
Abstract
Study Design
Cross-sectional survey.
Objective
Surgical treatment of degenerative lumbar spondylolisthesis is remarkably varied due to heterogeneity of clinical-radiological presentations. This study aimed to assess which spinopelvic radiological parameters were considered for decision-making.
Methods
Survey distributed to International AO Spine members to analyze surgeons’ considerations for treatment. Data collected includes demographics, training background, years of experience, and treatment decisions based on various radiographical findings, including segmental and global spinopelvic parameters.
Results
From 479 responses, the most frequently radiological parameter considered was slippage on dynamic X-rays (79.1%), followed by disc height (78.9%), global sagittal balance SVA (71.4%), and PI-LL mismatch (69.7%), while the least important was absolute spondylolisthesis on static lateral radiograph (22.8%). Fellowship-trained surgeons were likelier to use SVA (OR = 1.73, 95% CI = 1.02-2.99, P = 0.049), and disc height (2.13, 1.14-3.98, P < 0.05). There was no difference between orthopedics and neurosurgery in applying SVA and PI-LL mismatch. Surgeons from Asia Pacific emphasizes segmental lordosis (2.39, 1.11-5.15, P = 0.026) as from Latin America (2.55, 1.09-5.95, P = 0.030) and Middle East (4.33, 1.66-11.28, P = 0.003). However, surgeons from Latin America and Middle East also significant consider disc height (2.95, 1.07-8.15, P = 0.037) and (3.03, 1.04-8.83, P = 0.043), respectively. Additionally, the surgeons’ age was associated with using angular motion on flexion-extension radiographs, and volume of treated cases yearly with consideration for disc height.
Conclusions
Treatment of degenerative lumbar spondylolisthesis was influenced by slippage on dynamic radiographs, disc height, global alignment, and PI-LL mismatch. Surgeons’ age and Region, fellowship-trained, and volume of treated cases were significantly associated to apply these radiological parameters.
Keywords
Introduction
Surgical treatment of lumbar spondylolisthesis remains controversial due to the high heterogeneity of the clinical and radiographical presentations and surgeons’ variation in surgical practices. Surgeon’s preferences may range from the decision-making for conservative vs surgical treatment, 1 decompression alone vs decompression with fusion,2,3 open vs minimally invasive surgery, 4 direct or indirect decompression, 5 stand-alone vs circumferential fusion, 6 in-situ fusion without instrumentation vs reduction with instrumented fusion, 7 traditional surgery vs endoscopic surgery, 8 different lumbar interbody fusion approaches 9 and osteobiologics filling the cage 10 are examples of the wide variation of practice in the treatment of lumbar degenerative spondylolisthesis across the globe.
In recent years, there has been increasing awareness and adoption of applying the understanding of local segmental and spinopelvic alignment in treating degenerative lumbar conditions to avoid iatrogenic deformity. 11 While the idea of improving segmental lordosis and spinopelvic alignment to improve clinical outcomes and reduce pos-operative complications such as adjacent segment disease and pseudoarthrosis has not been proven, there is still significant educational efforts to emphasize correction of segmental and spinopelvic alignment in degenerative spine surgery to improve surgical outcomes. Some studies have shown that improving preoperative radiological parameters in degenerative lumbar surgery is correlated to better functional outcomes and quality of life during follow-up. Therefore, it is imperative to consider segmental sagittal spinopelvic alignment for improving surgical results. 12
The aim of the current study was to assess which spinopelvic segmental and global radiological parameters are deemed important by spine surgeons, and whether demographics, training background, and practice patterns affect the use of those radiographic parameters during the decision-making process in the management and surgical planning of degenerative lumbar spondylolisthesis.
Methods
Study Strategy
To investigate the surgeon’ considerations regarding radiological spinopelvic parameters in degenerative lumbar spondylolisthesis a survey was distributed to over 6000 AO Spine members internationally and was conducted electronically in March 2023 through the AO Knowledge Forum Degenerative. Demographics, training background, clinical experience, and other surgeon characteristics were included in the survey, in addition to questions related to spinopelvic parameters considered by the surgeons when a decision on treatment is necessary. The study did not required inform consent or regulatory approval as there was no patient data or clinical interventions involvcd.
