
Abstract
From the roots of cross training to the rigorous worldwide events, triathlon has become a means for physical conditioning, competition and socialization that is adaptable to everyone with a desire and commitment to participate. The novelty of athletes with limb loss competing alongside able-bodied has passed. The current expectation is that sport, including triathlon, is well within the reach of any amputee athlete with the physical ability and determination to compete. Commitment by the clinical team to the amputee athlete along with the systematic practice of prosthetic fitting, sport-specific training and accurate record keeping will not only assist today's athletes, but will establish the foundation for future amputee triathletes. This article outlines the prosthetic and training consideration for clinicians working with novice and intermediate amputee triathletes or those interested in swimming, cycling and running. In addition, prosthetic fitting and component selection and race day strategies is discussed.
Introduction
In 1974, the first triathlon was held San Diego, California, as a light-hearted break from the gruelling training typically associated with preparing for marathons. The concept of cross training grew quickly and although only 12 men competed in Hawaii at the first Ironman in 1978, today there are over 20 Ironman events worldwide to qualify for the Ironman World Championships in Kona Hawaii. Ironman Hawaii also receives over 7,000 applications for 150 lottery slots for the chance to compete in Kona each October with 1,700 qualifying competitors. Evidence of the accelerated interest in the sport is made apparent where the sanctioning organization USA Triathlon, grew from 19,000 members in 1999 to 96,000 members in 2007 and sanctions over a 2,000 triathlon events throughout the USA.[1]
A rapidly increasing number of athletes with disabilities have also found triathlon training and competition extremely rewarding as a means of healthy physical conditioning and a way of maintain the competitive spirit. One of the most internationally recognized events is the San Diego Triathlon Challenge founded in 1993 to support Jim MacLaren, the first transtibial amputee endurance racer, who was injured during a triathlon competition. The event exemplifies the strong bond between able-bodied and disabled athletes as hundreds of athletes with varying disabilities compete alongside and in tandem with able-bodied triathletes.[2]
From the roots of cross training to the rigorous worldwide events, triathlon has become a means for physical conditioning, competition and socialization that is adaptable to everyone with desire and commitment to participate. Not all triathlons are ‘Ironman’ competitions that require a 3.8 km swim, 180 km bike and 42.2 km mile run; sprint distance triathlons are excellent introduction races with a 500 m swim, 20 km bike and 5 km run. For people with limb loss the decision to prepare for the complexities of a triathlon, of any distance, is a commitment that requires discipline, dedication, and motivation. The physical and mental demands for a triathlete with limb loss are greater than the average able-bodied athlete, but the rewards can be equally fulfilling.
This article outlines the prosthetic and training consideration for clinicians working with novice and intermediate amputee triathletes or those interested in swimming, cycling and running. In addition, prosthetic fitting and component selection and race day strategies is discussed.
Prosthetic socket design and component selection
Transtibial socket considerations
A well fitting prosthesis is essential with regards to distance training performance and the reduction of injury risk. To date, no specific socket design or method of suspension has been demonstrated to be superior over another for sports. In fact, many triathletes will choose to use different prosthetic designs for cycling and running. During the socket fabrication process, the prosthetist and athlete should consider comfort, range of motion (ROM), stability and adaptability to volume changes. Comfort is a combination of socket shape, interface material selection, alignment and the ability of the socket to adapt to forces imposed at the stump-socket interface. The transtibial socket should permit adequate knee ROM while simultaneously providing enough stability to reduce any uncharacteristic knee joint motion that could hinder performance or lead to injury. Many athletes require greater knee flexion in their cycling prosthesis than their running prosthesis; therefore, they prefer either two different sockets or a single socket that provides a balance of the biomechanical requirements between the two events.
Residual limb volume fluctuations and suspension is a constant challenge for endurance athletes. Initially, there is often a reduction in volume from the onset of training as body fat is reduced and muscle reshapes the limb. Secondly, during long-distance cycling and running bouts, the loss of body fluids can result in a reduction in residual limb volume and create excessive movement within the socket. The use of silicone or gel liner suspension sleeves will assist in the reduction of shear forces, compression and peak pressures.[3] In the event of body mass loss or changes in residual limb shape, modification with leather or pelite pads within the socket surface can accommodate for minor volume changes. Eventually a new socket should be fabricated to reduce the possibility of additional friction to the skin from the pads. Throughout training, the athlete will learn how to accommodate fitting and limb volume issues utilizing socks or conferring with their prosthetist for permanent socket modifications.
