
Abstract
We present a new methodology to measure the running biomechanics of amputees. This methodology combines the use of a spring-mass model and symmetry index, two standard techniques in biomechanics literature, but not yet used in concert to evaluate amputee biomechanics. The methodology was examined in the context of a pilot study to examine two transtibial amputee sprinters and showed biomechanically quantifiable changes for small adjustments in prosthetic prescription. Vertical ground reaction forces were measured in several trials for two transtibial amputees running at constant speed. A spring-mass model was used in conjunction with a symmetry index to observe the effect of varying prosthetic height and stiffness on running biomechanics. All spring-mass variables were significantly affected by changes in prosthetic prescription among the two subjects tested (p < 0.05). When prosthetic height was changed, both subjects showed significant differences, in Δy max, Δl and contact time (t c) on the prosthetic limb and in kvert and kleg on the sound limb. The symmetry indices calculated for spring-mass variables were all significantly affected due to changes in prosthetic prescription for the male subject and all but the peak force (F peak) for the female subject. This methodology is a straight-forward tool for evaluating the effect of changes to prosthetic prescription.
Introduction
The development of amputee/prosthetics research has advanced due to the availability of improved technology to perform consistent and repeatable biomechanical studies on amputees with various levels of functional ability. There has been an increased emphasis on improving the measurement techniques used in the biomechanical analyses of amputees, but there is often difficulty linking the quantitative results to clinically relevant findings.[1] This difficulty is compounded by the inconsistency in measurement approaches limiting the ability for comparison between studies.[2]
In a review of general, able-bodied running biomechanics literature, Novacheck notes that there is ‘a significant void’ between the biomechanist and the clinician.[3] This divide between quantitative analyzes and qualitative observations is of concern in amputee biomechanics literature as well[2]. Measurement-based conclusions that are in agreement with the observations of clinicians and the amputee subjects are not often possible. Anecdotally, amputee runners describe instances where they perceive a difference in performance and comfort when foot alignment, height or stiffness categories are altered; however, methods to detect the effects of the change have not been adequately described. Clinically, aside from prosthetic alignment, the two prosthetic foot variables most often suggested to have the greatest potential to impact running performance are prosthetic height and stiffness category. To date the contribution of prosthetic height and stiffness has not been established.
As the functional abilities of amputees have been increased by improved prosthetic devices and clinical experience, more literature has addressed the subject of amputee running. Some studies have investigated transtibial amputee biomechanics in terms of muscle work and energy transfer.[4-7] The influence of the prosthetic device has been explored using the energy transfer approach[8] as well as the traditional gait analysis approach, comparing kinematic and kinetic variables.9,, [10]
Each of these studies has contributed to the advancement of the descriptive techniques used to gain insight into the physiological adaptations the amputee employs to run; however, it should be noted that such methods assume rigid body kinematics. Rigid body models have been used extensively[3] and are a useful, convenient approach to studying able-bodied biomechanics, but these models may not be ideally suited to observing amputee biomechanics, especially when considering the use of running prosthetic devices. It has been suggested that the varying levels of amputation and differences in the prosthetic devices prevents direct comparison between sound and prosthetic limbs or between subjects when using rigid body models.[11]
Amputees tend to exhibit asymmetric gait patterns, so it is not surprising that inter-limb symmetry has been investigated extensively by comparing measured gait parameters of amputees.[12-18] While these studies have contributed much to the field of amputee research, the variability in these methods hinder comparisons between limbs, between amputees and the able-bodied subject population, and between the studies themselves.
Spring-mass modeling literature
Research into running biomechanics of able-bodied subjects is extensive and has produced various methods for analysis.3,, [19] Spring-mass models have been used as a method to examine running biomechanics.[20-23] While there is some variability in some of the specific assumptions and implementation of this methodology,[24], 24,25 spring-mass models have been used in a variety of applications and research avenues.[26-31]
While some spring-mass modeling literature has suggested that the approach could be applied in the evaluation and design of prosthetic limbs for running,22,, [30] to the best of our knowledge, there have been no published studies to date that have used a spring-mass model or to evaluate amputee biomechanics. Only some parameters used in spring-mass models (t c, F peak) have been compared between limbs with a symmetry index.
The aims of this study were to propose and investigate the use of a new methodology to measure the running biomechanics of amputees. This method was evaluated in the context of a pilot study to observe the effects of changing prosthetic alignment and stiffness parameters on the behavior of amputee sprinters. Since quantitative measurement sensitivity is of high importance to amputee research, the efficacy of this method would be determined by the model's ability to demonstrate significant differences in measured spring-mass characteristics and inter-limb symmetry within subjects due to changes in the prosthetic setup between running trials.
