
Abstract
Study Design
Retrospective cohort study.
Objectives
Identify optimal lumbar lordosis in adult deformity correction to achieve age-adjusted targets and sustained alignment.
Methods
Surgical adult spinal deformity patients reaching an age-adjusted ideal alignment at one year were identified. Multilinear regression analysis was used to identify the relationship between regional curvatures (LL and TK) that enabled achievement of a given global alignment (T1 pelvic angle, TPA) based on pelvic incidence (PI).
Results
347 patients out of 1048 available reached their age-adjusted TPA within 5° (60-year-old, 72% women, body mass index 29 ± 6.2). They had a significant improvement in all sagittal parameters (except PI) from pre-operative baseline to 1 year following surgery (P < .001). Multilinear regression predicting L1-S1 based on TK, TPA, and PI demonstrated excellent results (R2 = .85). Simplification of the coefficients of prediction combined with a conversion to an age-based formula led to the following:
Conclusion
This study provides a simple guideline to identify the amount of LL needed to reach a given alignment (i.e., age-adjusted target) based on PI and associated TK. Implementation of this predictive formula during pre-operative surgical planning may help to reduce unexpected sub-optimal post-operative alignment outcomes.
Keywords
Introduction
Adult spinal deformity (ASD) has a significant impact on disability.1‐3 Subsequent surgical correction has been correlated to improvement in health-related quality of life (HRQoL) measures. 4 Sagittal malalignment within ASD patients results in predictable compensatory changes in order to maintain standing alignment.5‐8 The key compensatory mechanisms involve accommodations within specific regions of the spine which may alter the spinopelvic relationship and at certain extremes alter alignment of the lower extremities. 7 Dubousset’s “conus of economy” illustrates the importance of spinopelvic balance in maintaining upright posture and minimizing energy expenditure. 9 The relationship between spinal regions in compensatory settings and reciprocal changes from operative intervention has been highlighted in recent studies.10‐12 Flatback deformity illustrates the setting in which spinopelvic and lower extremity compensatory changes aid in upright posture, sometimes resulting in compensatory thoracic hypokyphosis.7,8,10 In order for the thoracic spine to effectively compensate, the spine must be “non-rigid” and be able to provide sufficient muscular recruitment, however, the clinical impact of this compensatory mechanism remains debatable.7,10,13 Regional correlations between thoracic kyphosis (TK), lumbar lordosis (LL) and pelvic incidence (PI) exist, yet the direct relationship between TK and PI remains unclear in the current literature. 14 The limitations of these relationships make predictions of regional spinal alignment difficult.
It has become apparent that multiple factors impact surgical outcomes for ASD patients. Formulas that aim to predict optimal surgical correction are limited and fraught with complex regional spinal relationships.5,15 The myriad of factors impacting deformity correction have been the focus of recent predictive equations in ASD surgery.16,17 One such study established a validated, simplified formula, LL=(PI+TK)/2+10, to estimate optimal regional spinal alignment based on PI and TK. 16 More recently, Lafage et al. emphasized age as an important metric in surgical correction, redefining the alignment threshold and goals of corrective surgery. 18 However, there remains no validated predictive formula incorporating the proportionality among sagittal curvatures (LL and TK) needed to reach a given global alignment based on the patient’s age. The purpose of this study is to establish a validated age-based, patient-specific formula to aid in obtaining effective sagittal alignment.
