
Abstract
Purpose:
This study aimed to analyze the effect of the thoracic anteroposterior diameter (TAPD) and pelvic anteroposterior diameter (PAPD) on global sagittal alignment in asymptomatic patients with normal sagittal alignment.
Patient sample:
The study investigated 2042 adult patients who initially presented at our hospital with a hip and knee problem without history of symptoms related to the entire spine. Only 57 patients with normal global sagittal alignment (C2–7 sagittal vertical axis (SVA) and C7–S1 SVA of <10 mm) were considered.
Methods:
The whole-spine standing lateral radiographs were obtained to analyze the following parameters: pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), lumbar lordosis (LL), thoracic inlet angle (TIA), T1 slope, cervical spinal parameters (angle of C0–2, C2–7, and C0–7), TAPD, and PAPD. Statistical analysis was performed using Pearson correlation coefficients and multiple regression analyses.
Results:
All the parameters showed a normal distribution. TAPD had a significant relationship with thoracic kyphosis (TK; r = 0.458), TIA (r = 0.677), and C0–2 angle (r = 0.294) but no significant relationship with T1 slope and other cervical parameters. PAPD had a significant relationship with PI (r = 0.309) and PT (r = 0.463) but no significant relationship with LL, SS, and TK. The multiple regression analysis showed that TIA = 21.974 + 0.405 (TK) + 0.188 (TAPD) (p < 0.0001).
Conclusions:
TAPD and PAPD are associated with TIA, TK, C0–2 angle, PI, and PT, all of which act as key factors in spinal sagittal alignment. Although they did not directly correlate with other cervical parameters, T1 slope, and LL, TAPD and PAPD might have indirect effects on cervical and lumbar spinal sagittal alignment through their relationships with TIA, TK, and PI.
Keywords
Introduction
Proper sagittal alignment of the body is essential for minimizing energy consumption in the upright position. 1 –4 Many studies have suggested that the relationships among pelvic incidence (PI), lumbar lordosis (LL), and thoracic kyphosis (TK) are important for maintaining sagittal alignment. 2 –8 Cervical lordosis (CL), which is another relevant parameter, is reported to be affected by TK, the T1 slope, and thoracic inlet alignment (TIA). 8 –13 Normal physiological spinal sagittal alignment is maintained by the interactions among these parameters. However, correlations among the parameters are not yet fully known, and additional parameters, not yet defined, may also influence spinal alignment.
In a normal sagittal alignment, a line of gravity bisects the weight of the body anteroposteriorly. 1 –4,13 Therefore, the anteroposterior diameter of the thoracic and pelvic regions would be expected to affect sagittal alignment (Figure 1). However, most studies to date have been based on angles, rather than diameters, and knowledge of the effect of the anteroposterior diameter of the body on spinal alignment is limited.

Expected correlation between the line of gravity and anteroposterior thoracic cage weight. (a) Normal thoracic cage and TK, A ≒ B; (b) large thoracic cage with small TK, C > D; and (c) large thoracic cage and TK, E ≒ F. (a) and (c) are considered balanced but (b) is considered unbalanced. TK: thoracic kyphosis.
Materials and methods
Materials
The study participants were selected from among the 2042 adult patients who initially presented at our hospital’s orthopedic department between January 2017 and March 2018 for the evaluation of hip and knee problems. Those who consented underwent a whole-body radiography for assessing sagittal alignment possibly related to hip or knee alignment. Among them, patients who were found to have factors that could affect the spinal sagittal alignment, such as scoliosis, degenerative spondylosis, spondylolisthesis, spondylolysis, fracture, and Scheuermann’s kyphosis, were excluded.