Study Criteria
Surgeon demographic information was collected including geographic region (Asia Pacific, North America, Latin America, Europe and Southern Africa, and Middle East and Northern Africa), gender, age, years of practice (categorized into predefined range clusters for ease analysis), specialty, practice setting, and volume of spondylolisthesis treated yearly. Finally, the surgeons were asked regarding which radiological spinopelvic parameters are considered for the decision-making in degenerative lumbar spondylolisthesis, including the following: • Slippage on static radiological exams and dynamic flexion-extension radiographs • Angular motion on flexion-extension radiograph • Pelvis incidence – Lumbar lordosis (PI-LL) mismatch • Global sagittal alignment SVA • Segmental lordosis • Disc height
Statistical Analysis
Continuous variables were provided and analyzed as categories. For inter-group comparisons of categorical variables, Pearson χ2 analysis and Fisher’s exact test were employed as appropriate. Odds ratios (OR) and 95% confidence intervals (CI) were calculated for each variable, in terms of its impact on the surgeon’s consideration for radiological spinopelvic parameters.
Any independent surgeon-related variable possibly influencing the consideration of the radiological spinopelvic parameters for the decision-making was included and analyzed using univariate regression by forward entry and retained in the final model when P < .1. Multivariable analyses by binary logistic regression were performed for each isolated radiological parameter, including slippage and angular motion on static and flexion-extension radiographs, segmental lordosis, PI-LL mismatch, SVA, and disc height. Data was exported for analysis into the statistical software program SPSS version 29 for Mac (IBM, Armonk, NY). A two-tailed P-value of <.05 was considered statistically significant.