Materials and Methods
Patient Sample
This is a retrospective review of a prospective multicenter database of ASD patients. Enrollment occurred between January 1, 2009 and December 31, 2018 among 22 sites. Institutional Review Board (IRB) approval at each of the 22 participating sites was obtained prior to conducting the study (IRB No. 2014-357). Informed consent was obtained from all participating patients. Adult patients older than 18 years old, radiographic inclusion criteria were at least one of the following: Cobb angle ≥ 20°, sagittal vertical axis (SVA) ≥ 5 cm, pelvic tilt (PT) ≥ 25°, and TK ≥ 60°. Patients were excluded if they had malignant, infectious, traumatic or neuromuscular causes of scoliosis. Additional inclusion criteria specific to this study were 1-year follow-up and patients’ post-operative T1 pelvic angle (TPA) matching age-adjusted alignment parameters based on the following formula: (age-55)/2 + 16, which served as the reference for age alignment. 18 Patients’ post-operative TPA determined to be within 5˚ of the TPA matching age-adjusted alignment were considered as reaching “ideal age-adjusted” alignment.
Data Collection
Demographic information for each patient was collected and summarized based on age, sex and body mass index (BMI). Classic radiographic sagittal parameters, as seen in Figure 1, were defined as PI, PT, LL, PI-LL, TK, TPA, and SVA. In the coronal plane, Cobb angles were measured in addition to the C7 plumb line. The Scoliosis Research Society (SRS)-Schwab classification was used to describe the deformities among the cohort. The following operative details were