The sagittal vertical axis (SVA) was measured to identify the sagittal alignment. The minimum distance between the C2 plumb line (vertical line from the C2 odontoid tip) and the C7 plumb line (vertical line from the center of the C7 body) was defined as the C2–7 SVA. The minimum distance between the C7 plumb line and a vertical line from the posterosuperior corner of the S1 body was defined as the C7–S1 SVA. The SVA changes with aging, making it difficult to obtain an accurate standard normative value. We defined normal sagittal alignment as both C2–7 SVA and C7–S1 SVA within 10 mm; 62 patients met this criterion. After exclusion of the patients with spinal symptoms or disease, 57 adults with normal spinal sagittal alignment aged 20–68 years were enrolled (mean C2–7 SVA 1.50 ± 5.11 mm, range −9.61 to +9.44 mm; mean C7–S1 SVA 2.18 ± 5.11 mm, range −9.33 to +9.98 mm). The male-to-female sex ratio was 21:36, and the mean age was 47.12 ± 14.55 years (8 patients were in their 20s, 10 in their 30s, 9 in their 40s, 18 in their 50s, and 12 in their 60s). The mean body mass index (BMI) was 23.2 ± 4.1 kg/m2 (range 17.8–30.4 kg/m2).
Whole-spine standing lateral radiographs were obtained using the EOS™ system (formerly Biospace Med, Paris, France). The patients were placed in the relaxed upright standing position with shoulder forward flexion and elbow flexion to bring the fingertips in front of both shoulder joints. Their heads were faced forward with a horizontal gaze parallel to the Frankfort horizontal plane (the extended line connecting the lower border of the orbit and the external auditory meatus). 14 The study was approved by the Institutional Review Board of Kyungpook National University Hospital (IRB protocol number KNUH 2018-07-012).
Simple radiograph analysis
Spinopelvic parameters
The PI was defined as the angle between the line connecting the midpoint of the two hip joint centers to the midpoint of the sacral end plate and the line perpendicular to the center of the sacral end plate, and this is a morphological parameter that does not change with posture. The sacral slope (SS) was defined as the angle between the horizontal line and the sacral end plate. The pelvic tilt (PT) was defined as the angle between the vertical line from the midpoint of the two hip joint centers and the line connecting the midpoint of the two hip joint centers to the midpoint of the sacral end plate. The LL angle was defined as the angle between the sacral end plate and the upper end plate of L1. The TK angle was defined as the angle between the upper end plate of T1 (T1UEP) and the lower endplate of T12, by the Cobb method (Figure 2 and Table 1).

Spinopelvic parameters. TK: thoracic kyphosis; PT: pelvic tilt; PI: pelvic incidence; SS: sacral slope; LL: lumbar lordosis.
Classification of the “morphological parameters” and “orientation parameters”.

CL: cervical lordosis; TAPD: thoracic anteroposterior diameter; TIA: thoracic inlet angle; TK: thoracic kyphosis; PAPD: pelvic anteroposterior diameter; SS: sacral slope; PI: pelvic incidence; LL: lumbar lordosis.
Cervical spinal parameters
CL, an orientation parameter that can change with posture, is generally divided into three major categories: C0–7 angle, C0–2 angle, and C2–7 angle (Figure 3, right). The C0–7 angle was measured as the angle between the McRae line and the lower end plate of C7. The C0–2 angle was measured as the angle between the McRae line and the lower end plate of C2. The C2–7 angle was measured as the angle between the lines extending from the posterior cortex of the C2 body and posterior cortex of the C7 body.
