
Abstract
Aim
The aim of this study was to investigate whether or not spinopelvic parameters alone affect the mechanism of formation and type of hip fracture. A secondary aim was to examine the impact on the formation mechanism of many factors that have been previously determined in the epidemiology of hip fractures.
Material and Method
The data of 200 patients who presented because of a hip fracture were retrospectively examined. The data included age, gender, body mass index, affected side and Singh Index (SI), and the measurements taken on radiographs of pelvic incidence, pelvic tilt, sacral slope, and lumbar lordosis values. The hip fractures were categorised into two groups: femoral neck and pertrochanteric.
Results
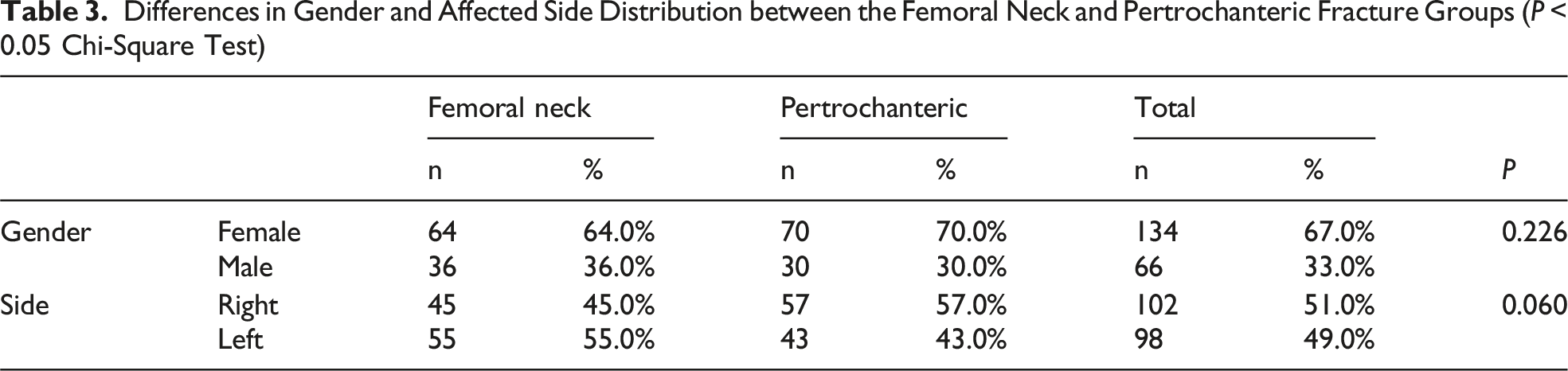
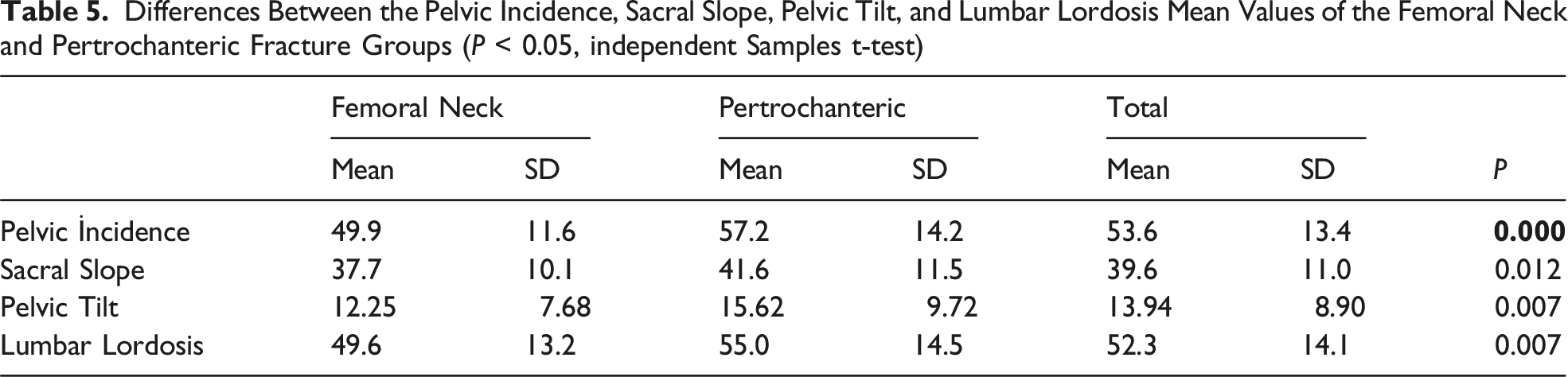
The 100 patients in Group 1 (femoral neck) comprised 64 females and 36 males with a mean age of 75.4 ± 10.9 years, and the 100 patients in Group 2 (pertrochanteric) comprised 70 females and 30 males with a mean age of 77.6 ± 11.1 years. In Group 1, the mean values measured were pelvic incidence: 49.9 ± 11.6, pelvic tilt: 12.25 ± 7.68, sacral slope: 37.7 ± 10.1, and lumbar lordosis: 49.6 ± 13.2. In Group 2, these values were pelvic incidence: 57.2 ± 14.2, pelvic tilt: 15.62 ± 9.72, sacral slope: 41.6 ± 11.5, and lumbar lordosis: 55 ± 14.5. These values were statistically significantly higher in the pertrochanteric group than in the femoral neck group (P < 0.05).