Using locking liners, one-way suction valves or Seal-In liner systems will eliminate the need for an external sleeve suspension that limit the knee ROM during running and cycling. Donning either a silicone or urethane liner system with the knee pre-flexed 5–10° can help reduce the material bunching and skin pressure in the posterior aspect of the knee. Suspension sleeves with wave or undulated features are designed to allow for increased knee flexion without gathering of excess material. For transtibial amputees with short residual limbs, athletes can utilize a supracondylar cuff strap or elastic two inch waist belt with inverted-Y strap to augment suspension.
Transfemoral socket considerations
Transfemoral amputee athletes will often experience friction issues at the proximal brim during running and especially during cycling. The use of an ischial containment socket is believed to permit greater proximal stability and use of the hip musculature during running. The height of the proximal brim is frequently an issue where the belief that the greater the ischial containment the greater stability. Conversely, with a higher medial socket wall there is greater proximity to the ramus bone and the surrounding soft tissues that can cause discomfort with the increased forces experienced during running. Finding the balance between containment and comfort is often a challenge early in the training process. Since stability is not as important during cycling, athletes will often choose to lower the height of the medial wall of the socket for increased comfort and reduce the friction to skin caused by the medial brim.
For those athletes who choose to use two different sockets, the time to change sockets becomes a consideration. To help aid in the first transition from the swim to cycling, a pin-locking socket design can reduce the time to don the prosthesis, ensure that limb will maintain suspension and diminish the need for a high medial socket wall.
Prosthetic component selection
Selection of the running prosthetic foot depends on the residual limb length, distance of the event and the athlete's preference. The novice athlete may choose to use their existing prosthetic foot while exploring their enthusiasm for the sport and the necessary prosthetic requirements. Moreover, it is not uncommon for distance runners or multisport athletes to select a carbon fiber foot with a heel as their preferred running foot. While the versatility of using a traditional walking prosthetic foot when running is attractive to some runners, a foot specifically designed for running feet are frequently preferred by athletes with the necessary financial resources.
Specifically designed running prosthetic feet for transtibial amputees have been found to have a significant reduction in heart rate and energy cost over prosthetic feet designed for walking, but have no physiological advantage when compared with non-amputee runners.[4] The first prosthetic foot specifically designed for distance running is the Ossur Flex-Run (Ossur Americas: 27412 Aliso Viejo Parkway Aliso Viejo, CA, USA) which is constructed from carbon fiber material, eliminates the heel and has a large radius or ‘C-shaped’ curvature designed to allow the runner's center-of-mass to move further forward over the toe with the purpose of deflecting the foot-plate from mid-stance to toe-off[5] (Figure 1). The increased vertical deflection theoretically permits the sound and prosthetic limb to achieve a more symmetrical stride length with a reduction in effort during running. A similar design is the Freedom Innovations Nitro Running Foot (Freedom Innovations: 30 Fairbanks, Ste 114 Irvine, CA, USA). Although widely favored by sprinters, some endurance runners prefer a sprinter's prosthetic foot (Figure 2).
A triathlete with transtibial amputation running with Ossur Flex-Run™ carbon graphite running foot. A transtibial distance runner with an Ossur Cheetah Flex-Foot competing in the Challenged Athletes Foundation Annual San Diego Triathlon Challenge.

Running style, speed, and terrain often influence the runner preference to the style of foot selected for their running prosthesis. For a transtibial amputee a clearance of 17–25 cm is required from the distal residual limb to the floor. If adequate clearance below the limb is not available, a posterior mount approach of the Ossur Cheetah foot may be applied, where the foot's pylon is fabricated into the exterior posterior wall of the socket. The Otto Bock 1E90 Sprinter (Otto Bock North American Headquarters: 2 Carlson Parkway North Suite 100 Minneapolis, MN, USA) is also mounted posteriorly and is designed for the short-distance runner, but may be used for long distance as well. Manufacturer's specifications for assembly may vary and should be followed by the prosthestist.
To properly determine the running foot's resistance category, it is important to accurately weigh the athlete. Running Cheetah feet are often fitted a half a category lower to reduce the impact moment, slow the deflection speed of the prosthetic foot and increase the swing time for sound limb. Currently, there is no objective method to dynamically determine foot category and therefore observation and the subjective feedback of the runner is still the most common approach.