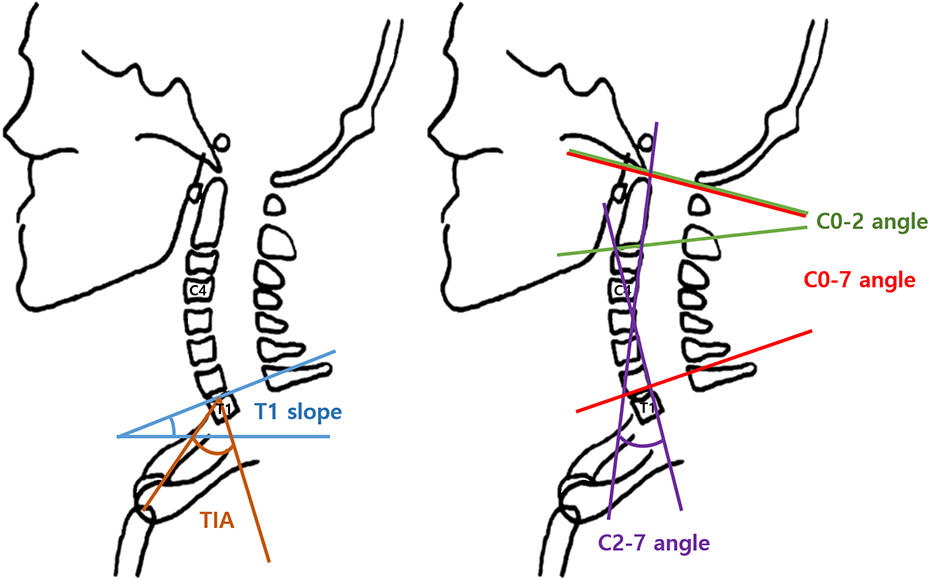
Schematic diagram of the upper thoracic (left) and cervical (right) spinal parameters. TIA: thoracic inlet alignment.
Proximal thoracic parameters
The TIA was defined as the angle between the perpendicular line drawn from the center of the T1UEP and the line connecting the upper end of the sternum to the center of the T1UEP; it is a morphological parameter that does not change with posture. The T1 slope, an orientation parameter that can change according to posture, was defined as the angle between the T1UEP and the horizontal plane (Figure 3, left).
Thoracic and pelvic anteroposterior diameters
The thoracic anteroposterior diameter (TAPD) was defined as the minimum distance from the posterior cortex of the 10th thoracic vertebral body to the most prominent anterior margin of the xiphisternal joint of sternum, measured from the lateral side. The pelvic anteroposterior diameter (PAPD) was defined as the minimum distance between the vertical line at the midpoint between the anterosuperior iliac spines and the vertical line at the superoposterior corner of the S1 body. TAPD and PAPD were classified as morphological parameters (Figure 4).

Measurement of the TAPD and PAPD. TAPD: thoracic anteroposterior diameter; PAPD: pelvic anteroposterior diameter.
Statistical analysis
The Picture Archiving and Communication System (π view; Infinitt, Seoul, Korea) was used by two independent observers to perform the measurements. To test inter- and intraobserver reliabilities, TAPD and PAPD were measured three times at an interval of more than 2 weeks by two orthopedic practitioners. Inter- and intraobserver intraclass correlation coefficients (ICCs) were calculated using the mean of each observer’s measurements. Linear regression models were obtained using the Pearson correlation coefficient and simple linear regression analysis. The statistical analysis was performed with the SPSS 17.0 (Chicago, IL, USA); a p value of <0.05 was considered significant.
Results
Descriptive statistics
For TAPD and PAPD measurement, the interobserver ICCs were 0.814 (95% confidence interval 0.61–0.93) and 0.801 (95% confidence interval 0.59–0.91), and the mean intraobserver ICCs were 0.861 (0.82, 0.843, and 0.921) and 0.848 (0.84, 0.812, and 0.894), demonstrating excellent intra- and interobserver agreement, respectively (Figure 5).

Distribution of the parameters. (a) PT, (b) PI, (c) PAPD, (d) TK, (e) TAPD, and (f) TIA. PT: pelvic tilt; PI: pelvic incidence; PAPD: pelvic anteroposterior diameter; TK: thoracic kyphosis; TAPD: thoracic anteroposterior diameter; TIA: thoracic inlet angle.
Spinopelvic parameters
The mean PI, SS, LL, and TK were 49.11° ± 9.91°, 35.48° ± 7.90°, 49.69° ± 9.87°, and 35.36° ± 9.35°, respectively.
TAPD and PAPD
The mean TAPD and PAPD were 131.46 ± 19.14 mm (range 93.43–169.61 mm) and 83.65 ± 11.62 mm (range 29.08–106.33 mm), respectively, and both parameters showed a normal distribution.