Conclusion
This study demonstrated that pelvic incidence and related spinopelvic parameters are associated with hip fracture morphology. Patients with pertrochanteric fractures had significantly higher pelvic parameter values compared with those with femoral neck fractures, suggesting that increased pelvic incidence may predispose to pertrochanteric fractures.
Background
Hip fractures not only represent an important and emergency health problem in the elderly population, but as a cause of significant morbidity and mortality in this population also cause high healthcare costs.1,2 The frequency of hip fractures increases with an ageing population, and it has been emphasised that it is necessary to increase awareness and undertake comprehensive research to determine biomechanical and anatomic markers of the causes of fractures.
Although hip fractures generally occur as a result of low-energy trauma such as a fall from standing, the region where they occur, classification, and whether they are femoral neck or pertrochanteric can be significantly affected by many individual anatomic differences, including the sagittal spinopelvic alignment. 3
Many spinal disorders are affected by the relationship between the spine and pelvis alignment. The effect of changes in this relationship on hip pathologies and surgeries has been reported in the literature. The range of movement of the spine decreases with ageing and this increases the weight-bearing and dependence on the hip in simple daily activities such as sitting, standing up, and walking. 4
The spinopelvic parameters of pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), and lumbar lordosis (LL) are crucial for achieving general sagittal alignment and body posture. Spinopelvic parameters are an important indicator of the complex relationship and interaction between pelvic and spinal morphological and anatomic structures and the functional postures of these. 5 Of the spinopelvic parameters, PI is accepted as a fixed morphological factor that does not change with a change in position. In contrast, PT, SS, and LL are accepted as dynamic parameters that can be affected by changes in body position. 6
Although previous studies have comprehensively researched the role of spinopelvic parameters on various spinal pathologies and on the results of total hip arthroplasty, the effects on the biomechanics of fracture formation and the type of hip fracture have not been sufficiently researched and determined. Therefore, the primary aim of this study was to investigate the relationship between spinopelvic parameters and hip fracture type, separating the fractures into femoral neck fractures and pertrochanteric region fractures. A secondary aim was to investigate whether or not there were any effects or associations of patient-related factors such as age, BMI (Body Mass Index), and bone quality evaluated with the Singh Index, with these spinopelvic parameters or fracture types. A deeper understanding of these relationships will make a significant contribution to determining the risk factors in the population at high risk of hip fracture, and enable the necessary precautions to be taken and more effective preoperative planning to be made.
Material and Method
This retrospective, observational study was approved by the Institutional Review Board (decision no: 05/04/2022-3498) and was conducted in compliance with the ethical principles of the Helsinki Declaration. The data of a total of 372 patients who presented with hip fractures at the Emergency Department of SBU Şişli Hamidiye Training and Research Hospital between September 2017 and January 2022 were examined. All patients provided written informed consent before participation in the study.
Patients older than 50 years who sustained low-energy trauma, such as a fall from standing height, and had a body mass index (BMI) below 35, were included. All participants had pelvis anteroposterior and lumbosacral lateral radiographs of adequate diagnostic quality and no history of hip or spinal disease, surgery, or rheumatologic disorders. Patients with adjacent joint contracture or muscle weakness were excluded to avoid factors that could influence spinopelvic alignment. Exclusion criteria also covered cases with missing or poor-quality radiographs, high-energy trauma, obesity (BMI ≥35), rheumatologic disease, or any previous hip or spinal pathology or surgery. Of the initial 372 patients, 93 did not have appropriate radiographs, 24 had fractures resulting from high-energy trauma, 9 were obese, and 5 had rheumatological disease. From the remaining 241 (107 femoral neck, 134 pertrochanteric), 200 patients were included in the study. These patients had experienced low-energy trauma, were aged >50 years with BMI <35, had appropriate pelvis anteroposterior and lumbosacral lateral radiographs, had no history of hip and spinal disease or surgery, no rheumatological disease, and no adjacent joint contracture muscle weakness. The first 100 patients in each fracture group were then selected according to their chronological order of presentation date, and were selected for each of the fracture types. The other patients were excluded from the study.
