
Abstract
Purpose:
Gait variability is a determinant of qualified locomotion and is useful for monitoring the effects of therapeutic interventions. The aim of this study was to compare gait variability and symmetry in trained individuals with transtibial (TT) amputation and transfemoral (TF) amputation.
Methods:
The design of this study was planned as observational. Eleven individuals with TF amputation, 14 individuals with TT amputation, and 14 healthy individuals (HI) were evaluated with a motorized treadmill. The mean step length, the step length variability, an ambulation index, and the time on each foot (stance phase symmetry) of participants were recorded.
Results:
There were differences between the three groups in the residual/non-preferred limb (RNp) step length (p = 0.031), the intact/preferred (IP) limb step length variability (p = 0.001), the RNp step length variability (p < 0.001), the time on each foot (p < 0.001), and the ambulation index score (p < 0.001). There was a similarity between the groups (TF, TT, HI) in IP limb step lengths (p = 0.127) and duration of prosthesis usage since amputation in individuals with lower limb loss (p = 0.224).
Conclusions:
This study provided basic data about gait variability and symmetry in individuals with traumatic lower limb loss. The results of the study showed that the variability of gait increased with the level of loss, and individuals with TT amputation showed partially equivalent performance with the healthy group. Similarities in gait characteristics may have resulted from effective prosthetic usage or effective gait rehabilitation.
Introduction
Spatiotemporal gait parameters are not absolutely uniform but rather fluctuate from one step to the next. These fluctuations are known as the gait variability, and this is associated with risk of falls and the risk for developing future mobility disability. 1 –3 Although gait variability is the result of neuromotor control system and a predictor of early age-related mobility impairment, the underlying mechanisms of variable gait have still not been adequately established. 3 Gait variability is related to multisystem functions such as peripheral and central neural system function, activity of autonomic system especially with cardiac adaptation mechanisms, musculoskeletal system, and psychiatric disorders. 4,5 Previous studies have measured the gait characteristics of individuals with amputations to differentiate the population based on fall history or reason for amputation. 6,7 Vanicek et al. 6 implied that there were differences between the “fallen” and the “not-fallen” individuals with limb loss in relation to swing time duration of the intact limb along with kinematic and kinetic measures, while there were no other differences in spatiotemporal or variability measures of gait. Tura et al. 8 proposed that the regularity in steps and strides is important, and it is sensible to determine whether the gait is normal or pathologic. 8 There were studies in variable subjects which investigated the effects of prostheses- and alignment-related factors on gait characteristics and variability 9 –11 effects of long-distance walking, 12 environmental factors, 13 and evaluating method-based factors 8 about the additional effects of osseointegrated prostheses. 14 Lin et al. 15 also investigated the relationship between the physical activity level and the gait variability in individuals with lower limb loss, and they implied that having better functional capacity and lateral stability might enable an individual with lower limb amputation to engage in a higher physical activity level, or vice versa. 15
The differential point of the present study from previous investigations was that the primary purpose of this study was to compare the gait variability based on amputation level in individuals with traumatic unilateral lower limb loss. Also, although there have been investigations in gait symmetry in individuals with lower limb loss, 8,13,16 the amputation level–related gait variability was not adequately discussed in trained individuals with lower limb loss. The principal aim of this study was to investigate the effects of amputation level on gait symmetry and variability in individuals with unilateral traumatic limb loss.
Materials and methods
Participants who had completed the traditional gait rehabilitation (10–12 sessions for 40 min) including weight-shifting, balancing, stool-stepping, gait, and joint control exercises 17 at the university biomechanics and rehabilitation department and who had applied for routine prosthetic alignment control were screened. Participants who met the inclusion and exclusion criteria (Table 1) were recruited for the study.
Inclusion and exclusion criteria.Inclusion criteria.

TF: transfemoral; TT: transtibial; HIs: healthy individuals.
Thirty-three potential participants with amputation and 17 potential healthy participants were screened for the study. Eight amputees were excluded: three individuals having peripheral vascular disease, two individuals having pain, and three individuals having metabolic syndrome. Three healthy individuals (HI) did not want to participate in the study and therefore were excluded.
