
Abstract
Study Design
A prospective study of healthy volunteers
Objectives
The influence of the sagittal alignment of the spine and its influence on the extension reserve have been reported in the literature. However, specific analysis of the intrinsic coxofemoral and extrinsic pelvic component in subjects without any spinal or hip pathologies remains poorly reported. The aim of this study was to categorize the hip extension capacity, or extension reserve (ER), in relation to spinal sagittal alignment whilst standing, in a young healthy population. We hypothesized that the global extension reserve (GER) of the hip joint was influenced by the sagittal spinopelvic alignment.
Methods
We evaluated the ER of 120 healthy Caucasian volunteers (56 females (46.7%), 74 males (53.3%); mean age 25.6 years), using low dose radiographs from an EOS® X-ray imaging system in 2 functional positions; neutral standing position and in a forward lunge position. The GER is defined as the sum of the intrinsic (hip) extension reserve (IER) and the extrinsic (pelvic) extension reserve (EER). Cases were grouped into 4 sagittal alignment subtypes according to the Roussouly classification, and analyzed.
Results
Global extension reserve values were not significantly different between the 4 Roussouly subtypes (P = .094), nor between patients with a sacral slope (SS) <35° (types 1/2) and ≥ 35° (type 3/4) (P = .837). Statistically significant differences were seen between IER in each subtype (P = .015), and EER (P = .006). No difference in ER was seen between subtypes regarding pelvic incidence (PI).
Conclusion
An inverse relationship was found between IER and EER among Roussouly subtypes. The range of motion of the pelvis and the hip joint was higher in patients with a greater sacral slope.
Introduction
During hip arthroplasty or spinal deformity corrections, the association between the hip joint and spinopelvic alignment is underappreciated, as it can have strong effects on the flexibility and range of motion of the hip joint.1,2 To avoid complications such as hip instability or impingement, intra-operative adaptations may be required to adapt to the spinopelvic alignment3‐5 which, in itself, is dynamic and difficult to predict using today’s imaging systems. We know that the alignment depends on the lumbopelvic system6‐9 and is affected by the aging process10‐12 and other pathologies.13,14
Research into this area is increasing, but few studies have reported the association of the lumbopelvic-femoral complex and its impact on hip extension from a standing position, extension reserve (ER), in a healthy young population with no hip or spine pathologies.