The hip fractures in this study were examined in two groups: femoral neck fractures and pertrochanteric region fractures. This grouping was categorised radiographically. The primary outcome measure of this study was the type of hip fracture (pertrochanteric or femoral neck), which was analysed in relation to spinopelvic parameters.
The patients in the two groups were compared in terms of demographic data, including age, gender, height, weight, BMI, and the fracture side and SI. The fractures were classified according to the Arbeitsgemeinschaft für Osteosynthesefragen (AO) classification, as it includes both femoral neck and pertrochanteric hip fractures and is accepted as universal and detailed. 7 The SI, which is used in the diagnosis of osteoporosis on anterior-posterior radiographs, is a semi-quantitative evaluation method, based on the bone trabecular network selected on proximal femur radiographs, which divides osteoporosis into 6 grades. 8 The age groups were determined according to the World Health Organisation classification as follows: 45-59 years as middle age, 60-74 years as early elderly, 75-89 years as late elderly and ≥90 years as very late elderly. BMI was evaluated as low:<18.9, normal: 19-24, overweight:25-29.9, obese:30-35, and morbidly obese: >35.9,10
Pelvic incidence (PI), which was first defined by Lageya in 1998, is an anatomic and morphological measurement proportional to other parameters. Therefore, it is accepted as unchanging.
11
In a study by Soo-An Park et al, it was shown that the PI value of a patient does not change on radiographs taken standing or supine.
12
Therefore, as standing lateral radiographs cannot be taken of patients with hip fractures for the measurement of spinopelvic parameters, lumbosacral lateral radiographs were taken with the patient positioned supine, hips and knees in extension, and the x-ray placed to be perpendicular to the lateral side of the patient, included in 30 × 90 cm cassettes. As PI is a fixed value, it was decided that PI would be the primary variable in this study. Care was taken for both femoral heads to overlap on this radiograph. On radiographs where this view could not be obtained, this point was defined as the midpoint of the line joining the centres of both femoral heads. Attention was also paid to this radiograph for complete visualisation of the sacrum, visualisation as far as T12 in the proximal, for disc spaces to be evident, both iliac wings to be superimposed on each other, and the sciatic notches to overlap (Figure 1). Lumbosacral AP and pelvis lateral radiographs (showing PI, PT, SS, LL measurements)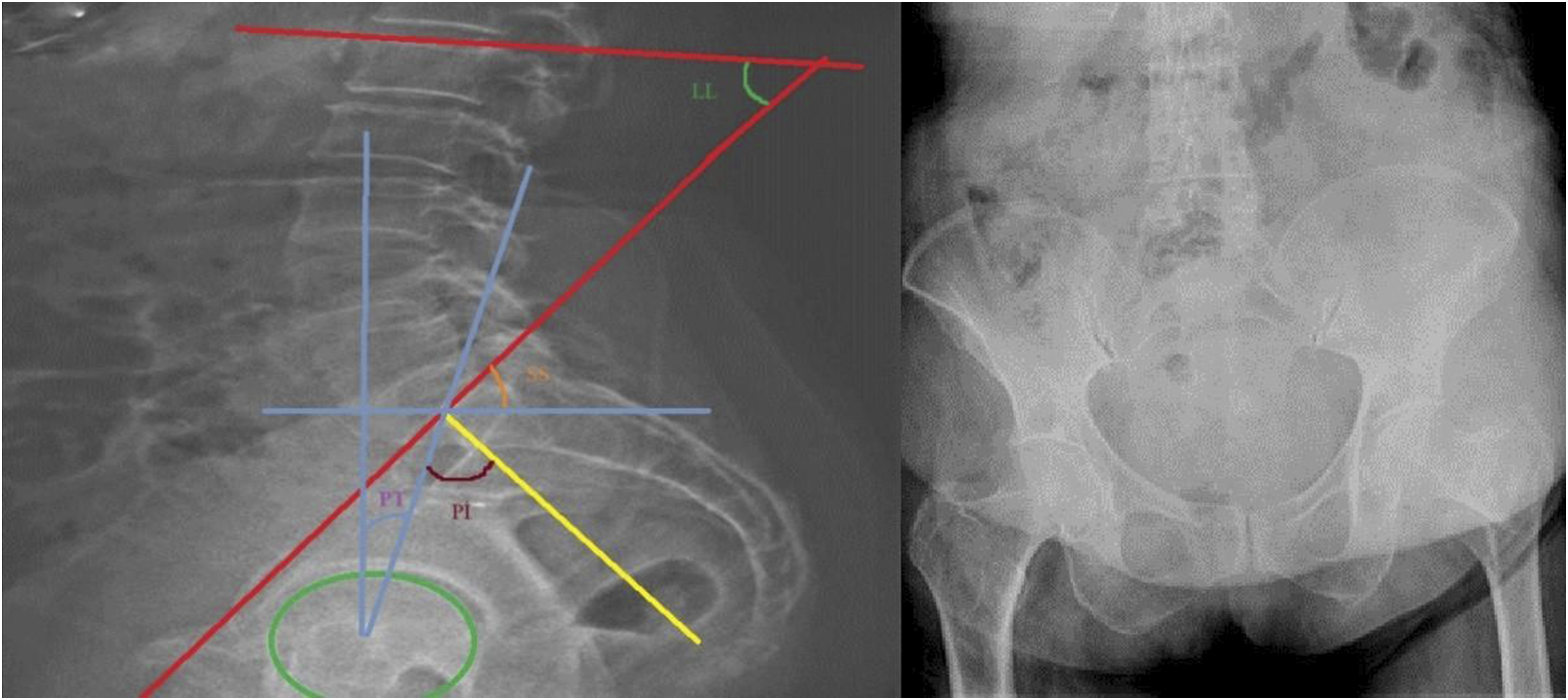