Demographic data, including age, gender, height, body mass, duration of prosthetic usage since amputation, and level and side of amputation, were recorded. Also, the preferred hand side of the healthy participants were chosen to match with the intact limbs of amputees. The non-preferred hand side of the healthy group was matched with the residual limb of amputees. Eleven individuals (4 male, 7 female) with traumatic unilateral transfemoral (TF) amputation, 14 individuals (12 male, 2 female) with traumatic transtibial (TT) lower limb loss, and 14 (8 male, 6 female) HIs met the inclusion and exclusion criteria.
Participants with TT amputation used the classical-type prosthetic design with dynamic foot (Otto Bock 1D10), and participants with TF amputation used the classical-type prosthetic designs, mechanical knee joint (Otto Bock 3R15) and dynamic foot (Otto Bock 1D10).
Gait characteristics including mean step length (cm), step length variability (%), ambulation index score (a composite score relative to 100 based on foot-to-foot time distribution ratio and average step cycle), and time on each foot/single support period (stance phase symmetry; %) of participants were evaluated at motorized treadmill (Gait Trainer 2™ analysis system; Biodex Medical Systems, Inc., Shirley, New York, USA). The treadmill incorporates a belt that allows locomotion on the movable surface while recording simultaneous signals from each transducer to identify the occurrence of heel strike plus foot position during segments of the step and combines these elements with belt speed to determine step length. 18 The gait trainer system provides repeatable measurements and is objective. 19 To determine walking pace, the treadmill speeds were increased by 0.08 m/s increments until participants reported the speed that most closely resembled daily walking. 20 Once the patient reached his/her own comfortable speed, a familiarization period of 4–5 min was utilized. 21,22 After the familiarization period, gait characteristics were evaluated. More than 200 consecutive steps were collected for each participant.
The university ethics committee approved our study. Participants gave informed consent, and the clinical trial identifier number is NCT02988310. The study was utilized according to the STROBE statement.
Histogram, Kolmogorov–Smirnov, and Shapiro–Wilk tests were utilized to determine whether the parameters were disturbed normally or not. According to the test results, it was decided to use nonparametric test. Statistical analyses were performed using SPSS version 21.0 (SPSS Inc., Chicago, Illinois, USA). The Kruskal–Wallis test was utilized to determine whether there was difference between the groups. Pairwise analyses (Mann–Whitney U test) were used to detect the difference between the two groups. The Wilcoxon rank test was used to detect whether there was symmetry in inter-limb parameters. An overall 5% type-I error level was used to infer statistical significance. Study progress is summarized in a flow chart (Figure 1). Statistical analyses was performed by a specialist (working at the university’s biostatistical department) who was blind to the study groups to prevent potential bias.