identified: type of osteotomy, posterior lateral fusion, interbody fusion, posterior fusion length, upper-most and lower-most instrumented vertebra. Intraoperative measures included estimated blood loss and operative time. Classic radiographic sagittal parameters: PI, PT, LL, PI-LL, TK, TPA and sagittal vertical axis.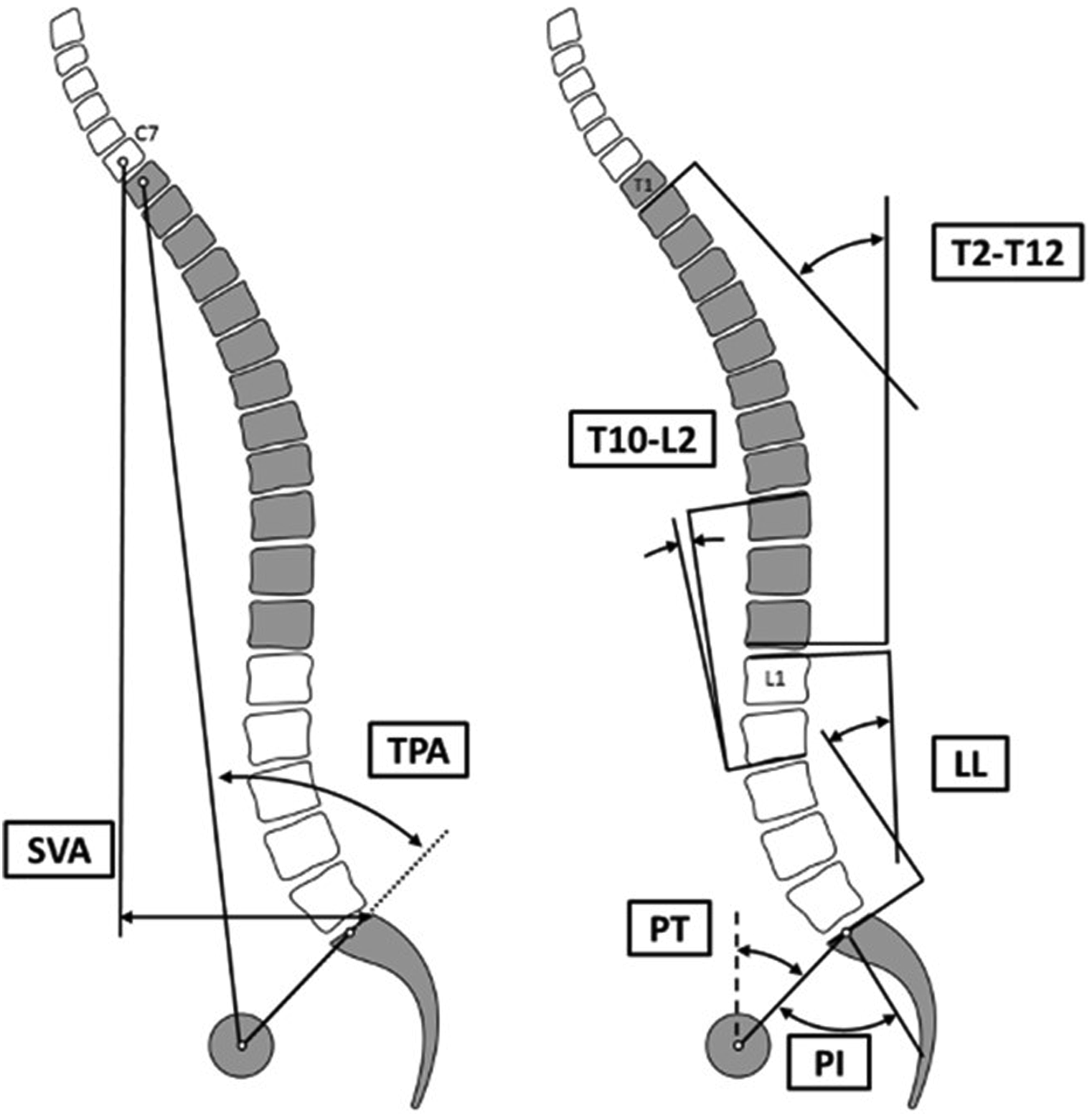
Statistical Analysis
Pre-operative information was collected and analyzed with rates for categorical variables and means with standard deviation and percentiles for continuous variables. Data distribution was investigated using Kolmogorov-Smirnov test for normal distribution. Pre- to post-operative analyses of results were carried out using paired t-test and Wilcoxon signed rank test as appropriate. After assessing rates of patients reaching TPA age-adjusted alignment post-operatively, independent t-test or Mann–Whitney U test were utilized for comparison. Multilinear regression was used to predict post-operative curvatures with LL as a function of PI, TK, and TPA. Our predictive formula was simplified along with integration of age-adjusted targets. Error of prediction used the mean error, signed difference between prediction and actual value to evaluate for bias. Mean absolute error, absolute difference between prediction and actual value, was used to evaluate for accuracy. IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, N.Y. USA) was used for statistical analysis with P < .50 considered as significant.
Results
Cohort Description
Cohort’s Sagittal Parameters by Quartiles.
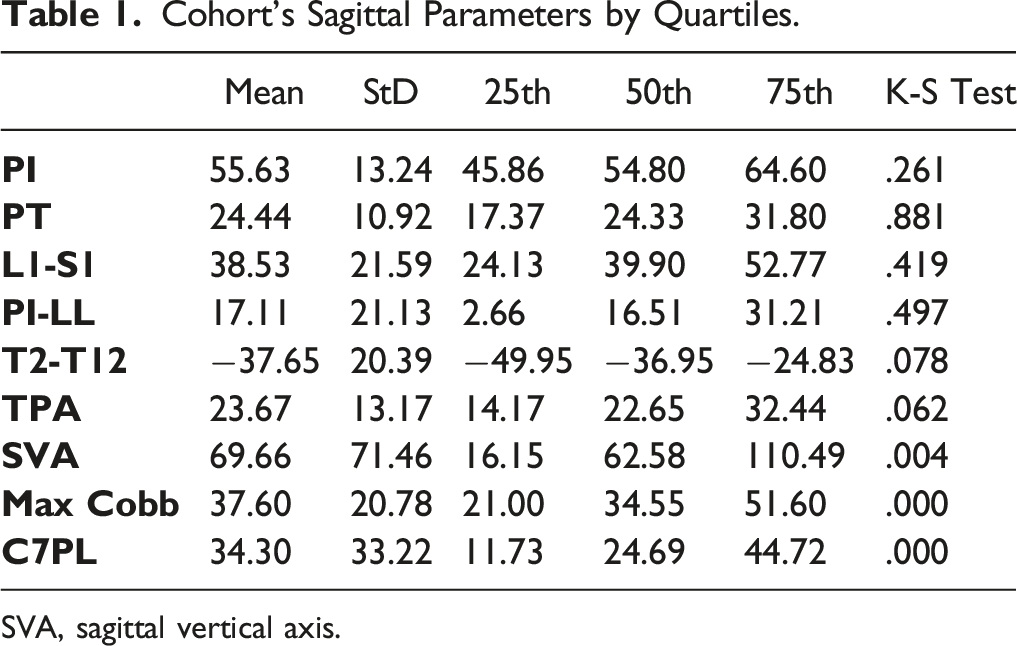
SVA, sagittal vertical axis.
