
Abstract
Background: Lower limb amputations should be evaluated carefully, especially with regard to the possibility of preserving the knee joint to enable a more physiological gait and lower energy consumption. Below-knee amputations were performed immediately below the tibial tuberosity with maintenance of the insertion of the patellar tendon, resulting in very short, but functional stumps. This case study examined whether very short below-knee stumps allow a more functional gait, as compared to more proximal amputations.
Case Description and Methods: Between June 2010 and June 2011, four patients had extremely short below-knee amputations, with resection of the head of the fibula at the junction and reinsertion of the collateral ligaments and structures attached to the tibia. This was followed by placement of a prosthesis with a vacuum-assisted suspension socket.
Findings and Outcome: At the end of treatment, patients that underwent transtibial amputations with an extremely short stump were considered well adapted to their prosthesis and were satisfied in relation to the acquired gait patterns.
Conclusion: The extremely short below-knee amputation, despite having a short lever arm should be considered as another option for lower-limb amputations, although we cannot yet assure that other patient groups undergoing this level of amputation may have the same results of the study.
The extremely short below-knee amputation, despite having a short lever arm should be considered as an option for lower limb amputations, as it can provide a prosthetic provision with a good functional outcome.
Background
Currently, amputations are indicated for different reasons, such as neuropathic and vascular diseases, trauma, infections, tumors and congenital malformations. The surgical techniques follow specific principles, seeking to provide a good residual limb, which allows a proper fitting to restore the functionality of the amputee. However, the choice of the level of amputation should be addressed thoroughly, so that the best results are achieved with rehabilitation.
In lower limb amputations, the proximal level of below-knee amputation that enables almost normal function should be considered. 1 The preservation of the knee joint allows good control of the prosthesis while walking, because the knee flexion and extension in stance and swing phases is physiological. Burgess defined the ideal length for below-knee amputation as 15 cm below the knee. 2 According to Mayfield, short below-knee stumps have bone lengths of 5.1–10 cm and very short stumps have lengths of 2.54–5.1 cm. 3 In contrast, Pant and Younge, below-knee stumps less than 3 cm are not functional, and suggest lengthening of the stump with the distal tibia. 4
In more proximal amputations, such as knee disarticulation and above-knee amputation, the presence of a mechanical knee, with different mechanisms positioned distal to the amputation stump, requires compensatory movements performed by the hip extensor and flexor muscles to control the knee joint, increasing the energy expenditure when using the prosthesis.5,6 According to Gonzales et al., this increases the energy expenditure of above-knee amputees during walking by up to 65%. 7 Pinzur et al. found that below-knee amputations have a lower energy expenditure, although the shorter stump consumes more energy when walking, as compared to longer below-knee stumps.8,9
Considering the great advantage of below-knee amputation in relation to higher levels, a below-knee amputation can be performed immediately below the tibial tuberosity, maintaining the insertion of the patellar tendon, and resulting in extremely short functional stumps, allowing good fitting and rehabilitation.
Case Description and Methods
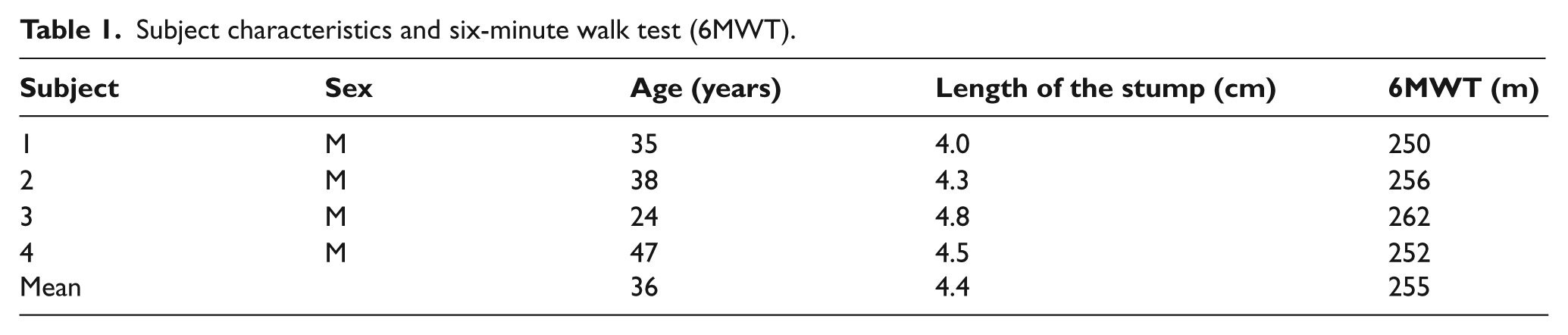
Between June 2010 and June 2011, four below-knee amputations with very short stumps were performed at the Clinical Hospital of the University of Campinas, in patients who would otherwise have undergone above-knee amputations. The study was submitted to ethical approval and informed consent was obtained from the patients. The patients were male and had amputations caused by trauma. Their mean age was 36 (range 24–47) years (Table 1). The tibial bone stumps were 4.0–4.8 cm long, as measured using nuclear magnetic resonance (NMR). In the surgical procedure for very short stumps, the total resection of the fibula is performed to regulate the bone in the region of the proximal tibiofibular junction and involves a new insertion of the collateral ligaments and the structures attached to the tibia. The removal of the fibular head allows the surgeon to gain extra skin, which is often important for covering the stump. The stumps were kept in rigid extension with a bandage for three weeks.