Low dose radiographs achievable with the EOS® x-ray imaging system can be used to quantify ER with little risk to the patient. Global extension reserve (GER) is defined by the sum of the intrinsic (hip) extension reserve (IER) and the extrinsic (pelvic) extension reserve (EER). IER can be measured when standing while the hip is in maximum extension. EER is measured according to the difference in pelvic tilt between hip extension and the neutral position (Figure 1). Any pelvic tilt beyond this (EER) can be measured.
15
Standing, neutral reference position, and dynamic position in extension: measurement of the - EIR (difference between the Sacro Femoral Angle (SFA) in neutral (SFAN) and extension position (SFAE). - EER (difference between the sacral slope in extension (SSE) and the sacral slope in neutral position (SSN).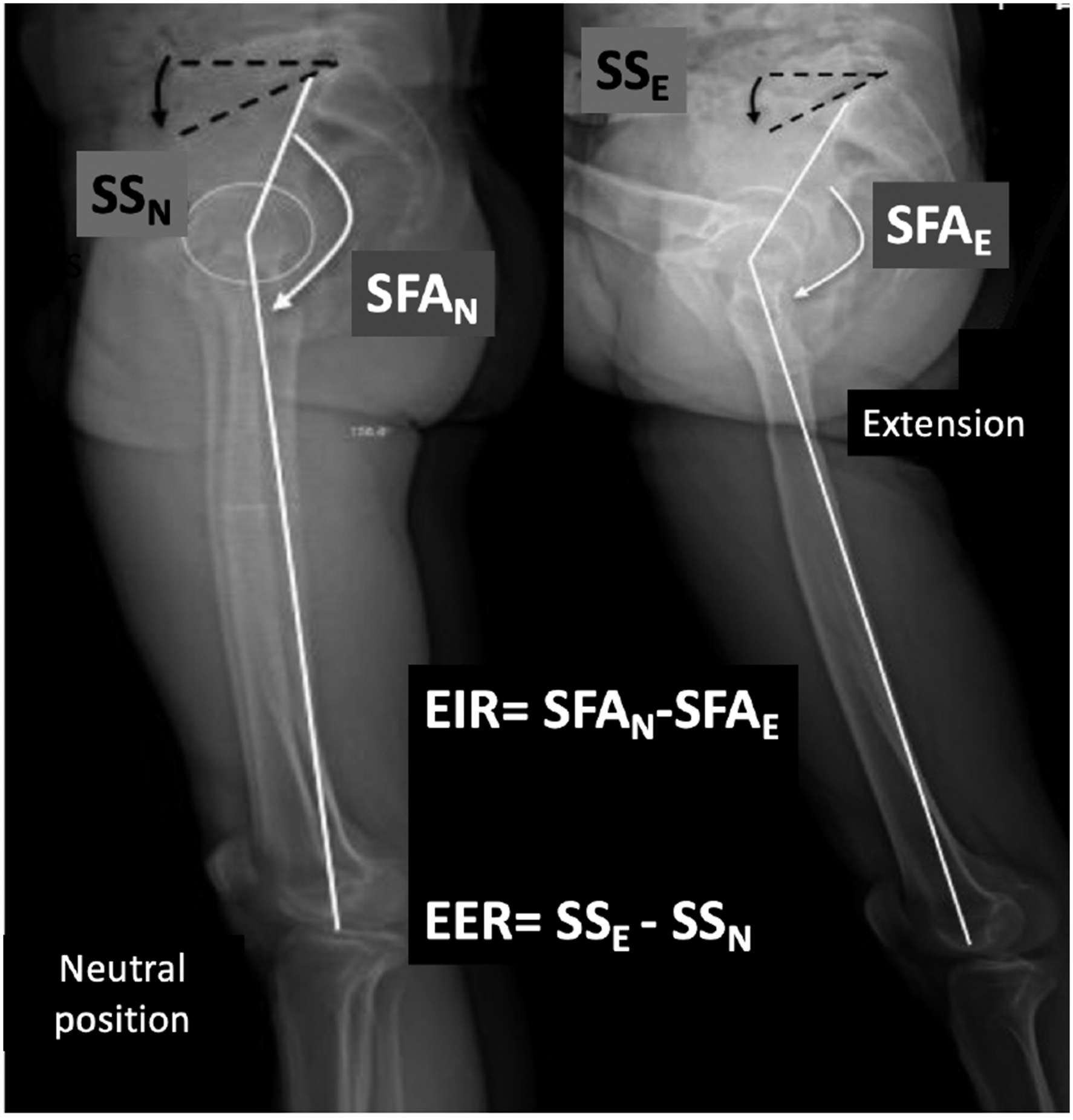
This study aims to categorize the hip's extension capacity in relation to spinal sagittal alignment in a young healthy population and to differentiate movement specific to the hip joint (IER) and the lumbopelvic complex (EER). We hypothesized that the GER of the hip joint defined by IER and EER would be influenced by the 4 sagittal alignment subtypes as proposed by Roussouly.16‐18
This study used the EOS® system to characterize lumbopelvic parameters as well as the extension reserve of the lumbo-pelvi-femoral complex.
Methods
Population