Pre- to Post Change in Sagittal And Coronal Alignment.
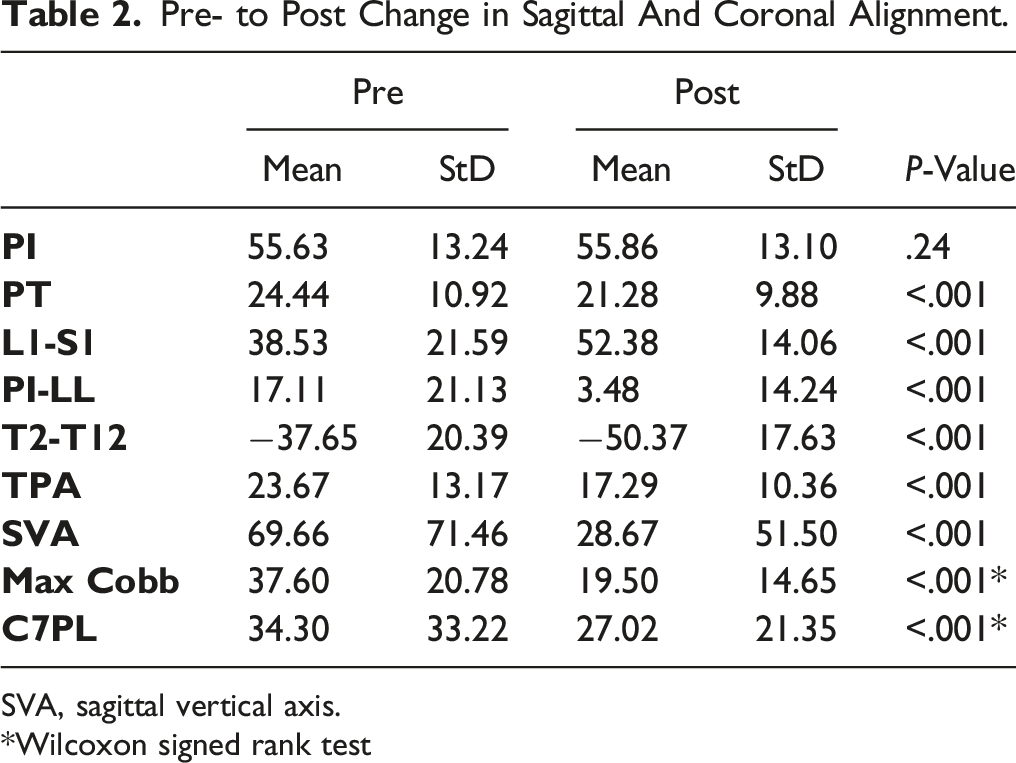
SVA, sagittal vertical axis.