Methods
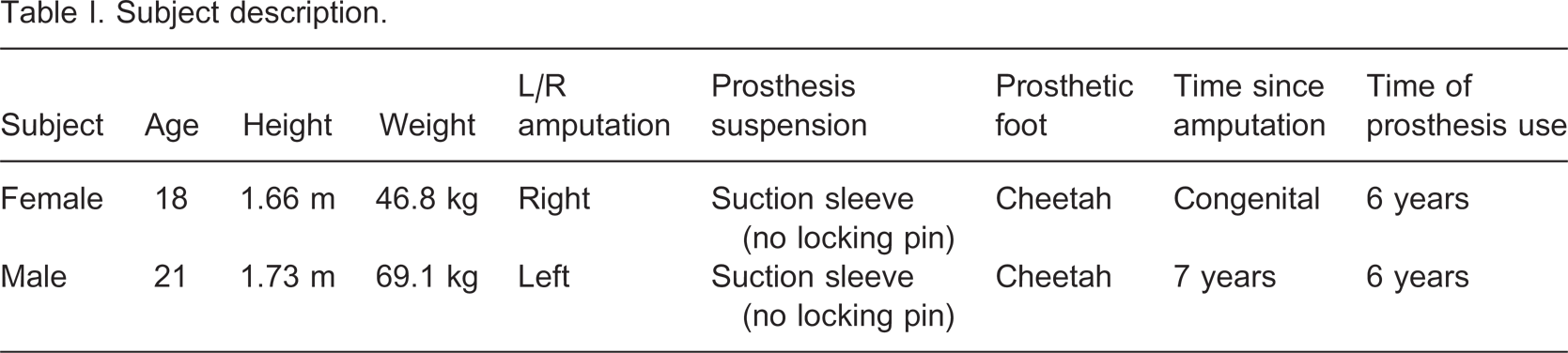
Subjects
Subject description.
Procedure
A pilot study was designed to investigate the performance of transtibial amputee athletes and evaluate the biomechanical changes due to modifications in their prosthetic devices. Each subject ran a total of five trials at 75% of their documented maximum running speed (male: 5.4 m s−1 and female: 3.6 m s−1) and their prosthetic device was uniquely adjusted for each trial. The subject's preferred prosthetic device alignment and stiffness category were considered the ‘baseline’ configuration for each subject; this setting was deemed the ‘neutral’ trial. The stiffness category was varied in two trials by an increase and decrease of a half-category respectively, while the height of the prosthesis was kept constant. Subsequently, when the height was varied in two trials, the neutral stiffness category was used. The height of the prosthetic foot was increased and decreased by 1.27 cm (0.5 inches) for these two trials using a vertical slide adaptor at the foot attachment site on the posterior aspect of the socket. A certified prosthetist was present to facilitate all prosthetic device adjustments.
The subjects were acquainted with the testing procedures and were prepared for data collection. It should be noted here that each subject wore electromyography (EMG) electrodes and 3D reflective markers throughout each of the trials. The procedures for electrode and marker placement and the corresponding data recorded are not relevant in this context and will not be discussed further.
Data collection
Trial capture order.