TAPD showed significant correlations with TIA, TK, and C0–2 angle: the correlation coefficients were 0.6777 (p < 0.0001), 0.458 (p = 0.0003), and 0.294 (0.026), respectively. There was no significant correlation with the T1 slope and other cervical spinal parameters (C0–7 angle and C2–7 angle) (Figure 6 and Table 2). PAPD showed significant correlations with the pelvic tilt (PT) and PI: the correlation coefficients were 0.463 (p = 0.0002) and 0.309 (p = 0.0191), respectively. TAPD and PAPD did significantly correlate with LL, SS, and the cervical and thoracic spinal parameters (Table 3). BMI showed significant correlation with TAPD (r = 0.671; p < 0.0001), but not with PAPD (r = 0.04; p = 0.770).

Relationship of TAPD to other upper spinal parameters. TAPD: thoracic anteroposterior diameter.
Pearson correlation coefficients and p values of the parameters for TAPD.
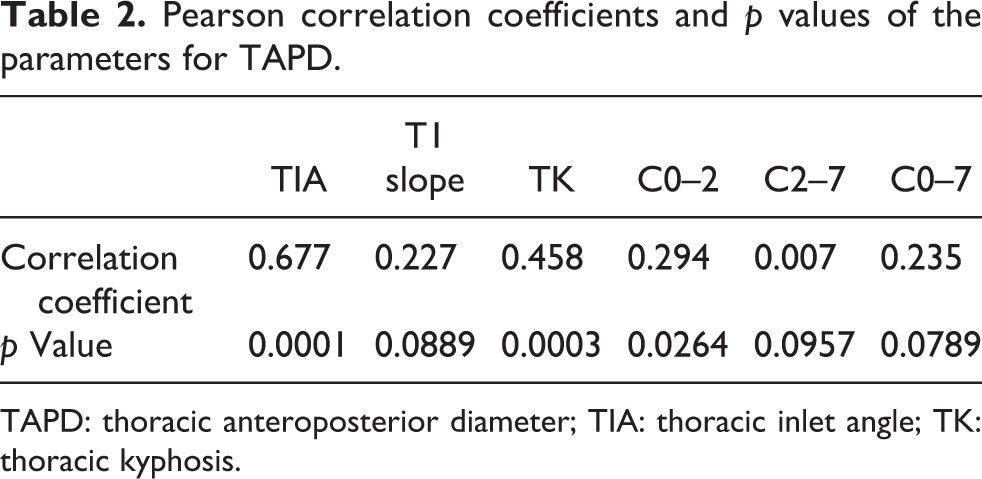
TAPD: thoracic anteroposterior diameter; TIA: thoracic inlet angle; TK: thoracic kyphosis.
Pearson correlation coefficients and p values of the parameters for PAPD.

PAPD: pelvic anteroposterior diameter; PT: pelvic tilt; PI: pelvic incidence; SS: sacral slope; LL: lumbar lordosis; TK: thoracic kyphosis; TIA: thoracic inlet angle.
The relationship between the TAPD and the TIA can be expressed by the results of a simple linear regression analysis (i.e. R 2 = 0.458; p < 0.0001) and TIA = 0.279 × TAPD + 24.389. TAPD also significantly correlated with TK (p = 0.0003). The relationship between the TAPD and the TK can be expressed by the results of the simple linear regression analysis (i.e. R 2 = 0.21; p = 0.0003) and TK = 0.224 × TAPD + 5.969. The multiple linear regression analysis showed that TIA = 21.974 + 0.405 (TK) + 0.188 (TAPD) (p < 0.0001). A large TAPD indicated that the thoracic cage was large; when this is observed in individuals, TK and TIA may also be large.
Discussion
Many studies have analyzed the effect of spinal sagittal parameters on sagittal alignment; however, few studies 15,16 have investigated the effect of the diameters of the thoracic cage and pelvis on sagittal alignment. Also, direct relationships between the lumbar spinal parameters and the thoracic and cervical spinal parameters remain incompletely characterized, and the thoracic and cervical spine may be affected by parameters that are yet to be elucidated. According to Hardacker et al. 9 , TK is associated with CL; many other investigators have reported that TK is associated with PI or LL. 2,3,5,6,11,17 –20 Although TIA reportedly affects TK, 8 data on the degree of physiological TK in individuals are lacking, and as of yet unreported factors also may affect TK.