Running feet are not generally used for cycling. Prosthetic foot and ankle stiffness appears to influence performance with transtibial cyclists who are able to perform at higher metabolic intensities, whereas those training or competing at lower metabolic intensity are able to use prosthetic feet with higher compression rates.[6] Cycling with a rigid ankle,[7] such as a standard J-shaped carbon fiber prosthetic foot, would be appropriate for an elite cyclist.[7] Some cyclist construct custom-made foot attachments with rigid ankles are fabricated for cycling only. However, novice and intermediate level cyclist will not be at a disadvantage if they train with their existing prosthetic foot[6] (Figure 3).
A cyclist with transtibial amputation using a stiff carbon fiber foot.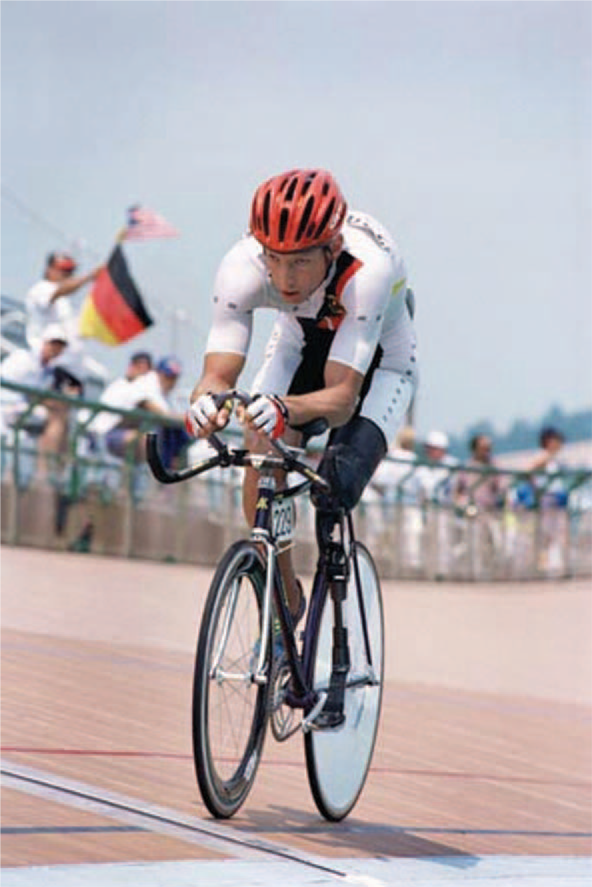
Frequently, cyclists will center the pylon over the pedal, in some instances the cyclist will cut the footplate in order to center the foot over the pedal or crank (Figure 4). It has been determined that for transtibial cyclists, the optimal placement of cleat is directly over the pedal.[8] Transtibial amputee cyclists may choose to directly attach their prosthesis to the pedal or crank; therefore, they must have a socket design that will permit them to quickly don the limb as they mount or sit on their bike. The obvious drawback to directly attaching the prosthesis to the bike would be in the event that the cyclist must dismount quickly, because of a flat tire or the need to walk to an aid station. Many cyclists prefer stirrups over toe clips for ease and speed of mounting and dismounting the bike.
A cyclist with transtibial amputation using a custom prosthesis with the pylon directly over the pedal.
The transfemoral amputee runner has the same options for prosthetic running feet as does the transtibial amputee runner. Because of alignment, foot stiffness and performance, presently transfemoral athletes prefer the Ossur Flex-Run foot for distance running. The reduction of ground forces and the increased time to advance the sound limb allows for more efficient and comfortable running style.
