
Abstract
Introduction:
The cervical spine has the largest sagittal motion in the whole spine, and cervical alignment affects the thoracic sagittal alignment. However, the effects of cervical flexion and extension on thoracic sagittal alignment have not been investigated in detail. The purpose of this study was to analyze the change of thoracic sagittal alignment following cervical flexion and extension.
Subjects and methods:
A total of 55 consecutive patients (42 men and 13 women; average age 49.1 years) who presented to our department with spinal degenerative disease between January 2016 and September 2017 were enrolled in our study. Subjects with a history of trauma, infection, tumor, inflammatory disease, ossification, or cervical deformities, and those who had undergone spinal surgery were excluded. The following parameters were analyzed: occipito-axial angle (O–C2), C2 slope (C2S), C2–C7 angle, T1 slope (T1S), thoracic kyphosis, T1–T4 angle, T5–T8 angle, T9–T12 angle, lumbar lordosis, sacral slope, pelvic tilt in cervical flexion, neutral, and extension.
Results:
Cervical flexion significantly decreased O–C2, C2–C7 angles and T1S, and increased C2S. Cervical extension conversely changed these parameters. At cervical flexion, the correlation of C2–C7 angle with thoracic parameters was maintained, except for the T1–T4 angle. At cervical extension, the correlation was observed with T1S and T1–T4 angle.
Conclusion:
Cervical flexion affects the T1S and T5–T8 angle, but there is no significant change in T1–T4 and T9 and lower spino-pelvic columns. This study suggests that T2–T4 can be considered as a stable distal end when cervical long fixation for corrective surgery is performed.
Introduction
The change of cervical sagittal alignment affects and is affected by other parameters of the spine in preserving global sagittal alignment. 1 The range of motion (ROM) of the thoracic spine is restricted by the ribs, 2 but the cervical spine normally has the largest sagittal motion of the whole spine, and cervical alignment affects thoracic sagittal alignment. 1,3 Previously, only a few studies have reported segmental ROM with regard to the thoracic sagittal plane. 2,4 The effects of cervical flexion and extension on thoracic and lumbo-pelvic sagittal alignment have not been investigated in detail. In a clinical setting, we encountered angular movements of thoracic spine that could induce thoracic compressive myelopathy in ossification of posterior longitudinal ligament patients. 5 Study of thoracic sagittal alignment by cervical sagittal motion is important for the treatment of thoracic alignment disorders. The purpose of this study was to analyze the change of thoracic sagittal alignment following cervical flexion and extension.
Materials and methods
A total of 55 consecutive patients (42 men and 13 women; average age 49.1 years) who presented to our department with spinal degenerative disease between January 2016 and September 2017 were enrolled in our study. Subjects with a history of trauma, infection, tumor, inflammatory disease, ossification, or cervical deformities, and those who had undergone spinal surgery were excluded. This study was approved by the ethics review board of our institution. Standing anteroposterior radiographs were taken in fists-on-clavicles position with elbows fully flexed and fists resting on clavicles in extended hip and knee position as described previously. 3,5,6 Lateral radiographs of the entire vertebral column were taken in cervical flexion, neutral, and extension (Figure 1(a)), and the reconstructed images of the cervicothoracic junction were shown in Figure 1(b). Subjects having difficulty with the radiographic procedures due to maintaining the posture without support were excluded. The following global spinal radiographic parameters were measured in the standing position by computer association: occipito-axial angle (O–C2), angle between C2 lower endplate and horizontal plane (C2S), cervical lordosis assessed by C2–C7 Cobb angle, which was defined as the angle from the lower endplate of C2 to the lower endplate of C7 (C2–7A), angle between T1 upper endplate and horizontal plane (T1S), angle between T1 upper edge and T12 lower edge (TK), T1–T4 angle, T5–T8 angle, T9–T12 angle, angle from upper endplate of L1 to upper endplate of sacrum (LL), angle between sacral plate and horizontal plane (SS), angle between line connecting midpoint of sacral plate to axis of femoral head and gravity line (PT) in cervical flexion, neutral, and extension positions. Whole spine anteroposterior and lateral radiographs were obtained using digital slot-scanning radiography mode of the Sonialvision safire fluoroscopy system (Shimadzu Corporation, Kyoto, Japan), and the association between changes in parameters during cervical motion was analyzed. The intra- and interobserver agreement rates of the measurements by this system have been described previously. 6

(a) Global and (b) cervical sagittal spinal radiography at (a′) cervical flexion, (b′) neutral, and (c′) extension positions.