In this study, the relationship between the TAPD and the TIA, both considered morphological parameters, was significant (p < 0.0001). If TAPD is large, the C0–2 angle of the upper cervical spine tends to be larger. However, in this study, TAPD was not associated with the T1 slope and most of the cervical spinal parameters. Nonetheless, TAPD was related to the TIA and TK, which are related to the T1 slope and cervical spinal parameters. Further studies of the correlation between TAPD and TIA are warranted.
PAPD showed a significant correlation with the PI (p = 0.0191), both parameters are classified as morphological parameters. PAPD also significantly correlated with PT (p = 0.0002) but not with SS (p = 0.7055). In other words, as the pelvic diameter increases, PI also increases without a change in SS in the nonpathological setting (Figure 7), seemingly moving the hip joint center forward. This forward movement of the hip joint increases the PT, and the line of gravity also changes in the nonpathological setting. In contrast, PAPD did not correlate with the parameters associated with LL and the cervical and thoracic spines. However, since PI was related to LL, and LL was related to TK, an additional relationship between the PAPD and the upper spinal parameters is likely to exist.

Relationship of PAPD to the pelvic incidence and tilt. PAPD: pelvic anteroposterior diameter.
Spinopelvic balance is known to be related to pain, disabilities, thoracolumbar deformities, and degenerative conditions. 17,21 –24 The results of this study suggest that PAPD and TAPD may affect PI, TK, and TIA and can be used as the reference index for global spinal sagittal alignment. Further, TAPD showed significant correlation with BMI, which can change according to increases or decreases in the body weight. This finding suggests that the line of gravity may change according to the body weight.
This study has several limitations. First, the age and sex distributions of the patients included in this study were uneven. Age and sex may affect sagittal sacropelvic morphology in asymptomatic individuals. 25 We studied only patients whose sagittal alignment was estimated to be normal; elderly patients with age-related degenerative changes and younger adults who were less likely to visit hospitals were underrepresented. Also, we cannot conclude that the study cohort was normative, given its small size (limited to 57 participants). Future studies involving control groups matched for additional factors, such as age and sex, are needed to expand on the results of this study. Second, the participants were patients who visited the hospital for hip and knee problems. Pathology at those sites would likely affect the overall spinal alignment. Third, we included only subjects who had normal sagittal alignment; it is possible that the same parameters measured in patients with abnormal spinal alignment would show different correlations. Fourth, the measured TAPD and PAPD may vary depending on the individual’s height, and we did not calibrate this difference; further research is needed in this area. Fifth, because TAPD and PAPD are lengths, rather than angles, unlike the other parameters, there is a possibility of introducing various errors depending on the distance between the tube and the detector, according to the radiographic technique. To compensate for this and reduce error, we used the EOS system; however, if the same method is not used in other studies, the results will not be comparable. Finally, it has been reported that the position of the upper limb can affect the spinal sagittal alignment. 26 In this study, we selected the position in which the hand is placed on the shoulder to include the cervical and lumbar spine in one radiograph, which may have introduced error in the resulting alignment. Nevertheless, the results of this study indicate that when planning the surgical correction of sagittal alignment is affected by trauma or degenerative changes, practitioners should keep in mind that the physiological sagittal alignment of individuals may differ according to TAPD or PAPD.
Conclusions
The study results show that TAPD and PAPD are associated with the TIA, TK, C0–2 angle, PI, and PT, which all act as key factors in spinal sagittal alignment. Although they did not directly correlate with the other cervical spinal parameters, T1 slope, and LL, TAPD and PAPD might have indirect effects on the cervical and lumbar spinal sagittal alignment through their relationships with TIA, TK, and PI. In other words, TAPD and PAPD may influence the physiological alignment of the lumbar or cervical spine. As expected, PI was strongly related to the normal value of LL. TAPD and PAPD can be used as a reference for estimating the normal parameter values of global sagittal alignment and may provide useful data for further studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.