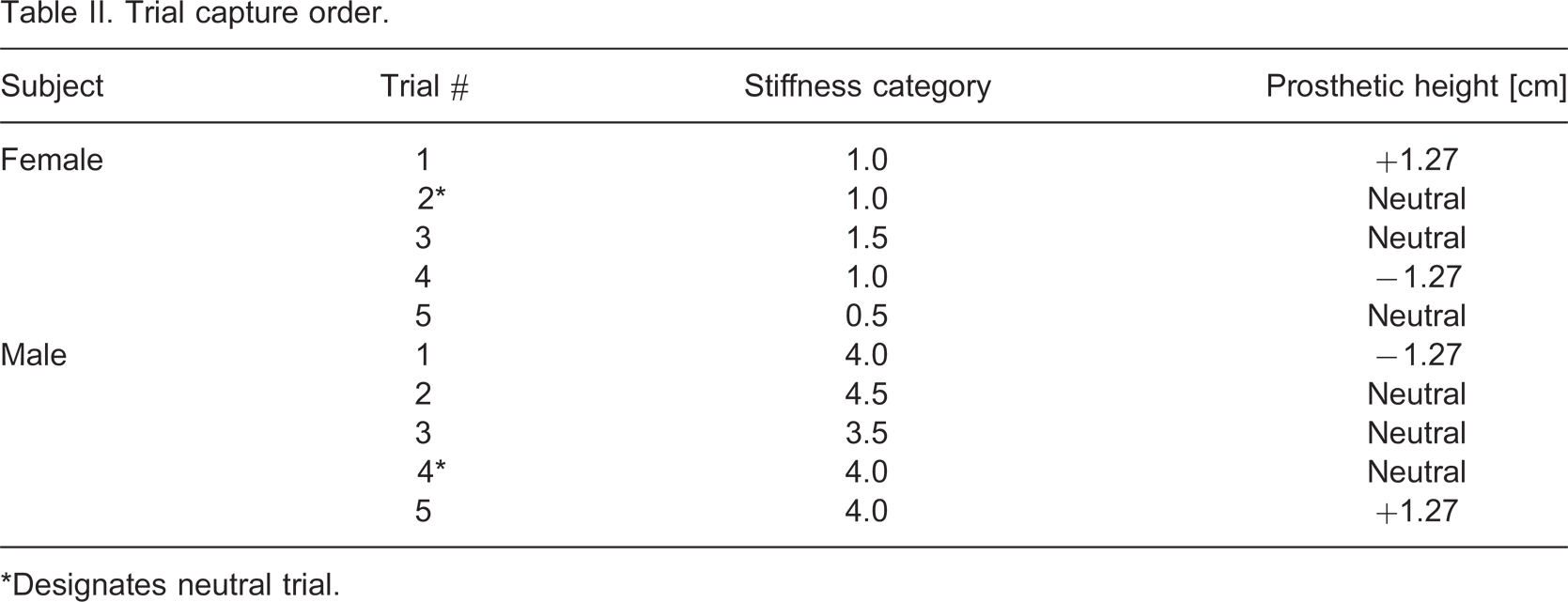
∗Designates neutral trial.
For the prosthetic foot tested, the stiffness category was designated by the manufacturer. The exact stiffness categorization was somewhat arbitrary, but was based on the subject's body weight. The available categories varied from 1–9 over a range of weight from 44–147 kg. Each subject typically used a stiffness category that corresponded to his/her weight range as determined by the manufacturer. In addition to each subject's preferred stiffness foot, two additional feet were obtained from the manufacturer, each a half-category rating above and below the subject's preferred category. The reader should note that stiffness of this prosthetic foot was not quantified in this study and all stiffness comparisons are based solely on the manufacturer's categorization.
Vertical ground reaction force (VGRF) data was collected at 3000 Hz using a Kistler Gaitway instrumented treadmill (Kistler Instrument Corp., New York, USA). Prior to data collection, subjects were given adequate time to run on the treadmill until each felt comfortable. Once the treadmill was placed in the permanent capturing location, the device was leveled and calibrated for speed and force accuracy prior to data collection. Belt speed calibration was verified by measuring the speed of a reflective marker placed on the belt. Force calibration was verified by taking static measurements on each plate with a calibrated weight. Running velocity was determined by the display on the treadmill and verified by transducer output in the Gaitway software (ver. 2.06, build 2013).
The treadmill was programmed prior to data collection to reach the desired speed at a preset, comfortable rate from standstill. The treadmill was initialized and the subject began running until he/she reached the required speed. At this time, simultaneous video capture, EMG, and force plate data collection began for 15 sec. Once data collection was completed, the treadmill speed was reduced and the subject stepped off of the treadmill, signifying a completed trial. The prosthetic device was then adjusted and the subject rested while preparations were made for the next trial.
