
Abstract
Purpose:
Global sagittal spinal alignment undergoes changes on the basis of sagittal malalignment (trunk inclined forward) in natural degenerative progression. We hypothesized that this change would associate with the disease state of the degenerative lumbar spondylolisthesis (DS). This study aimed to evaluate the global sagittal spinal alignment of low-grade DS by classifying in accordance with sagittal vertical axis (SVA).
Methods:
The DS group was classified into three types according to the adult spinal deformity classification: type 1, SVA < 40 mm; type 2, 40 mm ≤ SVA < 95 mm; and type 3, 95 mm ≤ SVA. Age and sagittal spinal parameters (thoracic kyphosis, lumbar lordosis (LL), sacral slope (SS), pelvic tilt (PT), and pelvic incidence (PI)) were compared among three types.
Results:
There were statistically significant differences in age, LL, PI, and PT among the three types. In comparison between two types, there was a statistically significant difference between type 1 and type 2 and between type 1 and type 3, but not between type 2 and type 3 in these parameters. PI tended to increase as the type increases. Furthermore, there was significant difference between types 1 and 3.
Conclusion:
We evaluated the features of the DS types classified by sagittal alignment. Large PI is one of the risk factors for SVA deterioration of DS. PI may be involved in the onset and progression of DS.
Keywords
Introduction
Degenerative lumbar spondylolisthesis (DS) was first described by Junghanns in 1930. 1 It occurs mostly at the L4/5 level in people over 40 years old. 2 Many factors associated with the incidence of DS have been reported including the shape of vertebral bone, the shape of the sagittal facet joint and female, among others. 2 –5 Recent studies have pointed out significant contributions of spinal degeneration by age-related changes, and some studies have particularly stated the significant role of global sagittal spinal alignment in the onset of spondylolisthesis. 6 C7 plumb line is the most commonly used index of the global balance. This parameter called “sagittal vertical axis” (SVA) has been historically quantified by measuring the position of a vertical line originating at the center of the C7 vertebral body with respect to the posterior superior corner of S1. Pelvic incidence (PI) was defined as the pelvic morphologic angle. 7 This angle, which represents the tilt of the sacrum relative to the pelvis, is unaffected by posture and remains constant for individuals, assuming that the sacroiliac joint is not mobile. 7 Accordingly, it is believed that this angle is the key parameter in determining the global sagittal spinal alignment.
Regarding global sagittal spinal alignment of DS, a recent study described that obtaining optimal alignment after surgery is important for achieving long-term surgical results. 8 A retrospective cohort study analyzed postoperative sagittal alignment in patients with DS showed that poor postoperative sagittal alignment with SVA >50 mm resulted in significantly worse clinical outcomes over a mean follow-up of 3 years. 9 The pre- and postoperative sagittal malalignment are associated with the development of DS. 10 These studies suggest the importance of SVA as parameter affecting the long-term outcome of DS after surgery.
In the present study, we hypothesized that global sagittal spinal alignment would undergo changes on the basis of sagittal malalignment in natural DS progression. Thus, we specifically paid attention to sagittal alignment and classified the DS type by SVA. This study aimed to evaluate the features of the DS types classified by sagittal alignment.
Materials and methods
The subjects were patients who underwent surgery for spinal degenerative disease and were able to take lateral whole-spine standing radiographs from January 2006 to September 2016 at our hospital. Among them we examined 193 patients with degenerative low-grade spondylolisthesis (L4/5 level). We excluded patients with severe listhesis (grades 2–4; Meyerding grade), spondyloscoliosis (over 30° of Cobb’s angle), severe hip or knee osteoarthritis who could not stand with their knees extended, and severe kyphosis caused by compression fracture. Patients with high-grade spondylolisthesis (grades 2–4) were excluded due to the small number of subjects in our facility and did not reach the sufficient number for decent statistical analyses. In addition, these subjects may have different pathology, because they often accompanied severer scoliosis together with lumbar kyphosis. We also excluded patients with dysplastic, isthmic, traumatic, and pathological listhesis. Furthermore, we excluded patients who needed to flex their knees to compensate for sagittal alignment.
Of the 193 patients examined, 112 were enrolled as subjects of this study (39 men and 73 women; mean age 68.6 ± 10.3 years; DS group). For the control group, 84 volunteers free of lumbar disease were enrolled (57 men and 27 women; mean age 66.8 ± 9.3 years; Control group) (Table 1).
Characteristics of patients and control groups.