This prospective study recruited healthy volunteers from our hospital cohort from February to March 2015. Participants were excluded if they had any known spinal or lower limb diseases, or spine or hip abnormalities seen on the EOS X-rays. We included 120 participants (240 hips); no participants were excluded. After approval by the institutional review board of the University of Montpellier (Identifier: NCT01909258, CPP 2013.05.06, IDRCB: 2018-A00989-46), written informed consents were obtained from all patients prior to this study.
EOS® Acquisition Technique
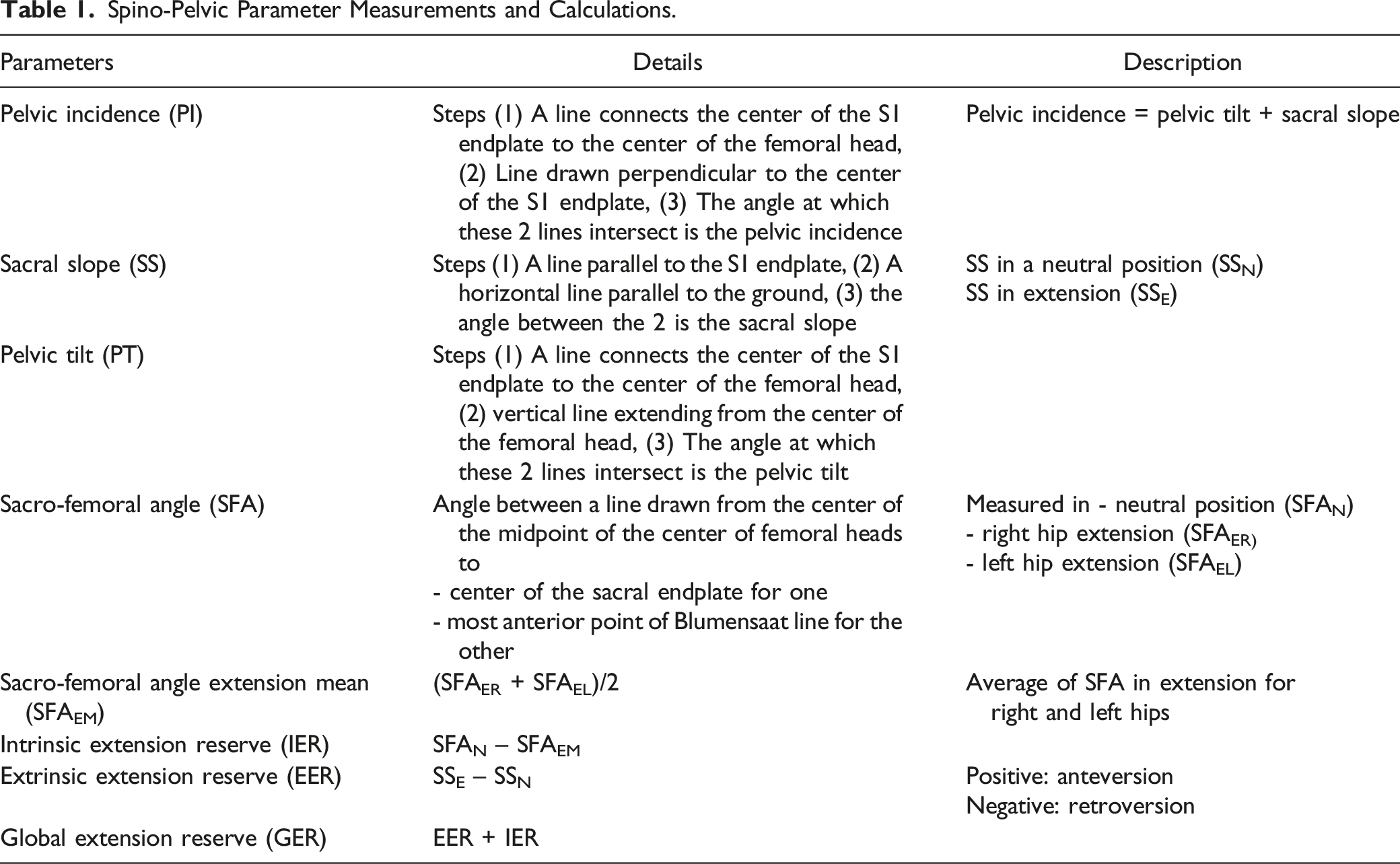
A neutral reference point was initially established for each participant, taken whilst they were standing naturally, looking straight ahead, with their feet 10cm apart and their hands held up to the side of their faces (Figure 2). A dynamic image was taken for each hip in extension whilst the contralateral foot was placed on a 40cm high step. During the dynamic phase, the trunk was held upright with hands remaining on the face. EOS® measurements were made by an independent observer. Spino-pelvic parameters measured are shown in Table 1.
15
Standing, neutral reference position (A) and dynamic position (B) in extension using a 40cm contralateral step for the left and right hip. Spino-Pelvic Parameter Measurements and Calculations.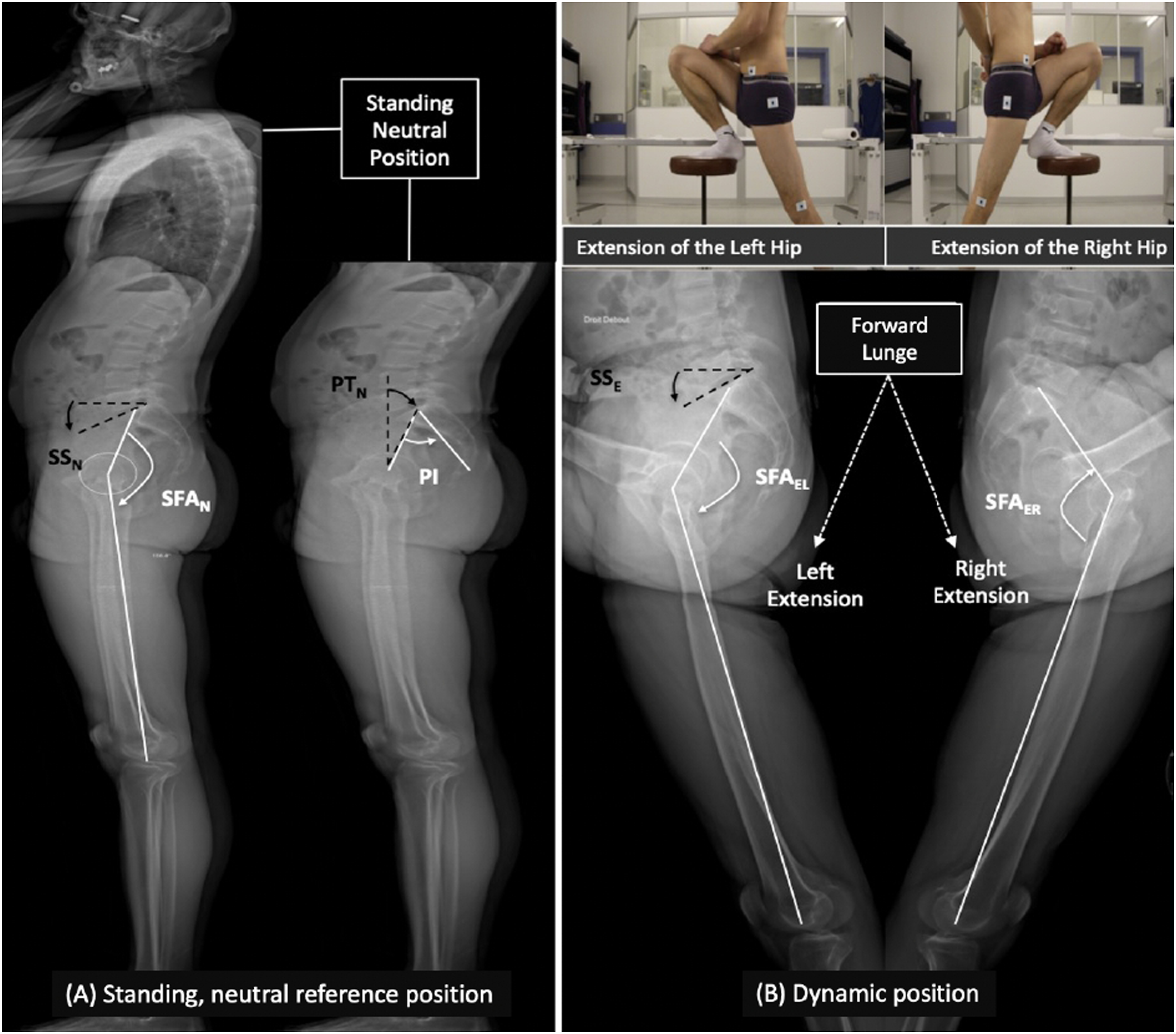