Spring-mass model
The spring-mass model used in this study (Figure 1) consisted of a point-mass located at the center of mass connected to the ground by a single linear mass-less spring as defined by McMahon and Cheng[23] and shown below as presented by Farley et al.[27] The stiffness of this leg spring, k
leg, is defined as the ratio of the peak vertical ground reaction force (F
peak) to the peak displacement (ΔL
max) of the leg spring:
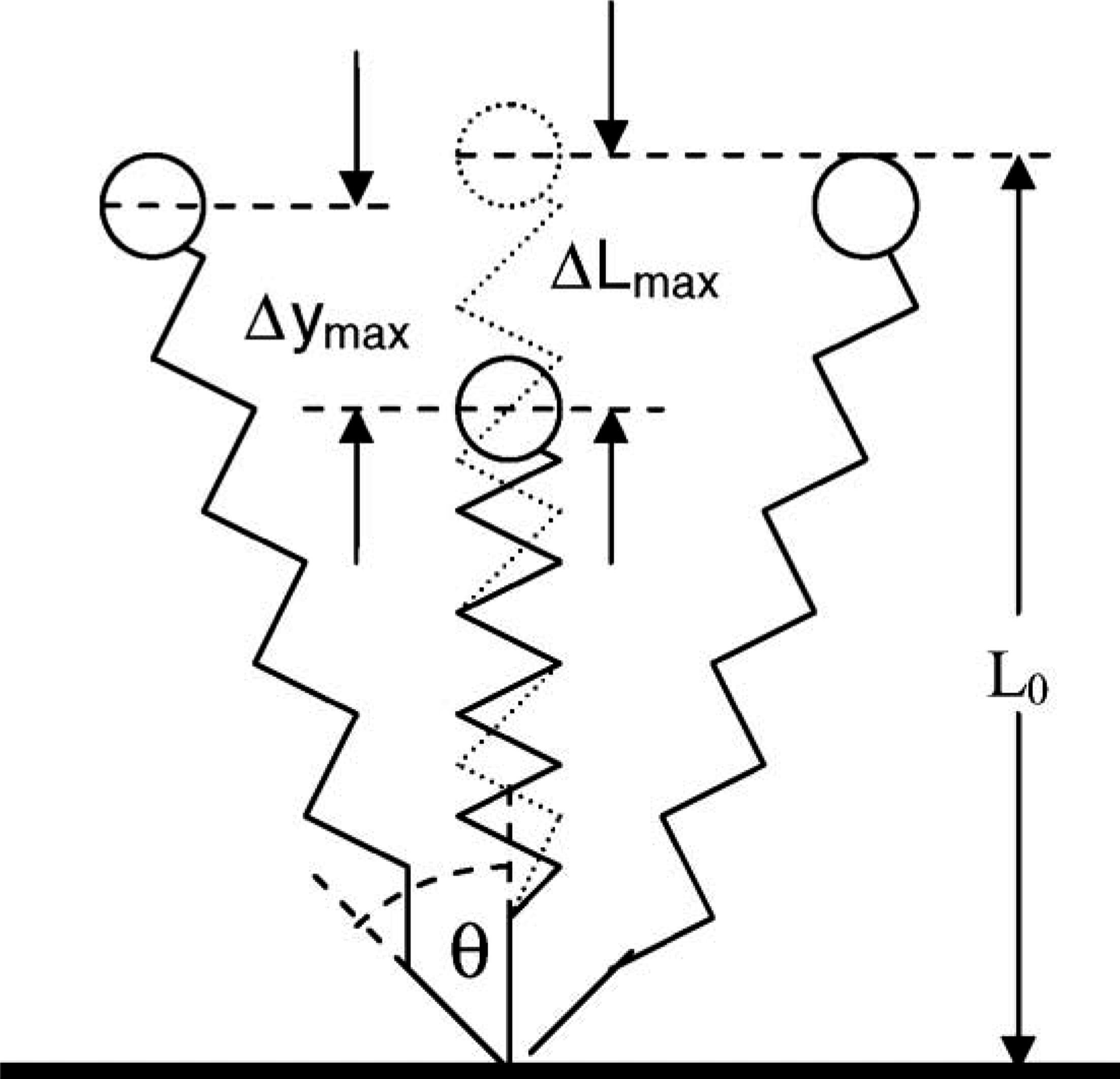
Diagram illustrates the spring-mass model (adapted from Farley and González[22]). L0
designates the initial, unloaded length of the leg, or more specifically, the distance from the surface to the center of mass (COM). ΔL
max represents the maximum change in leg length during contact, while Δy
max describes the maximum vertical displacement of the COM during contact. θ is half of the angle swept by the leg during contact.
The peak vertical ground reaction force (VGRF) occurred simultaneously with the instant of maximal leg compression, ΔL
max. The peak displacement of the leg spring was defined by the peak vertical displacement of the center of mass (Δy
max), the initial length of the leg spring (L
0) at contact and half of the total angle (θ) swept by the leg during contact:

The peak vertical displacement, Δy max, was calculated from the ground reaction force data by twice integrating the vertical acceleration.[34] Synchronized video capture and VGRF force data were collected simultaneously with a VICON 512 motion capture system (Oxford Metrics, UK) consisting of eight cameras during these trials. The initial leg length was determined in each subject by measuring the distance from the center of the hip joint to a reflective marker on the toe at the instant of contact. The location of the hip joint centers were computed by a consistent method between subjects in which motion capture markers placed at the specific knee and pelvic locations were used to estimate each position. The toe markers were placed on each prosthetic foot directly above the approximate location of contact.