The pelvis AP (anteroposterior) radiograph was taken with the patient positioned supine with the hips and knees in extension, both legs in 15° internal rotation, and the x-ray perpendicular to the patient. The image was accepted when showing T12 vertebra in the proximal, 5 cm below the femur trochanter minor in the distal, and all of the iliac wing in the lateral. When these criteria were not met, the images were excluded from the evaluation as correct measurement would be prevented.
The parameters examined on appropriate radiographs were as follows: Pelvic incidence (PI), as the angle between the line drawn to the midpoint of the promontorium from the centre of the line joining the femoral head centres and the vertical line drawn to the midpoint of the line joining the anterior and posterior points of the promontorium. Pelvic tilt (PT) as the angle between the line drawn to the upper midpoint of the promontorium from the midpoint of the line joining the femoral head centres, and the line drawn from the femoral head centre in the vertical plane to the horizontal plane. Sacral slope (SS) as the angle between the line drawn parallel to the horizontal plane and the line joining the anterior and posterior promontorium. Lumbar lordosis (LL) as the angle between the lines drawn to the lumbar 1st upper endplate and the sacral 1st upper endplate.
The Intraclass Correlation Coefficient (ICC) was calculated to assess the inter-rater reliability among the three evaluators within the study groups

The demographic characteristics, BMI, SI, and the relationship between these, and whether or not there was a significant difference between the two groups in the measured spinopelvic parameters, and relationships with other parameters were investigated.
Statistical Analysis
Data obtained in the study were analysed statistically using SPSS version 20 software (SPSS Inc., Chicago, IL, USA). Conformity of the data to normal distribution was assessed with the Kolmogorov-Smirnov test. A significant difference between the mean values of groups of quantitative data showing normal distribution was examined with the t-test in independent groups and with One-Way Analysis of Variance. Relationships between categorical variables were examined with Chi-square analysis and the Kruskal-Wallis test. A multiple linear regression analysis was performed to determine which factors independently predicted the type of fracture. Age, sex, body mass index, Singh Index, pelvic incidence, sacral slope, and lumbar lordosis were included as independent variables. In all the analyses, a value of P < 0.05 was accepted as statistically significant.