Results
Characteristics of the Spine Surgeons Included in the Study.
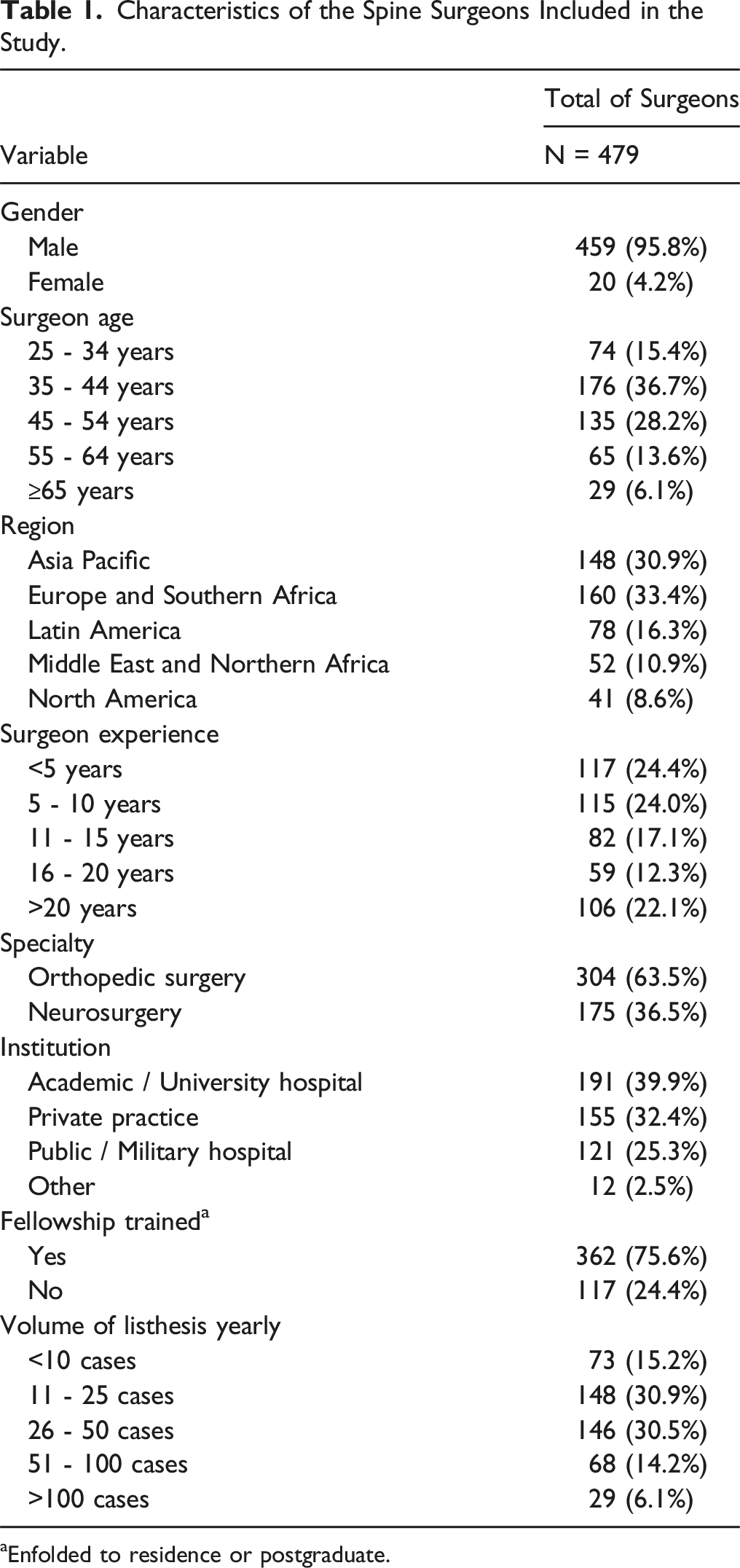
aEnfolded to residence or postgraduate.
Slippage in Static Radiological Exams
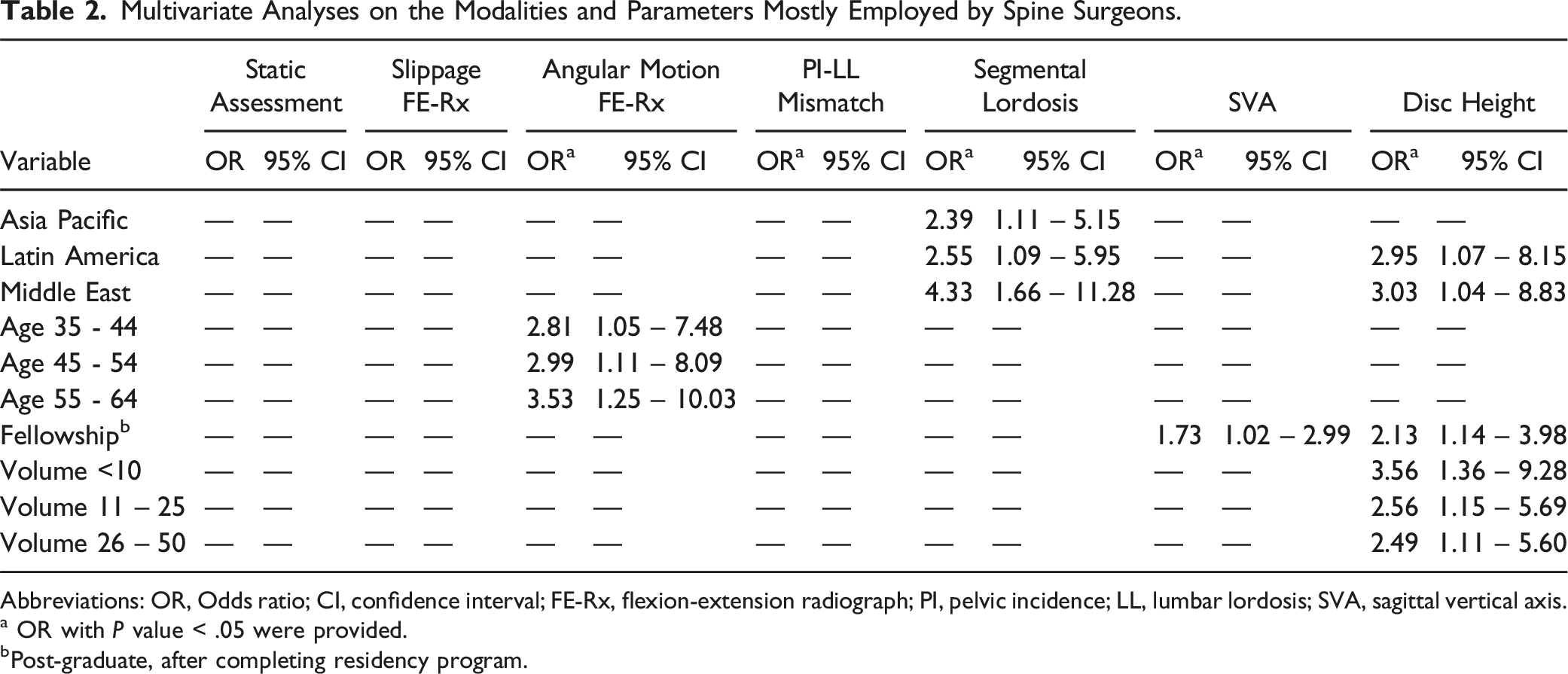
Our study indicates that the absolute displacement of spondylolisthesis on a standing static lateral radiograph is the least important factor considered by surgeons in making decisions about treating degenerative lumbar spondylolisthesis (Figure 1). Upon conducting a multivariate analysis, it was determined that the displacement of spondylolisthesis on a standing static lateral radiograph did not yield significant findings (Table 2). Distribution of the spine surgeons according to radiological modalities and parameters employed (N = 479). Multivariate Analyses on the Modalities and Parameters Mostly Employed by Spine Surgeons. Abbreviations: OR, Odds ratio; CI, confidence interval; FE-Rx, flexion-extension radiograph; PI, pelvic incidence; LL, lumbar lordosis; SVA, sagittal vertical axis. a OR with P value < .05 were provided. bPost-graduate, after completing residency program.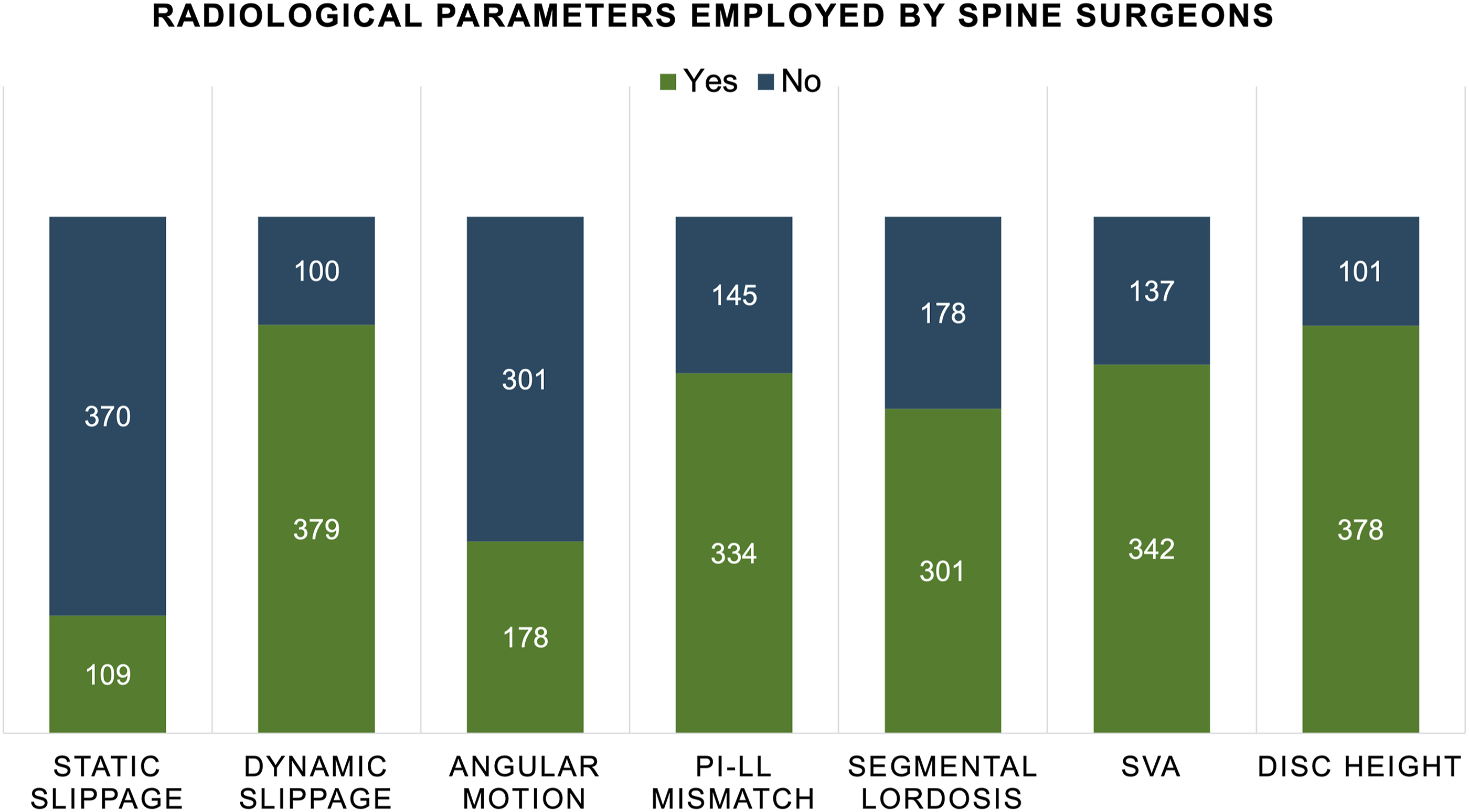
Slippage in Flexion-Extension Radiographs
The most common radiological parameter considered by surgeons for treating lumbar degenerative spondylolisthesis in this study was the motion observed on dynamic flexion-extension X-rays.