*Wilcoxon signed rank test
Surgical Treatment
Surgical details for our cohort demonstrated that 70.6% underwent an osteotomy (18.2% with 3-column osteotomy), and 64.8% received an interbody fusion. The average length of the fusion construct was 10.6 ± 4.4 levels, average estimated blood loss (EBL) was 1706 ± 15.14 ml, and intraoperative time of 431 ± 180 minutes. Of the patients that received interbodies, trans-foraminal interbodies (27.4%) were the most common, followed by anterior interbodies (24.6%), lateral interbodies (15.8%), and posterior interbodies (3.6%). In an effort to group types of deformity corrections based on common construct lengths, we identified 37% of patients as “T4-pelvis” fusion (mean: 14.9 ± 2.6 fused levels) and 47% as “T10-pelvis” fusion (mean: 9.5 ± 1.5 fused levels). Comparisons between patients reaching age-adjusted TPAs and those that did not revealed no significant differences in type of osteotomy (P = .240), interbody utilization (P = .895), number of levels fused (P = .095), or EBL (P = .329).
Lumbar Lordosis Formula
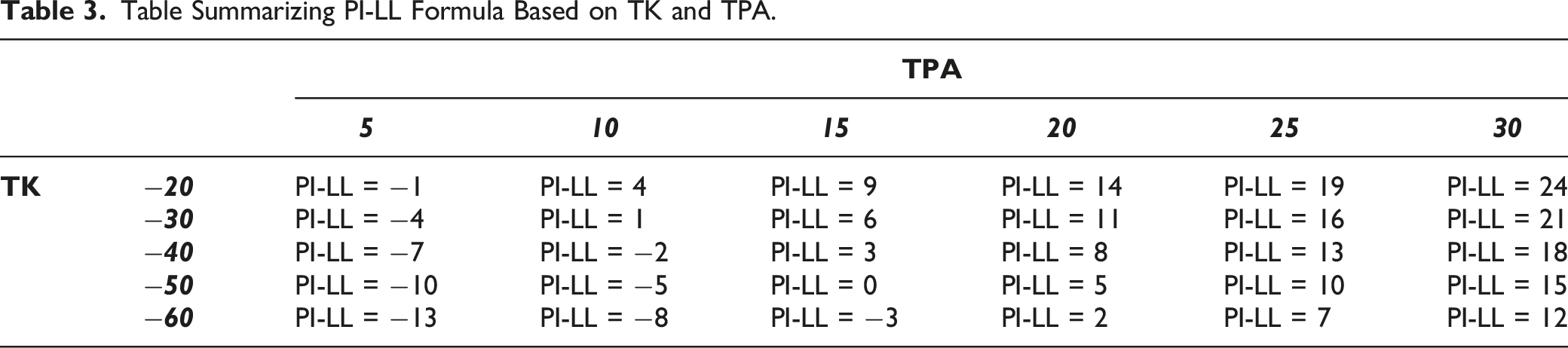
Among patients who reached age-adjusted post-operative alignment, multilinear regression based on TK, TPA and PI significantly predicted L1–S1 lumbar lordosis, with a r-square of .85. Simplification of the coefficients of prediction led to the following equation: LL = PI −0.3TK–TPA (mean error [ME] = 1.3°, absolute error [AE] = 4.5°). Figure 2 demonstrates application of this formula utilizing an age-based TPA target for a 56-year-old with thoracic hyperkyphosis and a resulting target LL of 45° (post-operatively achieved LL of 44). Internal validation on patients with an age-adjusted alignment revealed similar accuracy across the entire age-adjusted TPA spectrum (ranges of LL errors: ME = .2° to 1.7°, AE = 4.0° to 5.3°). Table 3 represents a simplification of the PI-LL target by value of TPA and TK. This 56-year-old patient presented with a pre-operative TK of −59° and a PI of 43°. The theoretical lumbar lordosis required to reach an age-adjusted TPA target of 16° without modification of TK was calculated as LL = PI −.3*(TK) −16 = 44.7° compared to 34.7° if only accounting for age and PI. At 1-year follow-up, this patient had a TPA of 15°, with a LL of 44° and a TK of −62°. Table Summarizing PI-LL Formula Based on TK and TPA.