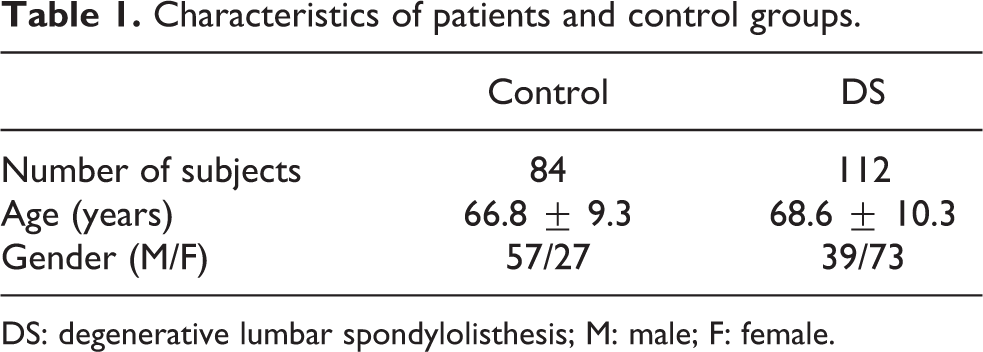
DS: degenerative lumbar spondylolisthesis; M: male; F: female.
The DS group was further classified into 3 types according to the adult spinal deformity classification by Schwab et al. 11 : type 1, SVA < 40 mm; type 2, 40 mm ≤ SVA < 95 mm; and type 3, 95 mm ≤ SVA (Figure 1, Table 2). We took lateral whole-spine standing radiographs of patients standing in the fits-on-clavicles position. In accordance with the measurement method described by Legaye et al., 7 we measured SVA (distance between the C7 plumb line and the posterior superior corner of the sacrum, an index of the anterior inclination of the trunk), thoracic kyphosis (TK, angle from the upper end plate of Th4 to the upper end plate of Th12), lumbar lordosis (LL, angle from the upper end plate of L1 to the upper end plate of S1), sacral slope (SS, angle between the sacral plate and the horizontal plane), pelvic tilt (PT, angle between the line connecting the midpoint of the sacral plate to the axis of the femoral heads, and the gravity line), and pelvic incidence (PI or pelvic morphologic angle, angle between the perpendicular line to the sacral plate at its midpoint, and the line connecting that point to the middle axis of the femoral heads).

Classification of degenerative lumbar spondylolisthesis: (a) type 1, SVA < 40 mm; (b) type 2: 40 mm ≤ SVA < 95 mm; and (c) type 3: 95 mm ≤ SVA. SVA: sagittal vertical axis.
Classification of DS.
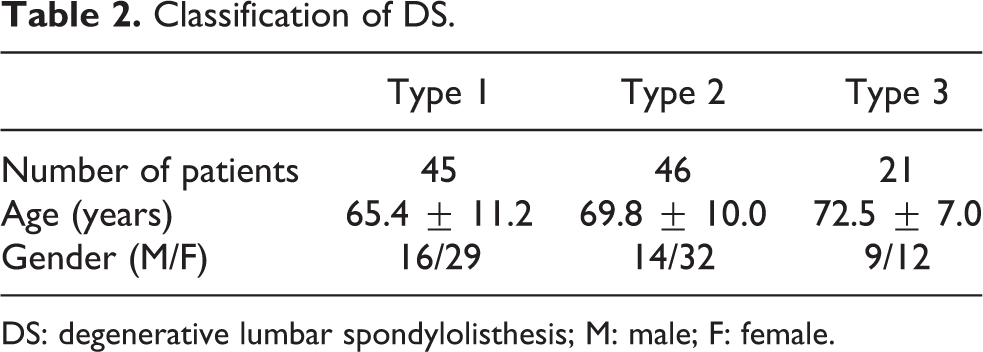
DS: degenerative lumbar spondylolisthesis; M: male; F: female.
We compared each global sagittal spinal alignment parameter between the DS and the Control groups and compared the DS types classified by sagittal alignment. Then, we evaluated the features of the DS types classified by sagittal alignment. This study was approved by the ethics committee of our institute.
Statistical analyses were performed using the JMP software package version 12.0 (SAS Institute Inc., Cary, North Carolina, USA). The value of p < 0.05 was considered to indicate a statistically significant difference. Mann–Whitney U test was used for analysis between two groups, and Kruskal–Wallis test was used for analysis among three groups.
Results
Comparisons of the global sagittal spinal alignment parameters between the DS and the Control groups showed that SVA, PI, and PT were significantly larger and LL and SS were significantly smaller in the DS group than in the Control group. However, there was no statistically significant difference in TK (Table 3). This indicates that there is a characteristic sagittal alignment (larger PI, human trunk incline, loss of LL, and large PT) in DS. For comparisons among the three DS types as classified by sagittal alignment, there were statistically significant differences in age, LL, PI, and PT (Table 4). However, in comparisons between two of the DS types, there was a statistically significant difference between type 1 and type 2 and between type 1 and type 3, but not between type 2 and type 3 in terms of age, LL, PI, and PT (Figure 2). This indicates that the sagittal alignment in type 1 shows larger LL than those in types 2 and 3, with a maintained pelvic anteversion including a smaller PI (Figure 2). On the other hand, there was no significant difference in TK and SS among the three types.
Global sagittal spinal alignment in control and DS groups.

DS: degenerative lumbar spondylolisthesis; SVA: sagittal vertical axis; TK: thoracic kyphosis; LL: lumbar lordosis; SS: sacral slope; PT: pelvic tilt; PI: pelvic incidence.