Demographic Data
Differences in the Age and BMI Values Between the Femoral Neck and Pertrochanteric Fracture Groups (P < 0.05 independent t-test)

Differences in Gender and Affected Side Distribution between the Femoral Neck and Pertrochanteric Fracture Groups (P < 0.05 Chi-Square Test)
Results
Radiological Measurement Results
In the multiple linear regression model, fracture type (coded as 1 = intertrochanteric 2 = femoral neck) was analysed as the dependent variable. The overall model was statistically significant (F = 3.55, P = 0.001), explaining 11.5% of the variance in fracture type(R2 = 0.115).
Multiple Linear Regression Analysis of Factors Associated with Fracture Type (R2 = 0.115 F = 3.55 P < 0.001)

Differences Between the Pelvic Incidence, Sacral Slope, Pelvic Tilt, and Lumbar Lordosis Mean Values of the Femoral Neck and Pertrochanteric Fracture Groups (P < 0.05, independent Samples t-test)
Differences Between the Pelvic Incidence, Pelvic Tilt, Sacral Slope, and Lumbar Lordosis Values According to Age in the Femoral Neck and Pertrochanteric Fracture Groups (P > 0.05 kruskal-wallis Test)

Differences Between the Pelvic Tilt, Pelvic Incidence, Sacral Slope, and Lumbar Lordosis Values According to BMI in the Femoral Neck and Pertrochanteric Fracture Groups (*P > 0.05 one-way variance analysis)

Differences Between the Femoral Neck and Pertrochanteric Fracture Groups in Respect of the Singh Index (*P > 0.05 chi-square Test)

Differences Between the pelvic Incidence, Sacral Slope, pelvic Tilt, and Lumbar Lordosis Mean Values According to the AO Classification of the Femoral Neck and Pertrochanteric Fractures Separately in Each Group (*P > 0.05 Kruskal-Wallis Test)

Discussion
This study investigated the relationship between the spinopelvic alignment and parameters, and hip fracture types, and focused in particular on the comparisons of femoral neck and pertrochanteric fractures. The primary finding was that Pİ, PT, SS, and LL measurements were significantly higher in patients with pertrochanteric fractures than those with femoral neck fractures. These findings suggest that sagittal pelvic morphology could play a role in the mechanisms leading to different fracture types. While spinopelvic parameters such as PI, PT and SS play an essential role in hip-spine biomechanics, their
High pelvic incidence, which is accepted as a fixed anatomic characteristic, has been previously associated with the formation of hip and spine degenerative conditions and with the progression of pathologies. 15 Consistent with this association, the current study results showed that patients with high PI measurements were more predisposed to have pertrochanteric fractures. This confirmed the results reported by Kwon et al that in patients with a high PI, there was an increased risk of femoral head collapse in osteonecrosis cases with no traumatic cause. The mean PI value of the current study patients with pertrochanteric fracture exceeded 55°, which was accepted as the clinically significant threshold value in the study by Kwon. 16 Although the present study focused on fracture morphology rather than osteonecrosis, these data reinforce the biomechanical concept that higher Pİ values may alter hip joint loading and stress distribution, potentially contributing to fracture pattern differences.
The biomechanical interaction between increased PI and pertrochanteric fractures can be explained through analyses of how PI and loading models affect sagittal alignment in the proximal femur. 17 Increased PI is strongly associated with increased SS and LL, and these cause a more anterior pelvic orientation. This positional change shifts the weight centre towards the posterior, changes axial loading orientations, and creates effective forces from the posterior while standing or in a fall. These forces are predominantly the effects of the lateral cortex of the proximal femur and can increase the risk of pertrochanteric fractures in individuals with a high PI. 18 This hypothesis was confirmed with biomechanical research by Hyun et al and Roussouly et al, who demonstrated that a higher PI requires greater compensatory lumbar lordosis to maintain sagittal balance, increasing mechanical stress on the hip joint and proximal femur.19,20 Furthermore, increased PI can lead to posterior pelvic rotation due to spinal stiffness or fixed hip contractures, altering the acetabular inclination and, as a result, the stress distribution on the proximal femur.12,21 These findings collectively underline the importance of pre-fracture and dynamic imaging in future studies to better establish causality.
In the current study, no statistically significant differences were observed in PI, PT, SS, and LL among different age groups of fracture type, indicating that age alone may not have a decisive influence on spinopelvic morphology. Previous studies have shown that PI remains relatively stable with ageing, although it correlates closely with LL and sagittal alignment parameters.22,23 Nevertheless, multiple linear regression analysis revealed that age and PI were independent determinants of fracture type. With increasing age, reduced mobility of the spine and pelvis leads to higher PI and PT values, altering the axis of load transmission and increasing stress on the pertrochanteric region. Elevated PI requires greater compensatory LL to maintain sagittal balance, modifying the proximal femur’s mechanical stress distribution. These findings suggest that advanced age and higher PI values may contribute to a greater likelihood of pertrochanteric fractures, indicating that sagittal alignment characteristics could be influential in determining fracture type.