The instant of contact was determined from VGRF data (see VGRF procedure in the Data analysis section below) and the contact event was located in the synchronized motion capture data. It is important to note that Δy max describes the vertical displacement of the center of mass, while ΔL max describes the maximum change of leg length as defined by the model.
The total contact time, tc
, for each cycle was determined by computing the difference between the instants of initial contact and toe-off (see Data analysis section). Consequently, the half angle swept by the leg during contact, θ, was determined by computing the inverse sine of the distance traveled in each half of a cycle, u·t
c / 2, divided by the leg length, L0:
The horizontal speed, u, was assumed to remain constant for each cycle. The speed was also assumed constant over within and between trials. Analysis of the speed transducer data for the treadmill verified that the speed did not vary more than 4 cm/sec for either subject over all trials.
The concept of ‘effective vertical stiffness’ describes the resistance of the overall system to vertical motion during contact. Vertical stiffness, k
vert, was defined by the ratio of peak VGRF, F
peak, to the peak vertical displacement of the center of mass, Δy
max:

Symmetry index
Once each these spring-mass variables were computed, they were separated into two categories: ‘sound’ and ‘prosthetic’. A measure of the inter-limb symmetry was then calculated using the symmetry index. The symmetry index (SI) was implemented as follows:[32]

The symmetry index was computed by taking the individual values of Xsound and Xprosthetic for each complete gait cycle. The cycle definition began with the initial contact of the sound limb, was followed by the prosthetic limb, and ended with the next sound limb foot strike. In the event that either foot strike was not recorded in succession to define a cycle, the recorded foot-strikes that would have defined that cycle were disregarded.
It should be noted here that this convention actually describes inter-limb asymmetry. Symmetry is achieved when SI is equal to zero. When SI value is negative, this indicates that the measured value is larger on the prosthetic limb. When the SI value is positive, the value is larger on the sound limb.
Data analysis