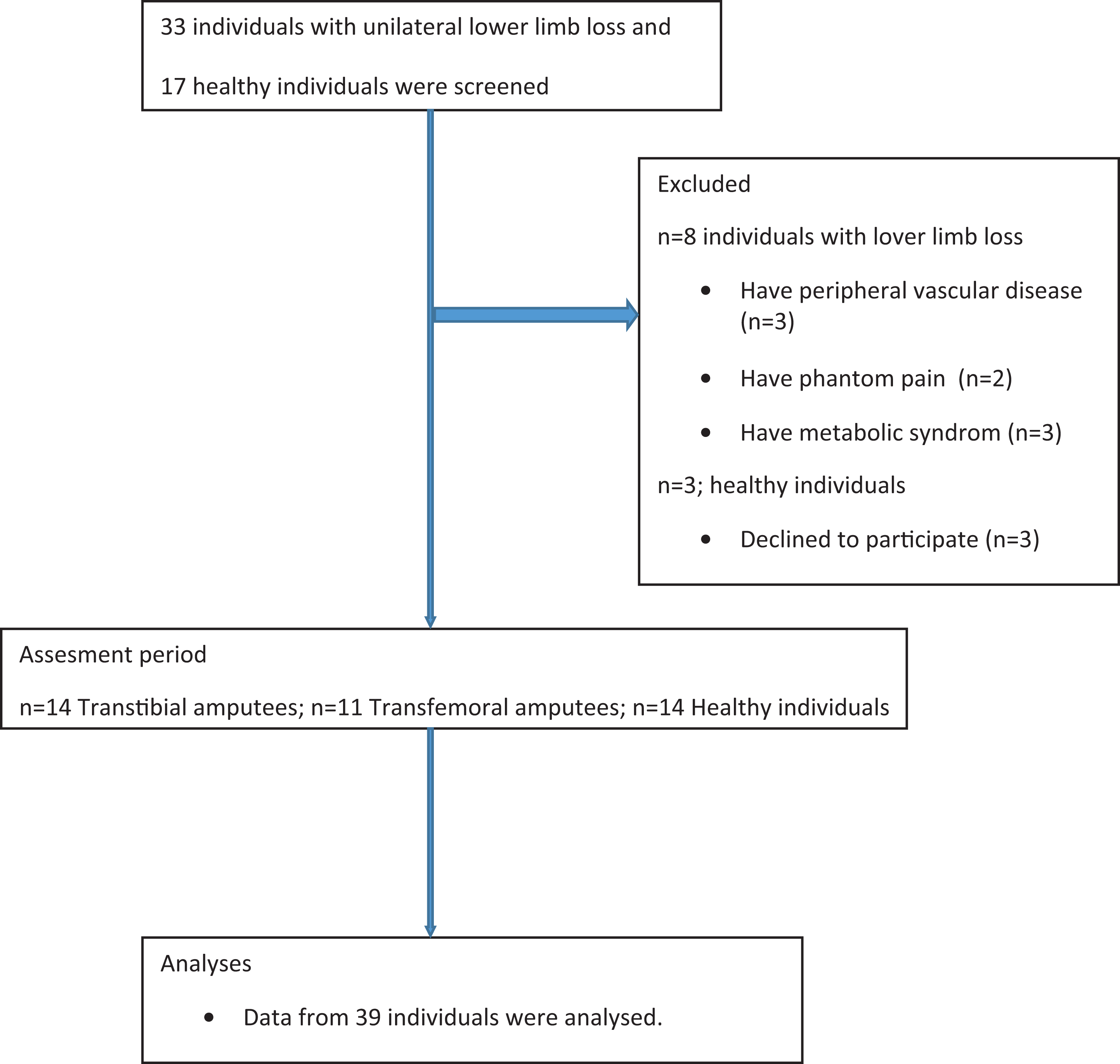
Flow chart.
Power of the study was calculated using the covariance of variability of residual/non-preferred limb (RNp) standard deviations of the groups. The power analysis showed that the study’s power was 99% with 39 participants at 0.95 effect size. The power of the study was calculated using the GPower 3.0.10 program (Universität Kiel, Germany). 23 The power α level was 0.05.
Results
There was a similarity between the groups in the demographic properties (p > 0.05). There was no difference in the intact/preferred (IP) limb step lengths (p = 0.127). There were differences between the groups in the RNp step length, the IP step length variability, the RNp step length variability, the time on each foot, and the ambulation index score, according to the Kruskal–Wallis test (p < 0.05).
Pairwise analyses of the TT and TF groups showed that there were differences in the gait characteristics (p < 0.05) between the two groups, except for the residual limb step length and the intact limb step length variability (p > 0.05). The step length variability of the TF group was higher than the TT group (p = 0.021). The ambulation index score, which shows the balance ratio between the step time and the step cycle, was lower in the TF group (p = 0.004). The time on residual limb was longer, and the time on intact limb was shorter in the TT group (p = 0.036). In other words, single support period of the residual limb of the TT group was longer. Also, the ambulation index score was higher in the TT group (p = 0.004). In other words, although there were similarities in the gait characteristics of the groups, the TT group had more stable gait pattern than the TF group.
Pairwise analyses of the TT and HI groups showed that there were differences between the TT and HI groups in the measurements (p < 0.05), except for the step lengths (p > 0.05). The variability of gait was higher in the TT group (p = 0.001). The ambulation index score was higher in the HI group (p < 0.001). The single support period of the RNp was shorter in the TT group (p < 0.001). In other words, the HI group had more stable gait pattern than the TT group.
Pairwise analyses of the TF and HI groups showed that there were differences between the groups in the gait characteristics (p < 0.05), including the RNp step lengths (p = 0.013), the IP step length variability (p = 0.003), the RNp step length variability (p < 0.001), the single support period (p = 0.006), and the ambulation index score (p < 0.001). In other words, the gait variability was higher in the TF group. The single support period and the step length of RNp were shorter in the TF group. The HI group had more stable gait pattern than the TF group. Table 2 lists the characteristics of the groups and the comparative results.
Characteristics of groups and comparative results.