Participants were divided into 4 groups according to their Roussouly subtype for thoracolumbar sagittal alignment. Group 1 has a sacral slope (SS) of less than 35° with a short lumbar lordosis curve, Group 2 has a slope of less than 35° but with flat back lordosis, Group 3 has a slope of 35° to 45°, and Group 4 has a slope of over 45° (Figure 3).
17
Spinal curvatures (adapted from Roussouly et al.)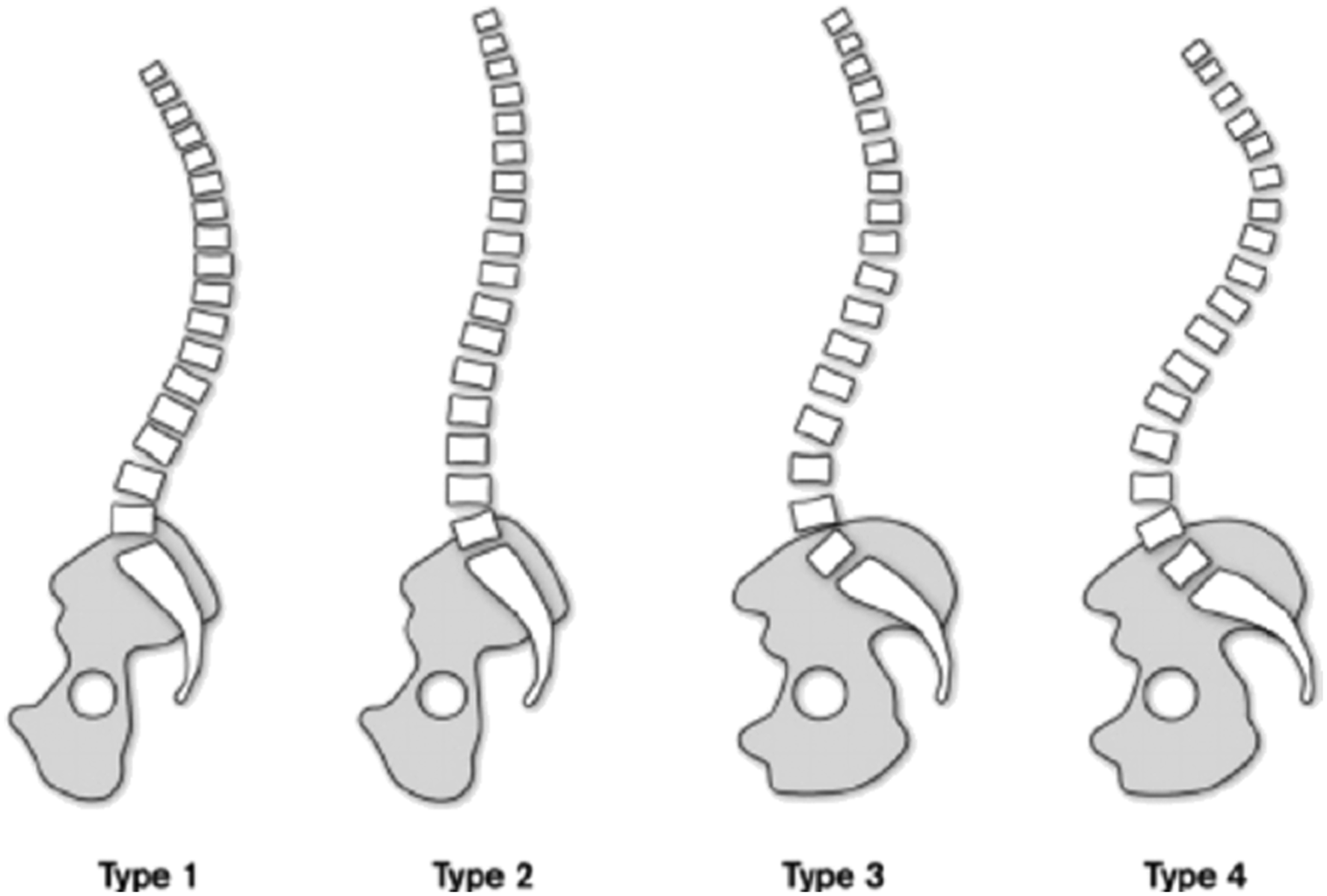
Statistical Analysis
Statistical analysis was performed using R version 3.5.1 software (R Foundation for Statistical Computing, Vienna, Austria). Quantitative variables were presented with means and standard deviations or medians and quartiles according to their distribution profile. Paired variables between IER in left hip extension and right hip extension (IERR) were compared using a non-parametric paired Wilcoxon test, and their concordance was evaluated by the Lin concordance correlation coefficient. The mean value of IER (IERm) was considered as the reference value for the analysis. Spearman's rank correlation coefficient was used to assess the correlation between the various parameters and the Kruskal-Wallis test was used to assess the association with Roussouly's subtypes. A P-value <.05 was considered statistically significant.
Results
Demographics of Participants, Divided into Roussouly Subtypes.
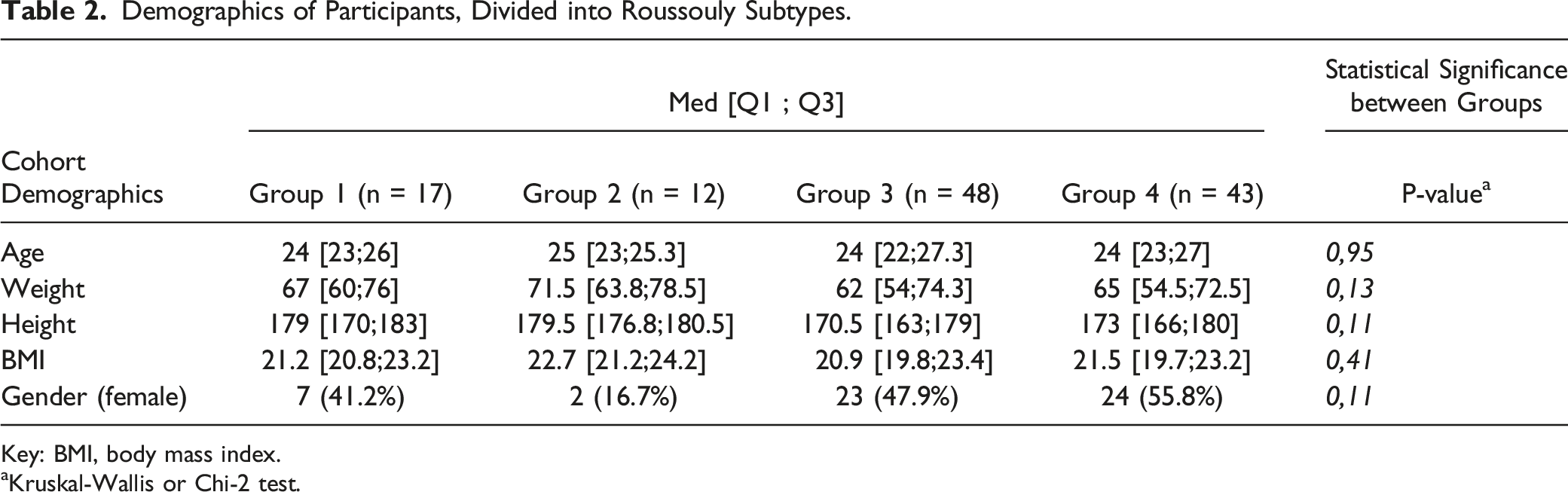
Key: BMI, body mass index.
aKruskal-Wallis or Chi-2 test.
Measurements of Spinopelvic and Extension Reserve Parameters.