Comparison of age and each parameter among types 1, 2, and 3 in DS.

DS: degenerative lumbar spondylolisthesis; SVA: sagittal vertical axis; TK: thoracic kyphosis; LL: lumbar lordosis; SS: sacral slope; PT: pelvic tilt; PI: pelvic incidence.

Comparison between parameters of DS groups: (a) age, (b) TK, (c) LL, (d) SS, (e) PT, and (f) PI. SVA: sagittal vertical axis; TK: thoracic kyphosis; LL: lumbar lordosis; SS: sacral slope; PT: pelvic tilt; PI: pelvic incidence.
Discussion
Barrey et al. showed that the characteristic global sagittal spinal alignment of DS was decreased lumbar lordosis, large PT, and large PI, and they concluded that such spinopelvic shape was one of the major causes of DS. 12 The present results showed that DS patients had larger SVA, PI, and PT compared to the Control group in line with reported previous studies; however, LL and SS were smaller in DS patients which contradicted previous studies (Table 3). 12 –16 Generally, SVA, TK, and PT increase and LL decreases with aging. When SVA becomes overly enlarged with aging, thoracic kyphosis decreases to maintain an upright position as a compensatory mechanism. 17 However, once this spinal compensatory mechanism reaches its limit, recruitment components other than the spine, including the pelvis, hip joint, and knee joint, take place. 18 In addition, it will be possible that SVA increased even further with decreasing LL, because subjects in this study had symptom of spinal canal stenosis. 19
Regarding global sagittal spinal alignment, Roussouly et al. described four types of LL according to PI and SS as pelvic parameters, and they specifically reported that type 4, which had large PI and SS (PI > 50° and SS > 45°, respectively), was associated with spondylolysis or spondylolisthesis. 20 Barrey et al. also reported that DS occurred more in patients having a larger PI. 12 In addition, sagittal malalignment has also been reported to be associated with the development of DS. 10 In the present study, DS patients also had larger PI and large PT. Patients having larger PI tend to compensate the loss of LL by large PT, 8,20 therefore, it is possible that in those patients, a large load will be directly applied to the lumbosacral region leading to the cause and progression of L4 slippage.
Regarding SVA, our results showed that SVA of the DS group included a wide range of variation (Table 3), and lumbo-pelvic sagittal alignment differed depending on the type (Figure 2). It should be noted that the ratio of gender between the control and the DS groups was different. However, the influence of this can be minimal, because recent study showed that there was no difference in LL, PI, and SVA between males and females of age over 50 years in asymptomatic individuals. 21 LL and SS in type 1 were significantly larger than those in types 2 and 3 (Table 4). Some previous studies reported different sagittal alignment of DS with large LL and SS as typical DS alignments unlike our result. 12 –16 This may be due to the difference in taking the SVA into consideration of the global sagittal spinal alignment, and this may indicate the importance of SVA for the evaluation of sagittal spinal alignment in DS. Type 1 showed small PI, large LL, and large SS, but PT was small and the pelvis did not tilt backward. Type 2 showed small LL and large PT compared with type 1. Type 3 showed no significant change in LL and PT compared to type 2 but tend to show smaller LL and larger PT than type 2 (Figure 2). These processes (change in global sagittal spinal alignment during the course of progression of type) reflected typical alignment changes due to aging. 22 The mean age also increased with the progression of type in this study (Table 3), suggesting that balance failure would be affected by general age-related degenerative changes. On the other hand, from the view point of PI (which should not be affected by aging), it tended to be larger as the type increases and the difference between types 1 and 3 was statistically significant. This indicates that large PI can be one of the risk factors of SVA deterioration in DS patients and suggests that pelvic morphology (PI) is involved in the onset and progression of DS (Figure 1).
The limitations of this study are that it uses a retrospective cross-sectional study design and that longitudinal studies including surgical results have not been conducted. Multiple factors such as gender, % of slip, slip angle, the shape of the facet joint, and the height of the intervertebral disc, which are involved in the onset of DS, were not studied. Furthermore, change in SVA due to symptom was not examined because of its invariability and a possible compensation of SVA by other elements, including pelvis was not examined. However, to the best of our knowledge, this is the first study to propose the classification including global sagittal spinal balance, which is considered clinically useful.
Conclusions
The global sagittal spinal alignment of DS showed large PI, SVA, and PT and small LL and SS. In the DS patients, large PI is one of the risk factors for SVA deterioration. PI may be involved in the onset and progression of DS.
Footnotes
Authors’ note
This study is a retrospective clinical research using lateral whole-spine standing radiographs. This study was approved by the Institutional Review Board of our institution. All subjects provided written informed consent after explanation of the experimental protocol.
Acknowledgements
We gratefully acknowledge the members of spine surgery group in our university for the contribution toward the fundamental findings of the current study. We are indebted to the Department of International Medical Communications of Tokyo Medical University for the editorial review of the English manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.