(79.1%). A difference in vertebral slippage between flexion and extension radiographs of 3 mm was the criteria employed in 35.3% of the surgeons, 2 mm in 14.6%, 4 mm in 14.0%, and 5 mm in 11.1%. However, on multivariate analysis, motion on flexion and extension standing radiographs was not found to be statistically significant (Table 2).
Angular Motion in Flexion-Extension Radiographs
Comparative angular motion in flexion-extension radiographs was considered by 37.2% of the surgeons surveyed in the present study for the treatment of lumbar degenerative spondylolisthsis, but it was the second least frequently considered after static slippage (Figure 1). The criteria utilized for dynamic angular motion consideration was >10 and ≤15 degrees in 17.1%, >5 and ≤10 degrees in 14.8%, and >15 degrees in 4.2% of the surgeons. On multivariate analysis, our study found that surgeons over 35 years old are more likely to consider dynamic angulation as a treatment option. Additionally, there was a trend indicating that the likelihood of considering angular motion to determine treatments increases with the age of the surgeon (surgeon’s aged 35 - 44 years (OR:2.81, 95% CI 1.05-7.48, P = 0.039); 45 - 54 years (2.99, 1.11-8.09, P = 0.030); and age 55 - 64 years (3.53, 1.25-10-03, P = 0.018) (Table 2).
PI-LL Mismatch
Our study revealed that PI-LL mismatch is an important consideration for the treatment of lumbar degenerative spondylolisthesis, with 69.7% of surgeons reporting that PI-LL mismatch affected their treatment decisions. Surgeons in academic/university practice (P = 0.01) and had fellowship training (P = 0.008) were most likely to consider PI-LL mismatch in their decision-making. However, there was no difference between orthopedics and neurosurgery in applying PI-LL mismatch (P = 0.06) in their treatment decisions for lumbar spondylolisthesis. Again, multivariate analysis did not find PI-LL mismatch to be statistically significant (Table 2).