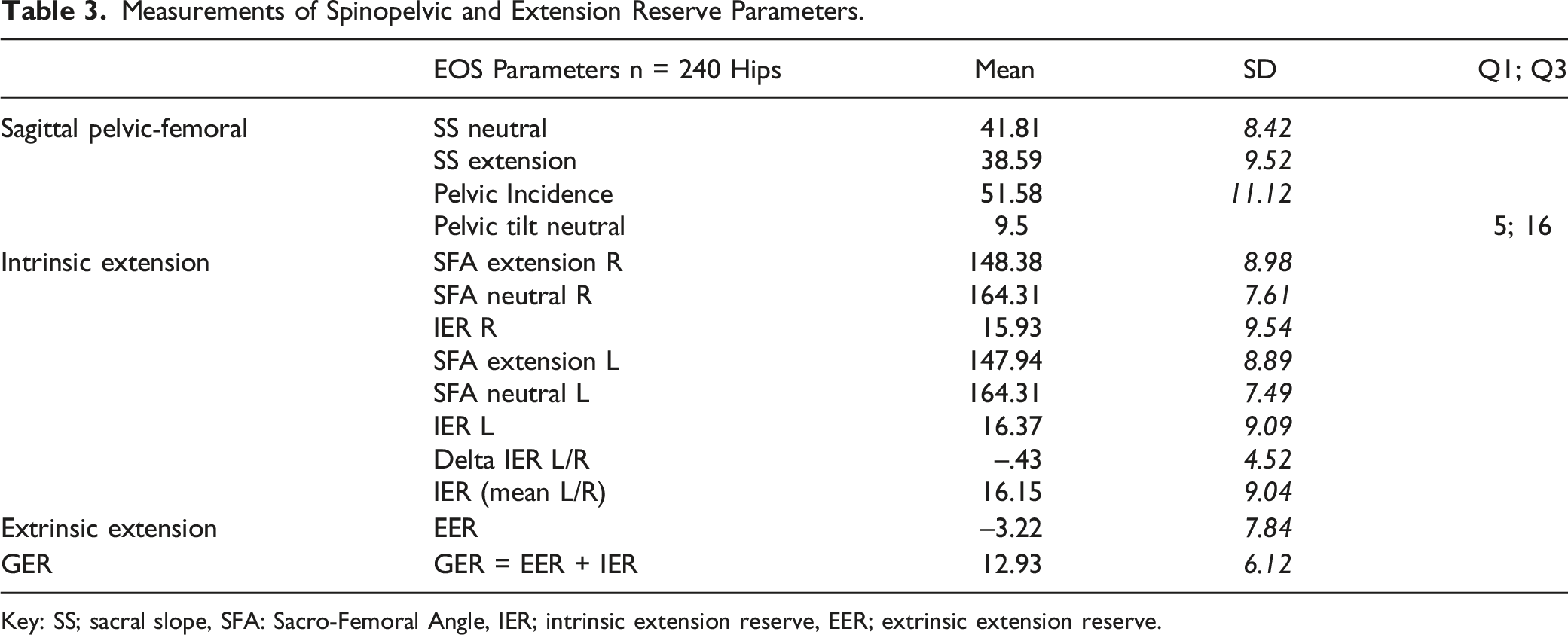
Key: SS; sacral slope, SFA: Sacro-Femoral Angle, IER; intrinsic extension reserve, EER; extrinsic extension reserve.
Correlation between Different Radiological Parameters in Different Hip Positions. Values in Bold are Statistically Significant (P < .05).
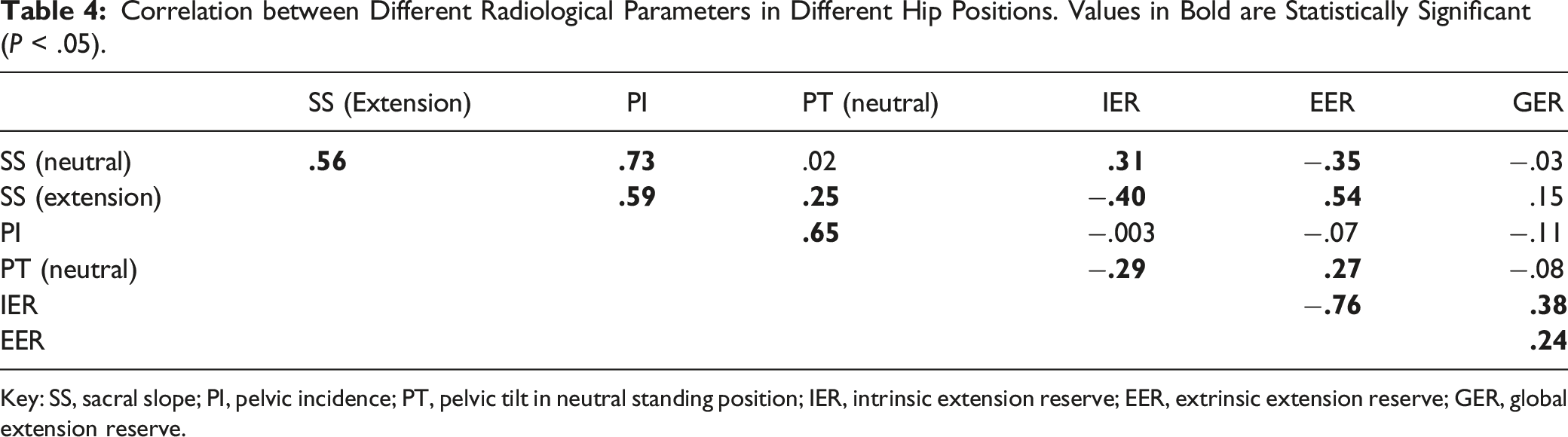
Key: SS, sacral slope; PI, pelvic incidence; PT, pelvic tilt in neutral standing position; IER, intrinsic extension reserve; EER, extrinsic extension reserve; GER, global extension reserve.