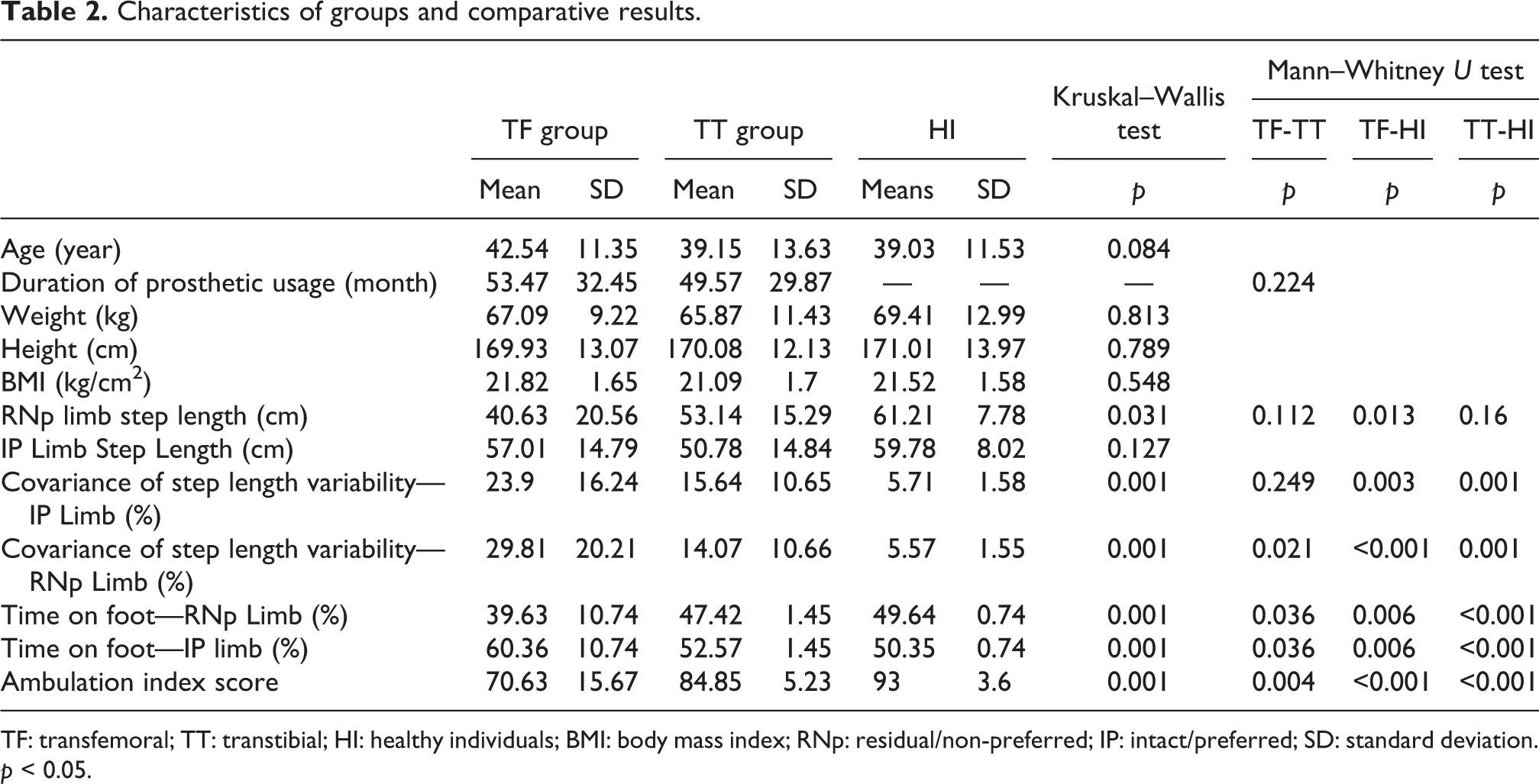
TF: transfemoral; TT: transtibial; HI: healthy individuals; BMI: body mass index; RNp: residual/non-preferred; IP: intact/preferred; SD: standard deviation.
p < 0.05.
Symmetry analyses showed that there was no asymmetry in the HI group (p > 0.05), while asymmetry was noted in the TF and TT groups. The step lengths (p = 0.01) and single support period (p = 0.009) were asymmetric in the TF group. In other words, individuals with TF limb loss spent more time on the intact limb and have a longer step length in the residual limb. The TT group showed an asymmetry in the single support period (p = 0.001); individuals with TT limb loss spent more time on the intact limb.
According to the results, the variability of gait increased with the level of loss. Individuals with TT amputation showed closer performance with the healthy group.