No statistically significant differences were found between fracture groups concerning BMI or SI classifications when evaluating patient-related factors. This finding indicates that bone quality and body composition may not significantly influence the relationship between spinopelvic morphology and fracture type. However, the mean age of the patients was determined to be slightly higher in the pertrochanteric fracture group. This was consistent with existing evidence that pertrochanteric fractures are more common in elderly individuals because of the probable occurrence of musculoskeletal degeneration and changes in balance.14,24,25 Some studies have also shown that patients with pertrochanteric fractures are older, weaker, shorter in stature, and could have lower bone densitometry than patients with femoral neck fractures. 20 Although no age-related differences in spinopelvic parameters were detected, these parameters may still contribute to fracture susceptibility when combined with factors such as bone mineral density, fall mechanics, and overall sagittal balance.
In a large sample study, Romero-Vargas et al found a positive relationship between BMI and pelvic incidence and suggested that increasing weight could gradually change pelvic morphology. 10 Mac-Thiong et al similarly determined age-related variations in PT and LL in asymptomatic adults. They reported that age-related posture and changes in spinal flexibility could affect sagittal alignment. 26 Although the results of the current study did not show that these variables had an effect, they should be considered in future studies of larger samples to determine in more detail the complex interactions with fracture risk.
The hypothesis associating pelvic geometry with fracture patterns is persuasive, but the retrospective design of the current study and the fact that there were no preoperative images limit the ability to establish causality. A fracture event can naturally change dynamic parameters such as PT, SS, and LL, leading to distorted measurements. Supine position radiographs in this study are essential as PT and SS are known to change with position. A few significant limitations of this study should be considered. There were no pre-trauma images, which limited the clarity of determining whether the spinopelvic differences determined were the cause of the fracture or the result. The lack of a control group of healthy individuals prevented comparative analysis. In addition, the study did not include dynamic evaluations of the sagittal alignment seen during sitting-rising movements. The fact that no postoperative images were available also limited the evaluation of how alignment could affect treatment results. The limited number of patients and the inability to meet the power analysis requirements are among the limitations of this study. The inclusion of additional variables such as DEXA-based bone mineral density, fall mechanism, and patient comorbidities would have enhanced the strength and comprehensiveness of the study; however, due to the unavailability of these data for all patients in the hospital records, they could not be incorporated into the final analysis. Finally, in addition to pelvic incidence, the spinopelvic parameters analysed are functional in nature and may be affected by pain, immobility, or compensatory mechanisms after the fracture.
Despite these inherent limitations, this study’s results highlight a potential biomechanical connection between sagittal pelvic alignment and hip fracture types. Future research should include prospective studies with biomechanical modelling, dynamic evaluation protocols, and pre- and postoperative imaging to further investigate the causal relationship between spinopelvic parameters and fracture types. İncluding postoperative data with a control group of healthy individuals would also help clarify whether or not sagittal alignment affects the decision for surgery or the postoperative rehabilitation strategies.
Conclusions
This study demonstrated that pelvic incidence and related spinopelvic parameters are associated with hip fracture morphology. Patients with pertrochanteric fractures had significantly higher pelvic parameter values compared with those with femoral neck fractures, suggesting that increased pelvic incidence may predispose to pertrochanteric fractures.
Footnotes
Ethical Considerations
This study was approved by the Clinical Research Ethics Committee of Şişli Hamidiye Etfal Training and Research Hospital, University of Health Sciences (Decision No: 3498, Date: 05/04/2022).
Consent to Participate
Informed consent was obtained from all participants.
Consent for Publication
Consent for publication was obtained from all patients included in the study.
Authors’ Contributions
SC was responsible for study conceptualization, data collection, analysis, and drafting of the manuscript.
FS contributed to data analysis and interpretation of the findings. He also participated in the critical revision of the manuscript
HMO was involved in the conceptual design of the study and contributed to drafting and revising the manuscript.
MK participated in data analysis and critical content revision of the manuscript.
YY and SE contributed to data acquisition, interpretation of results, and manuscript revision.
All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data supporting the findings of this study are available within the article and its supplementary materials.