Radiological Parameters According to Roussouly Subtype. Statistical Significance with the P-Value (Kruskall-Wallis Test).
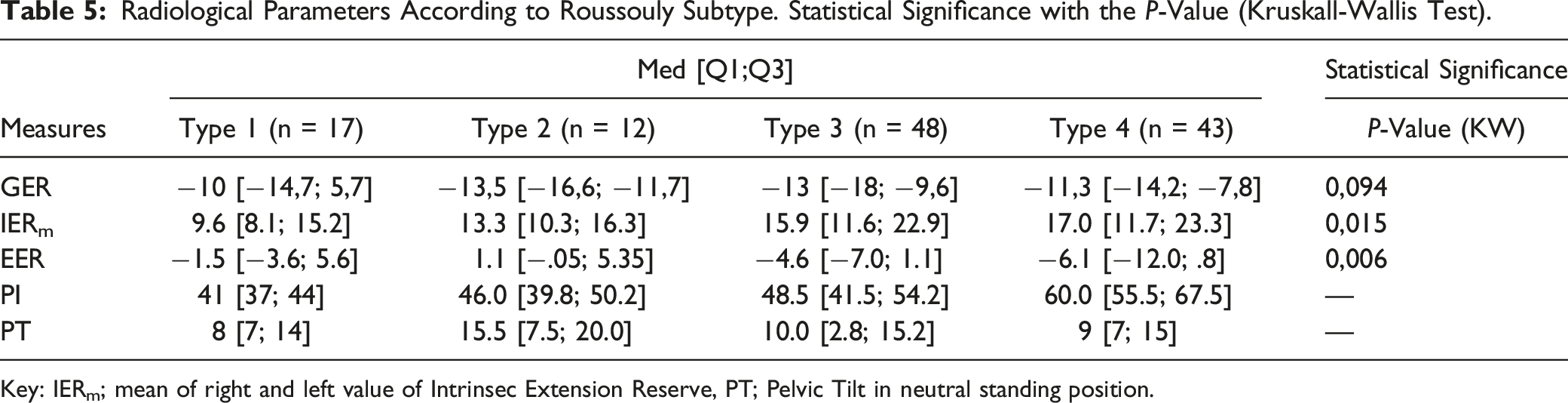
Key: IERm; mean of right and left value of Intrinsec Extension Reserve, PT; Pelvic Tilt in neutral standing position.
Comparison of IERm (Red Font) and EER (Blue Font) between Each Roussouly subtype (P-Values in Bold are Statistically Significant).
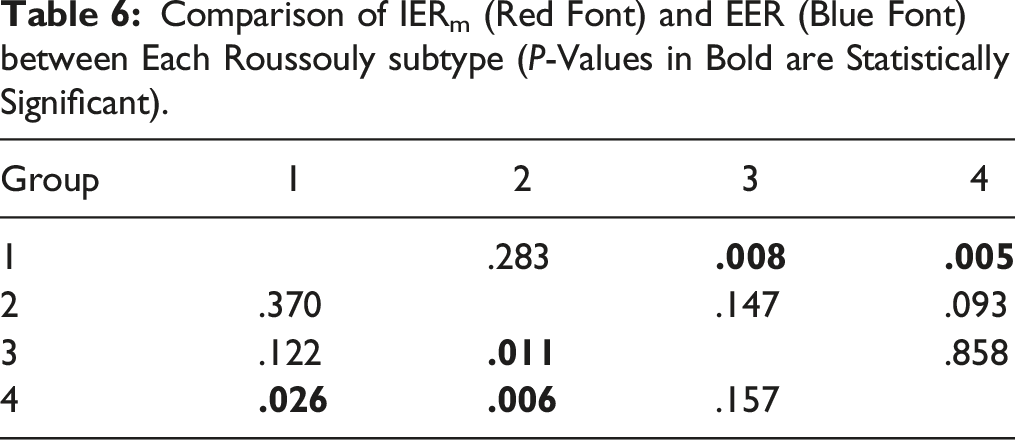
Considering the impact of pelvic incidence on extension reserve, no difference was found for EER (P = .814), IERm (P = .546), or GER (P = .176).