Discussion
This study provided basic data about gait variability in individuals with traumatic lower limb loss and showed that the individuals with TT amputation had almost equivalent gait patterns to the HI.
Gait variability is a biomechanical phenomenon that has been considered as a valuable physiological system indicator, and its presence is typically considered as a negative. 3 On the other hand, variability is a result of multisystem interactivities and is also a necessary component for neuromotor control system adaptability and sustainable mobility. 2,3
Variability in amputee gait usually depends on two factors: the prosthesis and the body properties. 6 –14 Svoboda et al. 10 investigated the influence of the prosthetic foot on ground reaction force variability for TT amputees and showed that the flexible foot provided more stability than the SACH foot. 10 Also, the study showed that there was an asymmetry in the ground reaction force between the limbs. The flexible foot had advantages for both residual and intact extremities movements. 10 In the present study, all participants used same prosthetic components. Therefore, it was possible to investigate the factors related with the level of amputation. It is inferred from the results of similarity in step lengths and intact limb step length variability between the TF and TT amputees that evaluating the consistency in steps of the residual limb can be more useful to determine the differences in gait features. Also, as already mentioned in Lee et al.’s 14 study, time on foot can be another descriptive determinant for gait analyses. 14
Interestingly, the IP limb step lengths were similar in all three groups. Possible explanation of this result was that since the reason of amputation was trauma, there was thus The possible explanation of this result was that since the reason for amputation was trauma, there was thus no necessity to would affect all gait parameters. In other words, there was no systemic or other neuromuscular damage that would affect the whole walking adaptability.
Another interesting finding of this study was that the step lengths were similar in the TT amputees and HIs. This could have resulted from two factors. Primarily, variability analyses could be more useful than spatiotemporal parameters in detecting even a minimal change in gait. Another possible explanation of this result might be the effective prosthetic design and use, or effective gait rehabilitation, was beneficial to close the functional gap due to limb loss. In conclusion, all participants with lower limb loss were already trained, and it is known that rehabilitation is essential for effective and accurate prosthetic use. 24,25 While the residual limb step length variability was different, the intact limb step length variability was similar in the TT and TF groups. It is hard to explain how this could be possible, because the lower limb movements are interdependent. 26,27 These results can be supported by the theory that the consistency of gait features was more related to central and peripheral neuromotor factors, or systemic functions, than musculoskeletal conditions. 3 On the other hand, the result of the present study was concordant with the results of a previous study which implied that the residual limb activity had instable pattern. 28
There were limitations of the present study. An important restrictive factor was that the present study does not provide any information on whether the use of another type of prosthetic component design would change the results or not. Another limitation of the study was that the evaluator of the study was not blind to the participants because of the nature of the study. It could not be possible to provide blindness to the level of amputation. However, to provide partial blindness and prevent potential bias, the statistical analysis was performed by a specialist working at the university’s biostatistical department who did not know the study hypotheses and groups.
In conclusion, this study provided basic data about gait variability in individuals with traumatic lower limb loss. According to the results, the variability of gait increased with the level of loss, and individuals with TT amputation showed partially equivalent performance with the healthy group. Similarity in the step length may result from good design and effective prosthetic use or effective gait rehabilitation; in conclusion, all participants with limb loss were already trained. Future studies should consider the impact of different prostheses and rehabilitation on the gait dynamics in individuals with limb loss. Also, analyzing the gait symmetry and/or comparing the sectional outcomes of the gait characteristics cannot provide the data of deviations from the normal gait in individuals with amputation. Therefore, the stability of gait must be evaluated to interpret the outcomes of the rehabilitation methods or determine the deviations from the natural gait.
Supplementary material
OSJ_832665_Supplementary_online_material_STROBE-Checklist-v4-MS-Word - Comparison of gait variability and symmetry in trained individuals with transtibial and transfemoral limb loss
OSJ_832665_Supplementary_online_material_STROBE-Checklist-v4-MS-Word for Comparison of gait variability and symmetry in trained individuals with transtibial and transfemoral limb loss by Hilal Keklicek, Elif Kirdi, Ali Yalcin, Semra Topuz, Ozlem Ulger, Fatih Erbahceci, and Gul Sener in Journal of Orthopaedic Surgery
Footnotes
Authors’ note
An earlier version of this article was presented as an oral presentation at the 19th International Conference on Biomechanics, 18–19 May 2017, Paris, France. All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Supplementary material
Supplemental material for this article is available online.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.