Values were expressed as mean ± standard deviation (SD). In determining the sample size of this study, we referred to the number table by Cohen (Cohen, Psychol. Bull., 1992) 7 and used G*Power Analysis software version 3.1.9.4 (Heinrich-Heine University, Duüsseldorf, Germany). We set the significance level (α err prob.) at 0.05, the effect size f at 0.25, and the power (1 − β err prob.) at 0.8, and this means that at least 159 samples were considered necessary. In this study, there were 55 patients with three neck positions, and thus the total number for statistical analysis was 165 (55 × 3). Therefore, we think that the number of patients in this study was sufficient. Statistical analyses were performed using the JMP software package version 10.0 (SAS Institute Inc., Cary, North Carolina, USA). Wilcoxon/Kruskal–Wallis tests were used to determine intergroup differences among cervical flexion, neutral, and extension to analyze the outcome measures of parameters in sagittal spinal alignment. Correlations between the variables of spino-pelvic parameters were analyzed by Spearman rank correlation coefficient. A p value <0.05 was considered to indicate a statistically significant difference between two groups.
Results
The cervical ROM in the standing position was 50.3 ± 23.1°. In cervical flexion, O–C2, C2–C7 angles and T1S were significantly decreased, while C2S was increased. In contrast, in cervical extension, O–C2 and C2–C7 angles were increased, while C2S was decreased (Figure 2). However, T1–T4, T5–T8, T9–T12 angles and TK were not changed significantly in cervical flexion and extension (Figure 3). LL, PT, and SS were also not affected by cervical flexion and extension (Figure 4). Regarding correlations among these parameters, in cervical flexion, C2–C7 angle correlated with T1S and T5–T8 angle, but the correlation between C2–C7 and T1–T4 angles had disappeared. In cervical extension, C2–C7 angle showed correlation with T1S and T1–T4 angle but not with T5–T8 and T9–T12 angles (Table 1).
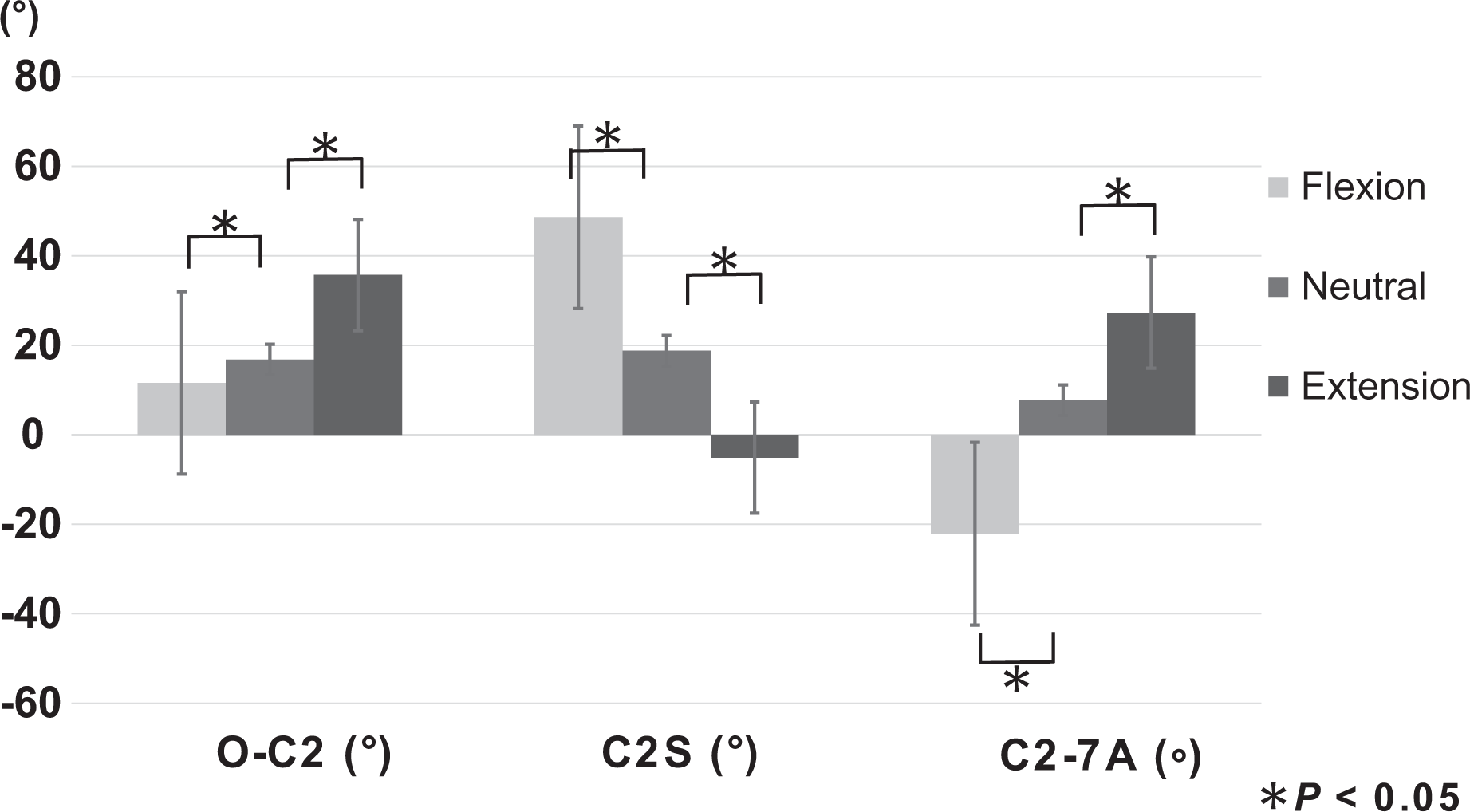
Cervical sagittal alignments at cervical flexion, neutral, and extension neck positions. Flexion and extension changed cervical alignments compared with neutral neck position. O–C2: O–C2 angle, C2S: C2 slope, and C2–C7A: C2–C7 angle.