Furthermore, combining participants with low SS values (< 35°; Types 1 and 2) and others with SS values over 35° (Types 3 and 4), no difference was found when assessing the global extension reserve (P = .837)
Discussion
During surgery to correct spinal deformities or to perform total hip replacements (THR), it is important to evaluate ER. In spine surgery, integrating this value to restore sagittal alignment is essential to compensate for postural imbalances. As for THR, the ER and pelvic tilt related to the orientation of the acetabulum are involved in impingement and dislocation mechanisms. The influence of sagittal alignment of the spine and its influence on extension reserve has already been reported in the literature.11,14-16,19 However, integrating this into the specific analysis of the intrinsic coxofemoral and extrinsic pelvic components in subjects free from any spinal or hip pathology remains little reported.
This study used the EOS® system to characterize radiographic lumbopelvic measurements including the extension reserve of the lumbopelvic-femoral complex, highlighting movements specific to the hip joint (intrinsic) and the lumbopelvic complex (extrinsic).
To assess the IER we used the sacrofemoral angle, as devised by Lazennec et al and considered a reliable and reproducible representation of this parameter. 15 Compared with our results (GER = 12.93°, IER = 13.95°, and EER = −11.1°), their absolute values were slightly lower (GER = 8.16°, IER = 8.82° and EER = −.65°), perhaps reflecting their use of a 25 cm high step rather than a 40 cm high step like the one we used in our study.
IER and EER appeared to be negatively associated with one another and were unrelated to pelvic parameters. Sagittal alignment of the spinopelvic complex did not influence the global extension capacity, and there was no difference between either side (ie right vs left).
In participants with a sacral slope of up to 45°, pelvic involvement is important, as it tends to tilt in retroversion relative to contralateral hip flexion, resulting in a negative extrinsic extension reserve. This may explain the absence of any difference in global extension reserve between the different subgroups. Conversely, in participants with small sacral slope angles, the pelvis is anteverted during hip extension for most hip movements.
When considering the absolute value of the EER, pelvic tilt enabling a wider range of motion during extension is essential in participants whose SS is greater than 45°. Thus, the SS appears to influence the type of enrollment of lumbo-pelvic complex during hip extension. Participants with high SS values of up to 45° presented significantly higher values for IER than participants in Groups 1 and 2. Finally, Roussouly's subtypes seemed to be predictive of IER and EER variances even if no significant difference was established for global extension reserve in the various subtypes.
Rivière et al. 19 suggested classifying the lumbo-pelvic complex into "hip users" with a Type 1 lumbo-pelvic complex (stiff with PI down to 40°) and "spine users" with a Type 2 lumbo-pelvic complex (Type 2 pelvis with 40°<PI<60° and Type 3 pelvis with PI >60°). They described the hip users as having a greater compensatory range of motion in the hip during activities of daily living than spine users. However, in our study, no relationship was noted between PI and extension reserve considering the method of testing the lumbo-pelvi-femoral complex's extension capacity.
The strengths of this study are that it provides information on the extension reserve of the lumbo-pelvi-femoral complex. This is the first study conducted on young healthy participants using measurements based on high-definition whole-body EOS® imaging acquisitions with which the spine and lower limbs could be clearly and reliably visualized in different functional hip positions to report the influence of spinal alignment on hip function during extension. Using this particular approach, specific evaluation and measurements of pelvic enrollment can be highlighted.20‐23
However, this study is limited due to the small number of participants. Certain subgroups may have been poorly represented. It is also difficult to evaluate the influence of spine alignment particularly in Subgroup 1 (14.2 % of participants) and Subgroup 2 (10%) and the subsequent robustness of the statistical analysis for these 2 groups is poor. However, the distribution of the population in each group of this study did reflect the normal distribution seen in a Caucasian population like our cohort. 16 Moreover, combining these 2 groups into 1 did not appear to be appropriate for the analysis as their biomechanical behaviors were different: Group 1 participants had an increased but short lumbosacral lordosis, whereas Group 2 had straighter backs.
The sagittal spinal alignment of healthy population- 7 -subjects has recently been divided into 5 sagittal types 6. A new classification for people classified as Type 3 sagittal alignment has now been devised with a new, unusual sagittal structure with low-grade PI, very low or negative PT, and hyperlordosis 6. Due to the small number of participants in each group, we were unable to analyze according to this new classification. Furthermore, considering SS as on of the main parameters influencing hip extension, variations in the PI grade did not appear to be a determining factor for the Type 3 group.
Finally, we do acknowledge that the ability to evaluate the extension reserve was influenced by contralateral hip flexion, specifically, paradoxical pelvic retroversion during dynamic extension measurement, and the choice of a forward lunge as the main test for evaluating extension reserve inhibits the ability to fully assess the real extrinsic extension reserve for participants with a significant SS.
Conclusion
Global extension reserve is similar among the 4 different Roussouly classification types. However, considering the absolute value of pelvic tilt between a neutral position and in extension, pelvic mobility is greater in high neutral SS participants. Contralateral hip flexion influences pelvic tilt during dynamic hip extension. However, we found that there was an inverse correlation between IER and EER based on Roussouly subtypes, leading to sufficient compensation regardless of neutral lumbar-pelvic-femoral balance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.