Temporal events from the VGRF data were required for spring-mass model computations. The raw VGRF data was filtered with the standard Gaitway software and exported into Microsoft Excel for data reduction. Left and right foot-strike recordings were separated and individual heel-strike, toe-off, and cycle events were calculated. The beginning of each gait cycle was defined by the first frame of the cycle where greater than 7% of the subject's body weight was recorded.[33] The end of stance was defined by the first frame where less than 7% of the subject's body weight was recorded. The end of each cycle was defined as the beginning of the next cycle where greater than 7% of the body weight was recorded (Figure 2).
Representative plot of vertical ground reaction force (VGRF) data. This plot is selected from trial 2 for the female subject. The dashed line represents the 7% threshold where the beginning of the gait cycle is demarcated. The end of the first cycle and beginning of the second cycle begins at the next strike of the ipsilateral limb.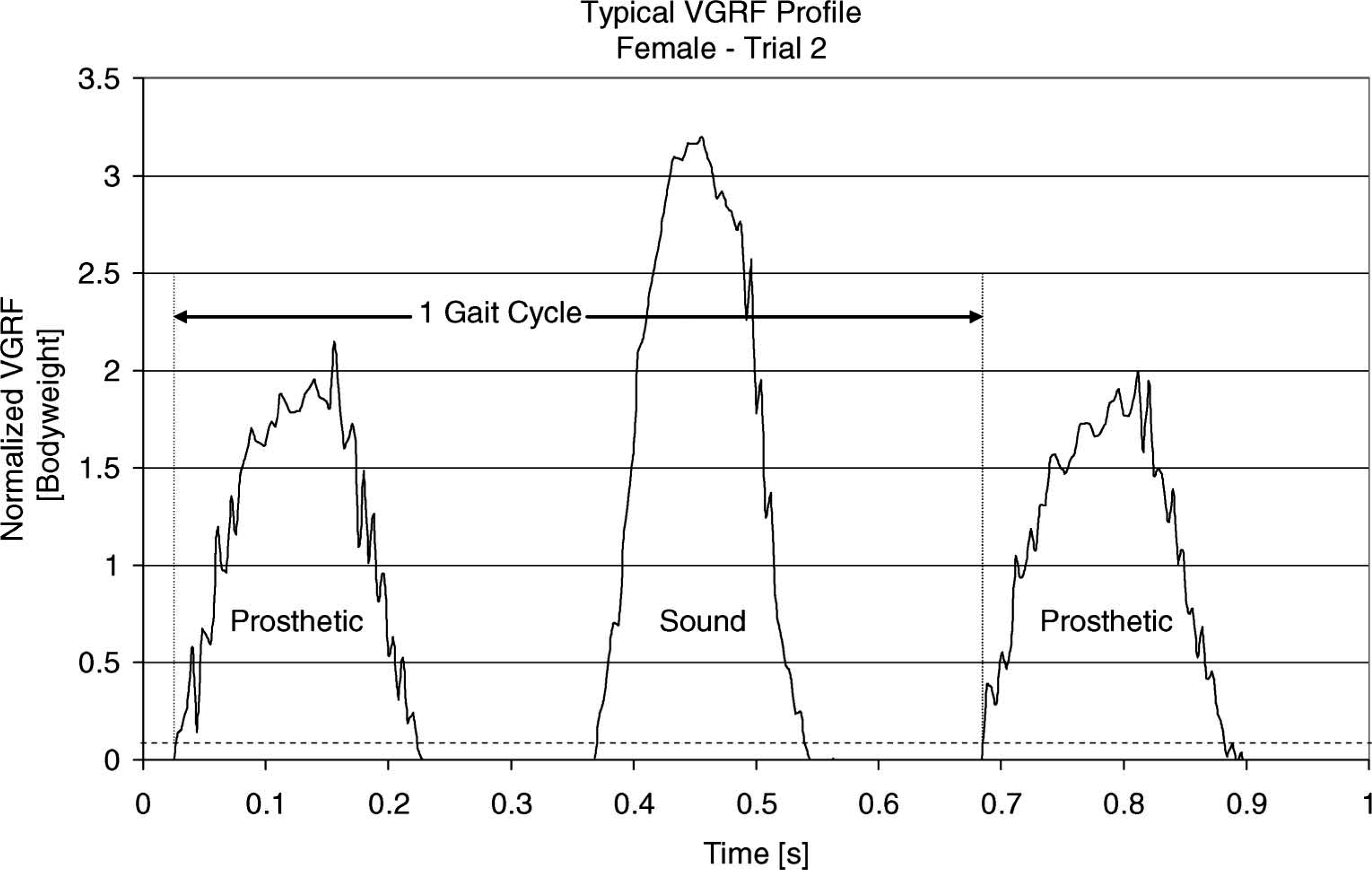
The effects of changes in the prosthetic height and stiffness were investigated by comparing measured spring-mass variables for each subject's sound and prosthetic limbs. This was followed by an analysis of the changes in inter-limb symmetry by comparing the limbs using a symmetry index within a single gait cycle for all trials.
One-way ANOVA tests were conducted for each subject to determine if there were statistically significant differences in the measured spring-mass variables for each limb (‘sound’ and ‘prosthetic’) due to changes in either prosthetic height or stiffness. The number of samples used from each trial in the ANOVA tests was determined by the minimum number of strides recorded in any one trial considered for that comparison. There were no fewer than eight strides for any trial for either subject. One-way ANOVA tests were also conducted for each subject to determine if there were significant inter-limb differences measured for each spring-mass variable (‘Symmetry index’).
Results
Statistically significant differences (p < 0.05) measured in spring-mass variables and symmetry due to changes in prosthetic parameters – male subject.
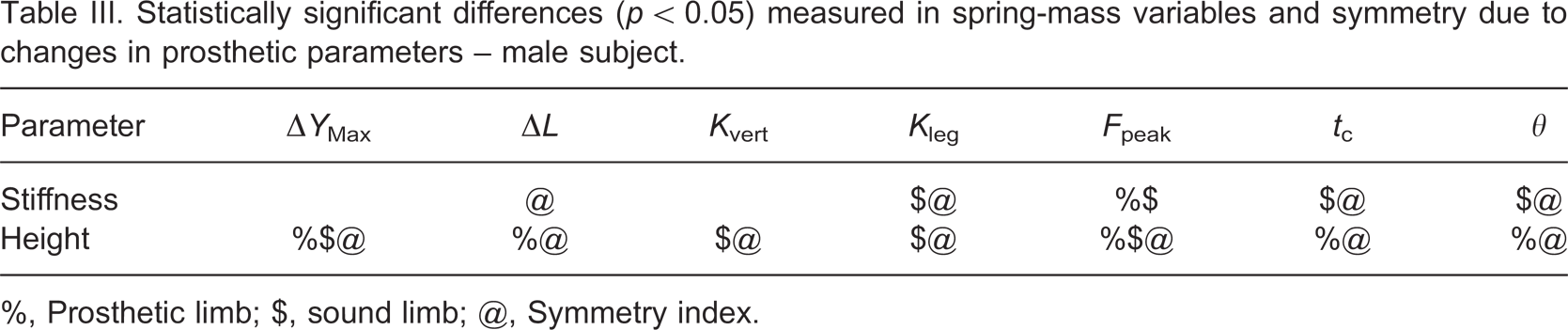
%, Prosthetic limb; $, sound limb; @, Symmetry index.