Transfemoral amputee distance runners have a choice, whether to use a prosthetic knee unit or run without the knee in favor of a straight pylon from the socket to the foot. Use of a prosthetic knee permits a more traditional style of running with knee flexion and extension. Three commonly observed knee systems at long-distance athletic events are: The Ossur Mauch Swing'N'Stance (SNS) Type Hydraulic or the S-Type Swing Only Hydraulic knee (Figure 5), The Ossur Total Knee 2100 hydraulic fluid control and polycentric knee axis design (Figure 6), and the Otto Bock Modular Polycentric Axis Joint (3R55) with Hydraulic Swing Phase Control (Figure 7). The Mauch Hydraulic cylinder uses a single-axis frame, and the SNS-Type offers athletes a wide range of resistance adjustment and stance control. Most competitive athletes, however, use the S-Type Swing-Only hydraulic unit because stance control is no longer necessary with athletes who are successful runners. For distance runners, the Total Knee 2100 with 3-phase hydraulic swing control including the extension promoter that assists with control of excessive heel rise that could slow the runner is favored. The Otto Bock 3R55 Polycentric Axis Joint is a favorite for knee disarticulation athletes because of the instantaneous center of rotation capabilities of a four-bar design, providing increased toe clearance and stride symmetry. Lowering the prosthetic knee joint center has also been found to improve stride symmetry and improve running speed.[9]
The Ossur Mauch SNS hydraulic knee. The Ossur Total Knee 2100 polycentric knee. The Otto Bock 3R55 hydraulic knee and Ossur Flex-Run on a triathlete with knee disarticulation amputation.


Running without the knee requires a circumducted swing phase and reduced arm swing. The metabolic difference between the two running styles has not been reported in the literature. The advantage of distance running without a mechanical knee anecdotally described by some transfemoral athletes is the decreased need to constantly survey the running surface for fear of landing on uneven terrain that would cause the prosthetic knee to suddenly collapse. Likewise, they report an associated reduction in the mental concentration required to ensure that the prosthetic limb strikes the ground with the knee extended, especially during the final miles of a long triathlon when they are physically and mentally fatigued.
Transfemoral cyclists may prefer a polycentric knee axis where the instantaneous center of rotation moves the shank under the knee center during knee flexion for a more symmetrical movement between lower limbs. Prosthetic knee stance control is not a consideration as transfemoral amputees find it very difficult, if not impossible, to stand out of the saddle and pedal when climbing hills. Triathlon events do not use any classification system restricting the use of a prosthesis and as a result the transfemoral amputee athlete must decide if the power generated by the prosthesis warrants the added weight, awkwardness and complexities of using a prosthesis. The main concern of not having a prosthesis would be in the ability to walk in the event of an unscheduled incident such as an extremely steep hill or a flat tire.
During any sanctioned International Triathlon Union (ITU), United States of America Triathlon (USAT), or the World Triathlon Corporation (WTC) races, swimming with any aid such as a prosthesis or orthosis is prohibited. During the first transition, an amputee exiting the water does have the option of donning prosthesis to run or walk to the bike transition. If the athlete chooses not to use prosthesis they have the option to use crutches, receive assistance from a volunteer or to hop to their bike at the first transition station (Figure 8). Amputees do employ the use of a swim leg during training or recreational swims for strengthening and increased mobility. Adaptive devices such as the Rampro Active Ankle (Figure 9) (Rampro: 709 North Nevada Street Oceanside, CA, USA), or the Freedom Freestyle Foot (Figure 10), can position the prosthetic foot in either plantar flexion for swimming or a neutral dorsiflexed position for walking or transitioning from the water to the cycling station.
A transtibial amputee triathlete using crutches as she exits the water during the first transition. The Rampro Active Ankle that permits plantarflexion for swimming and a neutral ankle for walking. The Freedom Innovations Freestyle ankle that permits plantarflexion for swimming and a neutral ankle for walking.


It is suggested that the athlete be reminded during each transition to keep any sand, dirt, or rocks off of the liner and make sure to don a clean liner or interface with no debris. This will help reduce fit problems or skin irritation issues that would become apparent later in the workout or race.
Triathlon equipment
Choosing the right equipment such as footwear, bikes, clothing and other accessories for triathlon training and competition is a process that will occur over time. During the equipment selection process, the amputee athlete has three basic criteria to consider: (i) Safety or injury prevention, (ii) comfort, and (iii) performance. Improper equipment can lead to injury or affect athletic performance.[10] Additionally, if the injury prevents pain-free use of the prosthesis, participation in daily activities such as work and social events could be limited.