Segmental Lordosis
The segmental lordosis was considered by the 62.8% of the spine surgeons included for deciding on treatment. Interestingly, on multivariate analysis there were regional differences in utilization of this radiographic parameter. Surgeons from the Middle East are most likely to consider segmental lordosis as a treatment criterion (4.33, 1.66-11.28, P = 0.003), followed by surgeons from Asia Pacific (2.39, 1.11-5.15, P = 0.026), and Latin America (2.55, 1.09-5.95, P = 0.030) (Table 2).
Global Sagittal Balance SVA
Our research revealed that global sagittal balance (SVA) is surgeons’ third most commonly used radiographic parameter to determine treatment for lumbar degenerative spondylolisthesis. 71.4% of surgeons consider global sagittal balance as an important treatment parameter, and most of them feel that SVA > 5 cm (35.9%) or SVA > 10 cm (28.8%) are thresholds that influence their decisions. In the univariate analysis, it was found that surgeons who had fellowship training (P = .01) or who worked in academic/university practices (P = .05) were more likely to use global sagittal balance (SVA) in treatment decisions. In the multivariate analysis, fellowship-trained surgeons were found to be associated with a higher likelihood of SVA utilization (1.73, 1.02-2.99, P = .049) (Table 2). On the other hand, there was no difference between orthopedics and neurosurgery in applying global SVA (P = .14) in their treatment decisions.