Subject characteristics and six-minute walk test (6MWT).
After three weeks, the sutures were removed and the patients referred for rehabilitation. Guidance on the use of a compressive elastic bandage for 24 hours/day, positioning the stump in extension, isometric contraction exercises, and strengthening the flexor and extensor muscles of the knee was given. The fitting process was initiated eight weeks post-surgery, using endoskeleton prosthetic legs with a vacuum-assisted suspension socket. The rehabilitation process and gait training started between parallel bars and then with the aid of a cane to complete independence with patients ambulating on flat and uneven, ramps and stairs. Rehabilitation of amputees with prostheses was carried out for eight weeks.
Findings and Outcomes
The six-minute walk test (6MWT) was fulfilled in the last week of training and the average result was 255 (range 250–262) meters (Table 1). 10 The stumps were examined daily after the training session. No complication was observed during the training period and the patients showed no significant gait deviations. At the end of the study a verbal yes/no question was performed to evaluate a patient’s level of satisfaction with their prosthesis.
Discussion
The maintenance of the knee joint is critical to the successful rehabilitation of amputees, especially elderly amputees or those with vascular disease and other comorbidities, which currently represent the largest population of amputees.
In this small case series, we note a limitation in the study because it involved only young patients, male and trauma amputees. Further more comprehensive investigation with other patient groups (male, female, age and etiology) must be carried out to check whether patients will also benefit from the proposed level of amputation.
Census data from the Brazilian Institute of Geography and Statistics in 2000, revealed the existence of 24.5 million people with a disability in Brazil, representing 14.5% of the population. Of these, 5.31% have amputations, which represents more than 1.3 million Brazilians. It is estimated that lower-limb amputations constitute 85% of all amputations, although there is no accurate epidemiological information.
In 1991, Bowker defined the optimal level of amputation as the most distal level possible with healing potential. 11 Although the ideal surgical level for below-knee stumps is considered to be the muscle-tendon junction of the gastrocnemius, the classification and length are controversial. According to Mayfield, short transtibial stumps are 5.1–10 cm and very short stumps 2.54–5.1 cm, while Bowker recommended that the length of the transtibial stump should not be absolute, but related to height.1,3 In this study we define extremely short stumps as those involving cross-sections made just below the bony insertion of the patellar tendon on the tibial tuberosity. This insertion, which is responsible for the action of the quadriceps in knee extension and control of the prosthesis, is critical to the functionality at this level of amputation.
Regardless of etiology, a below-knee amputation has numerous advantages, like preservation of the knee joint, reduction in energy consumption during walking, ease of placement and removal of the prosthesis and easier rehabilitation. Therefore, this amputation level should be prioritized, even when the procedure will result in an extremely short stump.
Pedrinelli suggests that the success of rehabilitation following amputation surgery is related to the level. At least 90% of the patients with below-knee amputations, but only 25% of above-knee amputations, make proper use of the prosthesis. 12
With prosthetics, an anatomical cartridge with a greater total contact area helps to distribute pressure. With resection of the fibula, it became possible to support weight on the side of the stump, which became important with this type of fitting. The prosthesis for short stumps can have a patellar-tendon-supracondylar type socket or a vacuum system. Due to the small lever inside the prosthetic socket, the stump can move within the socket during forced flexion or when the patient is seated. We used sockets with a vacuum suspension system, which, in addition to providing greater protection and comfort, best fixed the stump in the prosthesis socket during use. We did not include any auxiliary socket or suspension to stabilize the knee joint, as proposed by Isakov et al. when fitting a very short stump with a Swedish knee-cage. 13
Conclusion
The preservation of the knee joint in lower-limb amputees is key to a more functional prosthesis with less energy expenditure. However, many surgeons still perform proximal amputations, like knee disarticulation and above-knee amputations, because they do not believe that extremely short below-knee stumps can be functional. An extremely short below-knee stump can be performed since it preserves the insertion of the patellar tendon and good circulation. The extremely short below-knee amputation, despite having a short lever arm, should be considered as an option for lower limb amputations, as it allows a prosthetic provision with good functional outcome. The results indicate that patients in this study were considered well adapted and satisfied with their prosthesis based on gait pattern and daily independence. Future research is needed to determine whether the same results are found in other patient groups, such as older amputees with peripheral arterial disease and after above-knee amputation.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors declare that there is no conflict of interest.