Statistically significant differences (p < 0.05) measured in spring-mass variables and symmetry due to changes in prosthetic parameters – female subject.
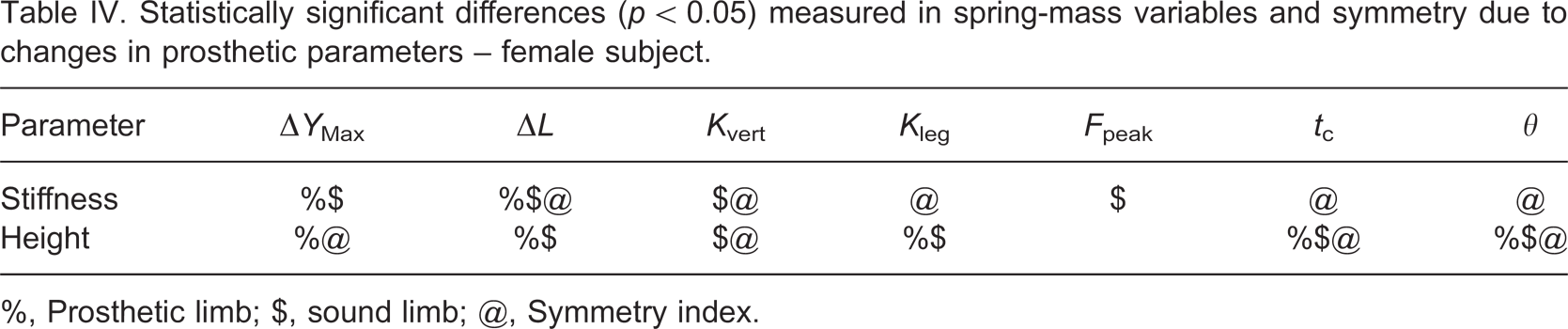
%, Prosthetic limb; $, sound limb; @, Symmetry index.
The effective vertical stiffness (k vert), on both the male and female subject's prosthetic limbs was not significantly affected by any changes in prosthetic height or stiffness. Furthermore, the only significant change in the measured leg stiffness (k leg) on the prosthetic limb was due to prosthetic height changes in the female subject. However, both subjects exhibited significant changes in Δy max, ΔL, t c, and θ due to changes in prosthetic height. While the female subject was able to achieve constant overall stiffness on the prosthetic limb, changes in the prosthetic height were detected in the length and timing parameters of the spring-mass model. The male subject seemed to accommodate the changes in prosthetic stiffness and height by a significant change in peak force (F peak), whereas, on the female subject's prosthetic limb, F peak was unchanged.
On the sound limb, both subjects exhibited significant differences in k vert and k leg due to changes in prosthetic height. The male subject had a significant change in F peak on the sound limb for both prosthetic prescription changes, but the female subject only showed significant differences in the sound limb F peak due to changes in the prosthetic stiffness category.
When comparing symmetry between limbs, both subjects showed significant differences in contact time (t c) and half-angle (θ) symmetry for all changes in prosthetic prescription. The male subject had significant differences for all calculated spring-mass symmetry indices due to changes in prosthetic height. The female subject's inter-limb symmetry was significantly affected in Δy max, k vert, t c, and θ due to changes in prosthetic height. This suggests that changes to the height of the prosthetic device may have resulted in a change in the overall symmetry between limbs for Δy max and k vert in both subjects.
For changes in the prosthetic stiffness, both subjects had significant differences in the observed symmetry of k leg and the change in leg length, ΔL. This indicates that the change in stiffness of the prosthetic device may have resulted in a corresponding change in the overall symmetry between limbs for ΔL and k leg.
Discussion
The measured spring-mass model variables were sensitive to small changes in the height and relative stiffness of the prosthetic device. Additionally, changes in the prosthetic device resulted in significant differences in inter-limb symmetry, quantified by the SI.
Ferris and Farley[30] reported that for subjects running on surfaces with various stiffness levels, the leg stiffness, k leg, was modified to adjust for the new surface stiffness resulting in constant center of mass mechanics, Δy max. In this study, both subjects showed significant changes in the SI of k leg and no significant changes in the SI of Δy max due to changes in the prosthetic device stiffness. The individual spring-mass behavior in each limb was inconsistent between subjects for stiffness changes, but these findings suggest that the subjects may have attempted to preserve the symmetry of Δy max by modifying the symmetry of k leg.