Disc Height
Disc height was an important radiographic parameter that surgeons considered for treatment of lumbar degenerative spondylolisthesis, and it was the second most important radiological measurement considered by surgeons (78.9%) (Figure 1). On multivariate analysis, consideration of disc height parameter was significantly associated with many different factors. Surgeons from Middle East (3.03, 1.04-8.83, P = .043) and Latin America (2.95, 1.07-8.15, P = .037) are most likely to consider disc height in their treatment of spondylolisthesis. In addition, postgraduate fellowship-trained surgeons also frequently consider disc height (2.13, 1.14-3.98, P = .018). Finally, surgeons who perform less than 50 spondylolisthesis cases per year are more likely to consider disc height in their treatment algorithm: <10 cases (3.56, 1.36-9.28, P = .01), volume 11 – 25 cases (2.56, 1.15-5.69, P = .022), volume 26 – 50 cases (2.49, 1.11-5.60, P = .026) (Table 2).
Discussion
Lumbar degenerative spondylolisthesis is one of the most common indications for surgical treatment for patients with back pain, radiculopathy, and neurogenic claudication. 13 However, there is no consensus on the optimal treatment for this disease due to the high degree of heterogeneity in the patient’s clinical presentation, radiographic features, and options of surgical approaches.14-16 While the goal is to relieve pain to improve patients’ quality of life, there are many options that can achieve that goal, including decompression only, posterior decompression and fusion with or without instrumentation, anterior fusion with indirect decompression or direct posterior decompression, and minimally invasive approaches such as lateral interbody fusion or posterior minimally invasive transforaminal interbody fusions. All those approaches have different abilities to affect local sagittal lordosis that can significantly impact spinopelvic alignment.17,18
In recent years, there has been a greater focus on restoring lumbar lordosis and spinopelvic alignment in lumbar fusions for lumbar degenerative disease to minimize iatrogenic spinal deformity.19,20 Studies have shown that failure to restore lumbar lordosis and spinopelvic balance may lead to post-surgical complications such as pseudoarthrosis, implant failure, adjacent segment diseases, and an increased rate of reoperations. 21 Our current study focuses on understanding what radiographic parameters surgeons consider when they treatment degenerative spondylolisthesis. We are particularly interested if surgeons consider spinopelvic alignment important for the treatment of degenerative spondylolisthesis with the current understanding and education on the importance of spinopelvic alignment in treatment of adult spinal deformity.
Based on 479 responses from surgeons worldwide, observed motion on dynamic flexion-extension X-rays is the single most important radiographic parameter that they consider in the treatment of degenerative lumbar spondylolisthesis, with 79.1% of surgeons utilize it in their clinical evaluations. It’s understandable that motion on dynamic X-rays is the most important factor since it indicates gross segmental instability associated with degenerative spondylolisthesis. One of the most important considerations for surgeons when evaluating degenerative spondylolisthesis patient is to decide to fuse or not to fuse. There are many studies in the published literature that have conflicting evidence that demonstrate the benefits of laminectomy alone over laminectomy with fusion or vice versa.14-18,22,23 However, with evidence of several high-profile historical studies on surgery for degenerative spondylolisthesis that indicates fusion is superior to decompression alone, surgeons are more likely to fuse when there is evidence of gross or obvious instability, such as cases that demonstrate motions on dynamic X-rays.22,23
Our study found that disc height is an important radiographic parameter that surgeons consider when evaluating degenerative spondylolisthesis patients. 78.9% of surgeons in this study utilized disc height in their clinical evaluations, and it is the second most common radiographic parameter that surgeons prefer when evaluating degenerative lumbar spondylolisthesis cases. It’s not absolutely clear why surgeons feel disc height is important in this study, but disc height is an indirect indicator of segmental motion and the risk of iatrogenic instability. When considering whether to fuse or not to fuse in cases of degenerative spondylolisthesis, the presence of collapsed disc height is less likely to be associated with segmental motion and risk of iatrogenic instability. 24 On the other hand, tall and preserved disc height indicated preserved local mobility and risk of iatrogenic instability after decompression alone. 24