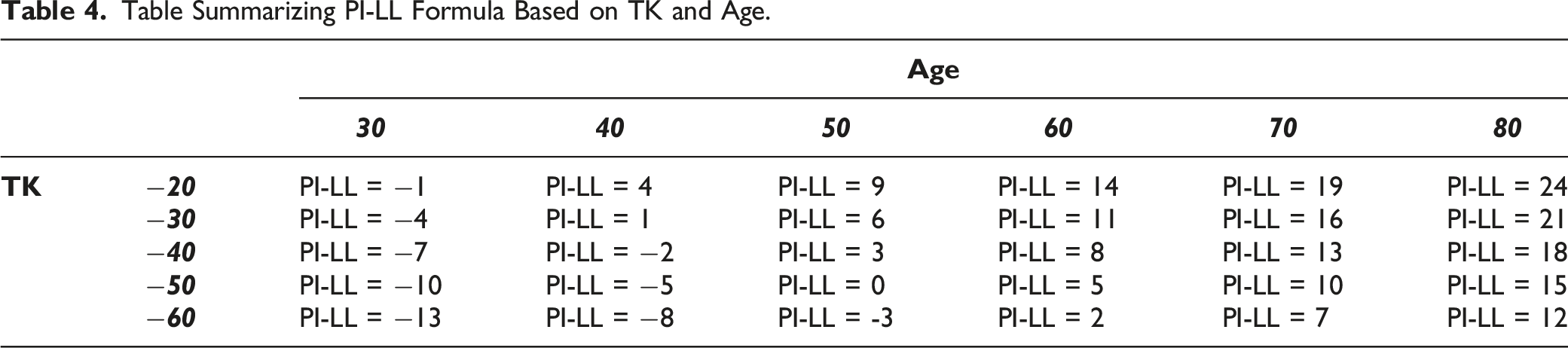
The formula, LL = PI −0.3TK −0.5Age + 10, was created with integration of age-adjusted alignment targets (ME: −.4°, AE: 5.0°). Figure 3 illustrates utilization of our formula in a 54-year-old with thoracic hypokyphosis and a resulting target LL of 33° (post-operatively achieved LL of 35°). Table 4 represents a simplification of the PI-LL target by value of age and TK This 46-year-old patient presented with a pre-operative TK of −14° and a PI of 42°. The theoretical lumbar lordosis required to reach an age-adjusted alignment was calculated as LL = PI −.3*(−14) −.5*46 + 10 = 33° compared to 39.4° if only accounting for age and PI. At 1-year follow-up, this patient matched his age-adjusted TPA (13°), with a Lordosis of 34° and a Kyphosis of −15°. Table Summarizing PI-LL Formula Based on TK and Age.
Discussion
Current literature has identified patients at greater risk of post-operative failure and complications; however, current predictive formulas identifying optimal sagittal alignment goals remain limited.19,20 Previous formulas addressing regional considerations are overly simplistic and lack patient-specific factors known to impact outcomes. Our equation is the first to address predictive “tailoring” of sagittal alignment, optimizing the relationship between TK and LL, while incorporating age-adjusted alignment. Our study attempts to address regional spinal alignment while incorporating updated and validated patient-specific parameters. Our predictive formula identifies ideal thoracic and lumbar relationships for individual patients undergoing spinal deformity correction surgery in order to reduce sub-optimal alignment outcomes.