Findings with able-bodied athletes report that there is a high prevalence of injury with triathletes directly correlated to the training mileage and the duration of participation in the sport. Approximately 56–78% of triathletes will experience injuries over time. [10-12] An average of 2–3 anatomical sites affected with the majority of injuries are related to overuse with a number of injuries sustained correlating to distance and the number of workouts.[7] Another estimate suggests that during training, an average of 2.5 injuries occur per 1,000 training hours and the injury rate increases to 4.6 injuries per training hours during the competition season.[12] The life time incidence of low-back pain and cervical pain was found to be approximately 68% and 48% respectively, with a little over 20% being discogenic in origin.[13] Although to date no studies have examined the prevalence of injury in amputee triathletes, it does stand to reason that because amputees are at a higher risk for degenerative joint disease in the sound limb14,, [15] and low back pain[16] than the general population, attention must be paid to injury prevention and comfort.
The reasons for injury include duration of triathlon participation, previous history of injury, high pre-season running mileage, inadequate warm-up and cool down.[8] Strategies to maintain endurance, develop form and prepare properly for competition are essential for the amputee triathlete's preparation and training program. The use of a training log is one of the most important pieces of equipment that a novice triathlete could maintain. The value of a training log is that if, and more likely when, injuries or problems occur, there will be an accurate record of diet, training routines and mileage that will allow the athlete together with the clinicians reviewing the training log to determine attributing factors.
Training logs can be as simple as using a paper notebook or as sophisticated as a specially designed computer program. The key elements of the log include: Training dates, durations, workout routines, weather, training conditions, diet and any health-related issues such as minor or persistent injuries. Accurate logs can be helpful not only with maintaining training consistency and motivation but can also be valuable in detecting where changes in mileage or equipment such as new shoes or bike parts that might contribute to an injury.
Moreover, amputees should log all prosthetic changes and dates. While clinicians record most major prosthetic modifications, often the small subtle changes can have an effect on sports prosthesis; therefore, accurate records keeping can be a valuable asset when assessing future problems. The following information related specifically to the amputee should be recorded in the training log. Dates for receipt of a new internal suspension sleeve should be recorded to determine average wear life to prevent material wear that may lead to increased skin friction and blisters. This will help gauge the timeframe for ordering new sleeves before the existing one becomes worn and a potential risk to the skin. New prosthetic feet with resistance category information and any customization performed. Prosthetic knee information should include installation dates and fluid viscosity. All socket changes include trim line alterations, socket relieves, added pads and replacements. Every alignment or prosthetic height changes should be recorded. These values should be exact as possible including how the values were measured. This information is rarely maintained, but can prove to be the most critical when trying to evaluate soft tissue, joint or back pain. Any changes to the everyday prosthesis should be recorded as well. Often a new prosthesis or changes to the existing prosthesis can contribute to musculoskeletal pain.
Swimming
For the amputee athlete, swimming is a low-impact training activity to build endurance and strength without traumatizing the residual limb soft tissues. Most athletes initiate training in a pool. Entry and exit from the water should be performed carefully. Walking on the pool deck without the prosthesis should be performed using crutches with tips designed for wet surfaces. Hopping can lead to unforeseen slip and falls resulting in injury. A simple water-resistant prosthesis can be an asset especially when the triathlete begins open water training and must negotiate the beach and other less stable terrains.
In the water, a pair of goggles and a comfortable swim suit is all that is required. When the athlete is ready for open water training such as a lake or the ocean, then choosing a properly fitting wetsuit with a specialist is important. Most wetsuits can also be tailored for the residual limb. Wetsuits have several benefits including increased buoyancy, increased safety, improved comfort and the ability to train or compete at a wider variety of venues where water temperature is a concern.[17]
There are numerous techniques and training programs that will assist the amputee in becoming an accomplished swimmer. Joining a community or masters swim program where instruction and peer motivation is available would be beneficial for any novice competitive swimmer.
Cycling
Cycling is another low-impact endurance sport for the amputee athlete with limited risk of injury to the residual limb.[18] Most transtibial amputees will wear a prosthesis during cycling, conversely, many transfemoral amputees elect not to ride with their prosthesis because of the poor power production and discomfort.
Cycling injuries in the general population are related to poor bike positioning.19,, [20] Injuries such as iliotibial band syndrome, patella pain syndrome and low back pain are often related to seat position, saddle position, cleat alignment, handlebar position or athlete predisposing to injury because of posture or anatomical anomalies.20,, [21] To ensure that the athlete is properly fitted to the bike, with or without a prosthesis, a clinical specialist should evaluate the cyclist posture. Likewise, if an athlete has chosen to start training, or decides to train indoors during the winter on a stationary bike, positioning and fit should also be evaluated. Because amputees tend to asymmetrically produce power with the sound limb being a major force generator, riding posture must be evaluated in an effort to promote as much postural symmetry as possible.