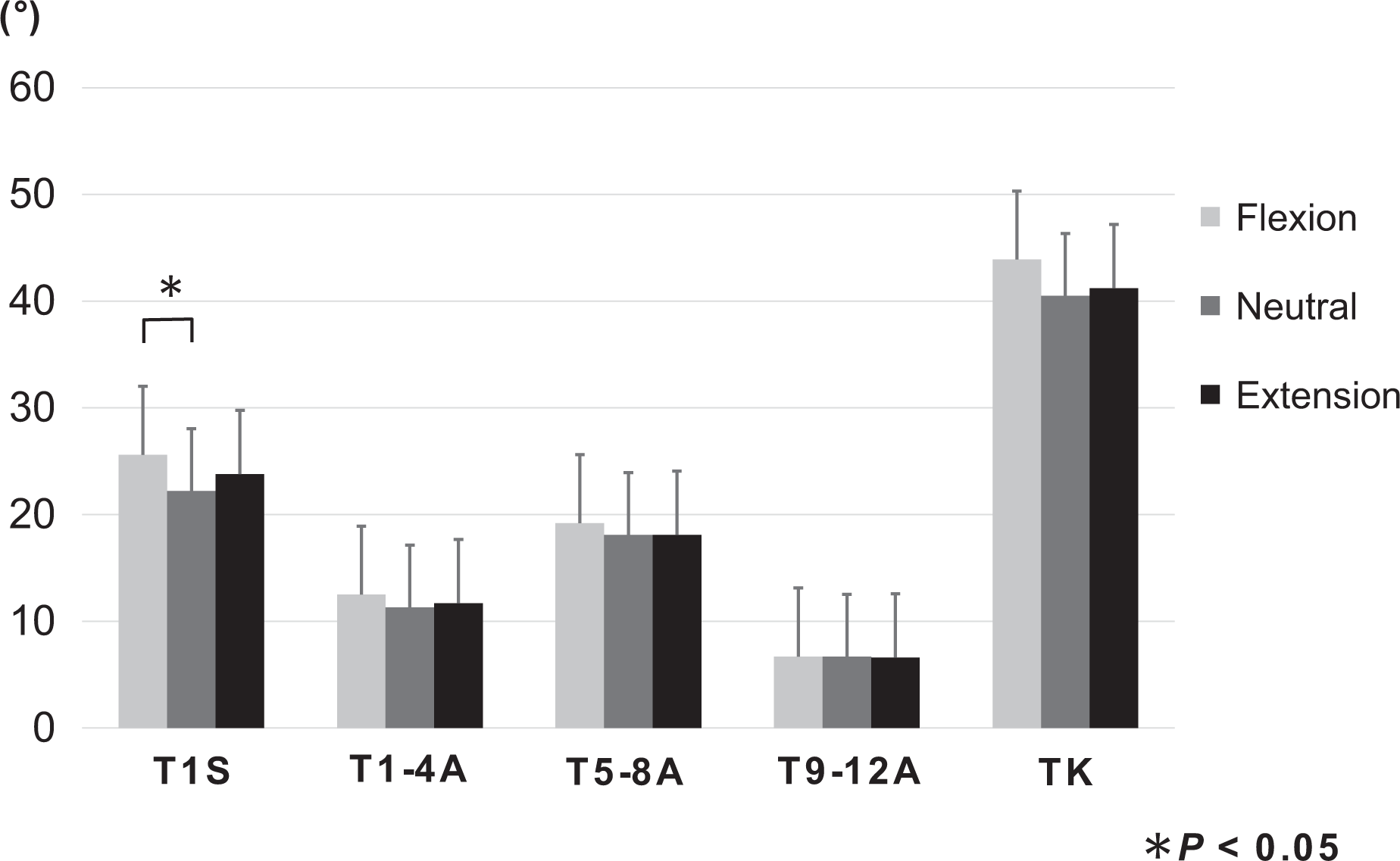
Thoracic alignments at cervical flexion, neutral, and extension positions. There were no significant changes in the three cervical positions below the T1–T4 angle. T1S: T1 slope, T1–T4A: T1–T4 angle, T5–T8A: T5–T8 angle, and T9–T12A: T9–T12 angle. TK: thoracic kyphosis angle.