Lafage et al. defined age-specific objectives for sagittal realignment furthering goals of patient-specific surgical planning. 18 Advancements in our understanding of radiographic sagittal parameters, such as TPA and reciprocal thoracic kyphosis, and the resulting effect of realignment surgery have expanded our abilities to customize surgical plans for ASD patients. Optimizing PI-LL and sagittal vertical access (SVA) remains a major focus when planning adult deformity correction. However, these parameters in isolation do not address the spine and pelvis as a unit. PI-LL does not account for an overcompensated PT and TK, which may predispose patients to adjacent segment pathology, proximal junctional kyphosis, and pseudoarthrosis.21,22
A recent study by the International Spine Study Group (ISSG) proposed a validated formula to estimate the optimal LL based on PI and TK, LL = (PI + TK)/2+10. 16 This modified formula accounts for abnormal TK and provides estimates of optimal regional alignment in the thoracic and lumbar regions. In order to better assess sagittal alignment, the ISSG proposed T1 pelvic angle (TPA) as a comprehensive spinopelvic parameter, which unlike SVA, does not vary with postural compensatory mechanisms. 23 Among our cohort, TPA percentile groups correlated with post-operative LL. Further statistical analysis and incorporation of TPA via simplification of the coefficients of prediction produced the equation LL = PI −0.3TK–TPA. Interestingly, analysis of age-adjusted alignment among our cohort revealed comparable accuracy across the entire age-adjusted TPA spectrum. The incorporation of age-based parameters within our formula in conjunction with the spectrum of our TPA led to our proposed equation, LL = PI −0.3TK −0.5Age + 10.
Figures 2 and 3 highlight some of the nuances between previous formulas and our equation in determining post-operative alignment goals. These figures illustrate patients of similar age, PI and surgical construct (T10-pelvis), yet the former has thoracic hyperkyphosis and the latter thoracic hypokyphosis leading to different LL. Theoretical LL based on TPA, Figure 2, and theoretical LL using our age-based formula accounting for thoracic parameters, Figure 3, resulted in different outcomes despite similar key parameters (age and PI). Guidelines accounting for age and PI only would have resulted in similar lumbar curvature for these patients. This would have led to an over-correction (more posterior global alignment) for patient in Figure 3 and an under correction (more anterior global alignment) for patient in Figure 2. Although these patients share similar pre-operative characteristics, our formula demonstrates better patient-specific capabilities of predicting successful post-operative outcomes.
This study has several limitations that should be considered. First, this is a multicenter patient database which utilized plain radiographs from multiple centers without standard radiographic protocols. Similarly, supine plain radiographs were not included for patients in our cohort which could further capture curve flexibility, especially in the setting of compensation. Given the limited ability to assess curve flexibility among our study cohort, selection of fusion construct and length were based on individual surgeon assessment. Furthermore, indications and techniques of surgeries were based on the judgment and experience of the surgeons across multiple centers and not based on standardized protocols. There are multiple strengths of this study. The generalizability of our proposed predictive equation is based on a large multicenter cohort. Our equation incorporates previous predictive equations and patient-related factors to provide a validated predictive equation accounting for age-adjusted impact.
This study provides a method to determine practical alignment goals while incorporating considerations for age, overall sagittal alignment and compensatory mechanisms. Our formula is an effort to provide a validated, predictive formula accounting for current risk factors known to have a significant impact on spinal deformity correction. It is important to appreciate alignment in the greater context of maintaining a harmonious spinal unit. Spinal alignment depends on a multitude of factors, including soft tissue response to gravity, bony alignment and neuro-sensory modulation. 24 Ultimately, individualized care formulas, such as the one proposed in this paper, should be implemented in conjunction with comprehensive evaluation to achieve the goals of surgery.
Conclusion
Predicting successful outcomes with ASD surgery remains a focus of research, especially as the impact of patient-specific factors is further studied. Formulas accounting for regional parameters, compensatory mechanisms and sagittal alignment remain imperfect in planning and predicting durable outcomes. Regional alignment considerations in ASD remain simplistic and may lead to over- or under-estimation of alignment goals. This study expands on previously validated predictive formulas by incorporating age-adjusted targets based on PI and associated TK using measures from patients with optimal and sustained correction. Implementation of the predictive formula, LL = PI −0.3TK −0.5Age + 10, during pre-operative surgical planning can help to reduce unexpected sub-optimal post-operative alignment outcomes. Our findings provide a key step in understanding of the ideal thoracic/lumbar relationship and promote a new predictive formula to reduce sub-optimal alignment outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval
Institutional Review Board (IRB) approval was obtained at all institutions included in this study