Farley et al.[28] and Farley and Morgenroth[29] concluded that k leg is primarily modulated by changes in ankle stiffness, with no significant changes in knee or hip stiffness. In the current study, the subjects were unable to achieve constant vertical displacement of the center of mass on the prosthetic limb and between limbs when subjected to changes in prosthetic height. If ankle stiffness is, in fact, the primary mechanism for k leg modulation, it is not surprising that transtibial amputees may have difficulty in maintaining constant Δy max and subsequently Δy max symmetry when subjected to changes in prosthetic height or stiffness.
It is not clear whether improved symmetry of kinematic and kinetic biomechanics provides an advantage or disadvantage to amputee gait[12-18] (or able-bodied gait for that matter[34]). In this study the SI was used as a tool to compare spring-mass parameters for amputees. The SI is a powerful measure, in that a single value is used to describe the relative changes in the spring-mass parameters due to changes in the prosthetic device configuration. In some instances, the measured spring-mass parameters were not significantly changed on either the sound or prosthetic limb, but the SI for that parameter was significantly affected. In other instances, this observed phenomenon was reversed. This relative measurement may help to explain the compensatory strategies employed by transtibial amputee runners. An example of this might be an instance where the measured F peak between trials significantly increased in both limbs, but the SI for F peak remained unchanged. This observation would indicate that subject maintained the same level of asymmetry between trials.
While the SI values for individual spring-mass variables are not presented here, the application of a symmetry index explicitly illustrates the relative changes between limbs. It has been suggested that reducing asymmetries in the gait of amputees could be a means to improve prosthetic prescription.[18] Further investigation with a larger and more diverse subject population would provide a better understanding of how spring-mass characteristics are affected by changes to the prosthetic device.
The differences between these subjects should not be ignored. While the changes in prosthetic height and stiffness category were consistent with the manufacturer recommendations between subjects, the influence of these variables with the individuals' height and weight have not been adequately described in the literature. Likewise, the influence of the subjects' gender and cause of amputation and athletic ability has not been determined. Future work should establish baseline standards for prosthetic fitting and alignment that are repeatable to ensure that differences between the adjustable variables are valid.
In an attempt to establish trends for optimization, an increase in the number and magnitude of modifications to prosthetic prescription should be made. These modifications should at least be standardized to each subject's height and body weight to promote comparison between subjects. The number of amputee subjects analyzed should be increased for future research, as well as including a variety of able-bodied subjects of both genders, with varying heights, weights and athletic abilities. Consequently, the differences between amputee and able-bodied locomotion may be better understood.
In future research, the spring-mass model could be modified specifically for use with running prostheses. Additionally, the authors suggest finding the preferred stride frequency of subjects at a given speed, as a method to aid in the selection of the prosthetic device. Stability and control models may be able to predict an ideal stride frequency based on a subject's overall spring-mass characteristics, and the alignment parameters could be iteratively adjusted to achieve this frequency. Future research should also emphasize comparing quantitative results to the amputee's perception and explore the relationship between kinematic and spring-mass model/symmetry parameters in an attempt to identify the most efficient compensatory strategies for amputee running. While not conclusive in this pilot study, the authors hypothesize that there may be a relationship between a subject's prosthetic prescription and his/her ability to achieve maximum possible symmetry of spring-mass parameters.
Conclusions
Prosthetic height and stiffness category is believed to influence performance in transtibial amputee runners. The application of a spring-mass model identified differences in lower inter-limb symmetry when prosthetic stiffness categories was altered in both runners. Changes in prosthetic height influenced inter-symmetry with one of the two runners. Although a clinically friendly method of optimizing running prosthesis height and stiffness has yet to be developed, the spring-mass model used with a symmetry index is a simple, robust method for analysis of amputee running biomechanics. Moreover, it appears that prosthetic height and stiffness category does affect running performance suggesting the need for further investigations to better understand how clinicians can modify these variables to optimize function.
Footnotes
Acknowledgements
The authors would like to thank Neil Spielholz, PhD, PT and prosthetists Alan Finnieston, CPO LPO and Adam Finnieston, CPO LPO for providing support in all data collection. We would also like to thank Mr. Moataz Eltoukhy for his assistance in data reduction and statistical analysis. Lastly, we would like to acknowledge Össur for providing all the prosthetic devices to perform the needed experiments.