The purchase of an expensive, high-tech bike is not necessary as many novice cyclists will start training with a road, mountain, or hybrid bicycle that should be comfortable to ride and in good condition. Typically, as the commitment to the sport of cycling increases, the more an athlete begins exploring options for better bikes and advanced technologies for improved performance. Alternative cycles such as recumbent bikes or handcycles should also be considered for training and competition because these designs may reduce the risk of injury and permit longer training rides.
Running
The highest impact for amputee triathletes occurs during running. Running also has the greatest risk of injury.[10] Similar to able-bodied triathletes, frequently amputee triathletes will limit their running mileage to weekly distances that will allow them to maintain a competitive level of performance, in an attempt to reduce the risk of overuse injuries. The appropriate distance varies depending on the athlete's fitness, level of limb loss, the training environment and type of event they are preparing to compete.
Running shoes should be properly fitted, lightweight and designed for specific events. If the amputee decides on a single shoe for both training and racing, the sole of the shoe for the prosthetic limb is often mounted to the surface of the prosthetic foot. Adherence to the prosthetic foot increases traction, reduce slippage and improves the running surface feedback. Not all distance runners will affix the sole of their running shoe to their prosthesis. Many like the ability to vary their shoe selection and do not find the slippage an issue that affects performance.
Amputee-specific equipment
The amputee athlete will have other equipment considerations that are unique to prosthetic wearers. Over time, the athlete will learn what specific items are required for specific workouts or competitions. The following is a list of equipment that may prove beneficial to novice amputee athlete:
Small towel and powder: Perspiration is a constant problem for athletes, especially during the warmer months and longer training sessions. Having a small towel and a small container of corn starch or baby powder to dry and powder the residual limb will pre-empt skin problems and improve comfort. Antiperspirants and other products designed to reduce perspiration are available but should be used with caution and the skin examined regularly until the effects are known.
Moist-wipe or alcohol wipes: Cleaning of the socket, liners or suspension sleeves must be performed immediately after training or competition. Prepackaged cleaning towels can make keeping the socket and suspension sleeves clean and free from dirt residual perspiration.
Skin dressings: When skin abrasions or blisters occur, a frictionless bandage using surgical dressings and gels can allow the athlete to continue. However, great care should be employed to limit the skin damage and not push beyond what the skin and soft tissue can safely tolerate.
Extra stump socks: Frequently, because of the muscular contractions, altered diet and sometimes changes in altitude, limb volume may change. Carrying extra socks during training to accommodate volume fluctuations can prevent many issues such as skin abrasions, loss of suction and the increased effort with cycling or running that occurs when trying to keep control of a loose prosthesis.
Elastic sleeve or auxiliary suspension: Early in training or long-distance event the presence of excessive movement within the socket can become so great that the prosthesis may tend to rotate or move to the extent that security in the prosthesis has been lost. After sock adjustments have been made, additional suspension with an external elastic suspension sleeve or temporary suspension belt can help.
Lamb's wool: In some cases, increases in muscle girth or swelling of the residual limb within the socket can result in the loss of distal end contact with the socket. One temporary remedy is to place lamb's wool at the bottom of the socket to eliminate any void. This is only a temporary remedy; the prosthetist should make modifications to address the change in volume.
Small tool kit: Most athletes carry their own tools to make prosthetic adjustments, minor repairs or to change prosthetic feet.
Conclusion
The novelty of athletes with limb loss competing alongside able-bodied has passed. The current expectation is that sport, including triathlon, is well within reach of any amputee athlete with the physical ability and determination to compete. Just as sports medicine has become a specialty within so many fields of medicine, select clinicians need to develop a similar specialty within the field of prosthetic and amputee rehabilitation. The scientific evidence is currently lacking with respect to sports and amputees; however, becoming familiar with current prosthetic technology, existing literature with able-bodied athletes and the sharing of existing clinical strategies will help serve the emerging generation of amputee athletes and advance this rapidly growing field. Commitment by the clinical team to the amputee athlete along with the systematic practice of prosthetic fitting, sport-specific training and accurate record keeping will not only assist today's athletes, but will establish the foundation for future amputee triathletes.