Lumbar alignments at cervical flexion, neutral, and extension positions. Lumbar alignments did not change significantly in the three cervical positions. LL: lumbar lordosis; SS: sacral slope; PT: pelvic tilt; PI: pelvic incidence.
Correlation between C2–C7 angle and thoracic sagittal alignment at flexion, neutral, and extension cervical positions.a

a p Values are given in parenthesis.
b p < 0.05.
Discussion
It is known that the C2–C7 angle is well correlated with T1S and global thoracic curvature in the up-right neutral position. 3,4 The present study demonstrated that cervical sagittal motion affects the T1S and T5–T8 angle, but the T1–T4 angle, T9–T12 angle, and lumbo-pelvic columns did not change significantly. The reciprocal change of T1–T4 angle was smaller than that of T5–T8 angle upon cervical flexion and extension. The thoracic spine has limited ROM because of restriction by the ribs, 2,8 but our results showed no significant difference in thoracic sagittal alignment between cervical flexion and extension. However, correlation between the C2–C7 angle and T1S, T5–T8 angle was clear, and it should be taken into consideration in terms of the effects of cervical dynamic factors. The thoracic spine takes part in approximately 33% of cervical flexion and 21% of cervical rotation and is closely associated with cervical movement. 9 In our results, cervical sagittal alignment both in neutral and flexion/extension was affected by T1S. At cervical extension position, T1S was increased and T1–T4 angle had correlation to C2–C7 angle. These may represent a thoracic compensation to maintain balance by leaning forward slightly, as has also been reported in previous studies. 3,10 The thoracic spine has a regional interdependence and its dysfunction affects symptoms of the cervical spine. 11 The present study analyzed the association between global sagittal spinal alignment and cervical sagittal alignment in cervical flexion, neutral, and extension. For a detailed analysis, the thoracic spine was divided into three parts—T1–T4, T5–T8, and T9–T12. Alignments of T1–T4 angle, T9–T12 angle, TK, LL, and PT were not changed significantly by cervical flexion and extension in comparison with neutral position. However, T1S and T5–T8 angle positively correlated with C2–C7 angle at cervical neutral and flexion positions. These results indicate that T1–T4 movement was less than that of T5–T8 during cervical movement and was relatively rigid following cervical flexion. Morita et al., by computed tomography scanning, showed that total ROM of thoracic spine (T1/L1) was 31.7 ± 11.3° and that segmental ROM decreased from T1/T2 to T4/T5 but increased gradually from T4/T5 to T12/L1. 2 The stability of T1–T4 is supported by the presence of the shoulder girdle (scapula bone and rhomboid muscles) because rhomboid minor and major muscles are located from the scapula to C7–T5, 12 and the role of those back extensor muscles is particularly important. For cervical surgery strategy, those findings would represent very useful information, as selection of the lower end in case of posterior long fusion for cervical sagittal imbalance has been a controversial issue due to anatomical and biomechanical complexities of the cervicothoracic junction. The present study showed that T1S correlated with C2–C7 angle at cervical flexion, neutral position, and extension but that it was not correlated with T1–T4 angle at cervical flexion and neutral positions. Therefore, when cervical long fixation for corrective surgery is performed, the suitable distal end would be at T2, T3, or T4, but not at T1, because T1 can be mobile by cervical motion.
The present study has some limitations, the first being that measurement of the thoracic spine could not each vertebra because of difficulty with the X-ray findings. A second potential limitation was the fact that the clinical findings in the subjects were not analyzed. A third limitation was that the findings in this study only reflect the situation at standing straight but not at other postures such as sitting or stooping. Despite these limitations, our data from a quantitative analysis standpoint could provide useful basic information for considering the dynamic thoracic sagittal movement by cervical sagittal motion as well as present useful information to aid in the diagnosis and decision-making of surgical strategy for cervicothoracic spinal disease.
Conclusions
Cervical flexion affects the T1S and T5–T8 angle, while the T1–T4 angle and the T9 and lower spino-pelvic columns do not change significantly. This study suggests that T2–T4 could be considered as a stable distal end when cervical long fixation for corrective surgery is performed.
Footnotes
Acknowledgements
The authors are indebted to Mr Arndt Gerz for the editorial review of the English manuscript. Advice and comments given by him have been a great help to us. The authors are also grateful to Ms Yuri Amamizu of the Department of Orthopedic Surgery for assistance with preparation of the initial English manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.