorable cost-effectiveness, their limited applicability in urgent cases should be considered when selecting the surgical technique. The accuracy using navigation-assisted technologies was overall optimal and comparable to existing evidence from the literature, confirming its effectiveness and safety for CPS placement. Nevertheless, certain technical inconveniences and the higher costs remain significant issues for this type of technology.
Considering the favorable safety and efficacy profile of these techniques, the choice of the technology for CPS placement should depend on the surgeon’s expertise and on the availability of resources within the healthcare system. Ongoing technological advancements and future comparative research will be crucial to further enhance the accuracy of CPS in cervical fusion procedures.
Footnotes
Ethical Approval
The local ethical committee reviewed the study design and confirmed that no formal approval was necessary.
Informed Consent
This study was conducted following the Guidelines for Good Clinical Practice and the Declaration of Helsinki (2002) of the World Medical Association. Written informed consent was obtained from all the patients for each diagnostic and surgical procedure.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.