While global sagittal alignment and spinopelvic alignment are not the most common radiographic parameters used by surgeons in the evaluation and treatment of lumbar degenerative spondylolisthesis, our study found that the majority of surgeons believe that global sagittal balance SVA and PI-LL mismatch are important radiographic parameters to consider in this condition. 71.4% of surgeons use global sagittal balance SVA, and 69.7% of surgeons use PI-LL mismatch in their evaluation of lumbar degenerative spondylolisthesis. Research and clinical studies over the past decades indicates increased risks of failed surgery, complications, and re-operations in adult spinal deformity surgery. 21 Similar concerns are shared among many surgeons in the treatment of lumbar degenerative diseases when there are global sagittal malalignment and PI-LL mismatches after fusion surgeries. Much of these concerns remain in academic debates in conferences and education programs without concrete or class I scientific evidence.3,23,24 Thus, it’s not surprising that our studies find that surgeons in academic/university-affiliated practices and fellowship trained are most likely to apply global sagittal balance SVA and PI-LL mismatch in their evaluation of lumbar degenerative spondylolisthesis patients. However, there was no observed difference between orthopedics and neurosurgery surgeons in applying PI-LL mismatch for treatment of lumbar degenerative spondylolisthesis.
Morse et al 25 in their survey across the members of the Lumbar Spine Research Society and Society of Minimally Invasive Spine Surgery found the most common radiographic parameter that affected the decision to fuse patients with degenerative spondylolisthesis included instability, grade of spondylolisthesis and laterolisthesis. The current also found parameters such as instability noted through movement on dynamic radiographs to be a significant factor that determined the decision to fuse or not. Further, the study also found disc height and global sagittal balance as additional factors that affected the management decision of the surgeons.
One of the intent for our research is to study and understand the geographical differences among surgeons around the world in the surgical evaluation of degenerative lumbar spondylolisthesis. The study did not identify any significant differences in the use of degree of slip on lateral static X-rays, degree of slips on flexion-extension dynamic X-rays, angular motion on flexion-extension dynamic, global sagittal SVA, and PI-LL mismatch. However, our study found significant regional differences in surgeons with the use of disc height and segmental lordosis when evaluating degenerative lumbar spondylolisthesis patients. Surgeons from the Middle East and Latin America were the most likely to apply disc height and segmental lordosis in their surgical evaluations of patients with lumbar degenerative spondylolisthesis. Additionally, Surgeons from the Asia Pacific also consider segmental lordosis an important radiographic parameter to consider in the treatment of lumbar degenerative spondylolisthesis.
Limitations
This study has several limitations. Firstly, the responsive rate was relatively low, considering the survey was distributed to 6000 AO Spine members, receiving responses from less than 500 members. A second limtations of the present study was the fact than the open questions regarding radiographic and spinopelvic parameters were not combined with clinical considerations for the decision-making. Other limitation is there were not assessed the most conventional radiological characteristics of the static radiological exams, such as foraminal area and height, and spinal canal area or diameter. Finally, for these questions with regard to radiological parameters important factors as bone mineral density and degree of vertebral anquilosis were not considered, being a well-known factor affecting the outcome and the rate of complications of the surgical treatment in spondylolisthesis, and therefore influencing the decision-making in a real-life scenario.
Conclusions
Treatment of degenerative lumbar spondylolisthesis among surgeons worldwide is influenced by several radiographic parameters, including slippage on dynamic radiographs, disc height, global alignment, and PI-LL mismatch. Surgeons’ age and Region, fellowship-trained, and volume of treated cases yearly were significantly associated with these radiological parameters in their decision-making. Additionally, while this degree of slip on dynamic X-rays was the most crucial radiographic parameter considered by surgeons around the world, the majority of surgeons, particularly those that are in academic/university practices and fellowship-trained, feel that global sagittal SVA and PI-LL mismatch are also critical parameters to consider in the treatment of lumbar degenerative spondylolisthesis.
Footnotes
Acknowledgments
This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international spine degeneration experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international spine degeneration experts.