
Abstract
Background:
The amputee population is elderly, has significant medical co-morbidities and perioperative mortality leading to high financial implications. Commonly used outcomes in the literature are survival, prosthetic use and mobility.
Objectives:
Our study aims to share our 12-year experience of amputee care, concentrating on perioperative mortality and patient rehabilitation.
Study Design:
Observational study in the form of a retrospective case series.
Methods:
In total, 130 amputations, performed between January 1998 and December 2009, were followed up for a mean of three and a half years and analyzed for demographics, vascular history, operation details, prosthetic use, mobility and mortality.
Results:
The population was 59.2% male, had a mean age of 73 and the most common indication for amputation was critical ischaemia (78.5%). The average length of acute inpatient stay was 63 days with a 30-day mortality rate of 15.3% and inpatient mortality of 29.3%. In total, 63.3% of patients were issued with a prosthesis with 48.2% of all patients achieving at least indoor mobility, transtibial (49.9%) rehabilitated better than transfemoral amputees (24.3%).
Conclusions:
Our data support the urgent need for action to improve perioperative mortality in the amputee population, with the added advantage of reducing its financial impact.
Clinical relevance
Our study gives an overview of the clinical journey taken by a 12-year amputee population. By following this cohort from initial procedure through to rehabilitation or mortality we provide the reader with a valuable insight into the difficulties of managing this population and the likely outcomes for these patients.
Background
Major lower limb amputation, defined as either above or below knee amputation, is a commonly performed procedure for peripheral vascular disease with an estimated 30,000–50,000 carried out annually in the USA. 1 In England, an estimated 49.487 non-traumatic lower extremity amputations were performed over a five-year period from 2004 to 2008 2 with 4,574 amputees being referred to a UK prosthetic unit in the year 2006–2007. 3 Critical limb ischaemia (CLI) is the most common indication for amputation 4 and the majority of patients (60–70%) have undergone previous revascularization attempts.5,6 This population tends to be elderly with significant medical co-morbidities with diabetes (80.6%), ischaemic heart disease (66.2%) and hypertension (68.2%) being the most common.4,6
CLI patients suffer significant associated morbidity and mortality leading to considerable consumption of health and social care resources. With the increasing financial pressures on the NHS, the cost-effectiveness of treatment has become more important and is regularly scored as an outcome measure for surgery. The optimum management of CLI remains unclear and although some studies claim that primary amputation is a cost-effective solution,7,8 the majority recommend an aggressive approach to reconstruction on economic grounds.9–11 One such UK study looked prospectively at the cost of treatment over 12 months of patients undergoing revascularization (£3,970), angioplasty (£6,611), reconstruction (£6,766) and primary amputation (£10,162). 12 The initial cost of arterial reconstruction is offset by more rapid rehabilitation compared to the long-term support an amputee requires.13,14 This higher cost of primary amputation may be related to longer inpatient stays, need for more home support and time spent in institutional care. 12
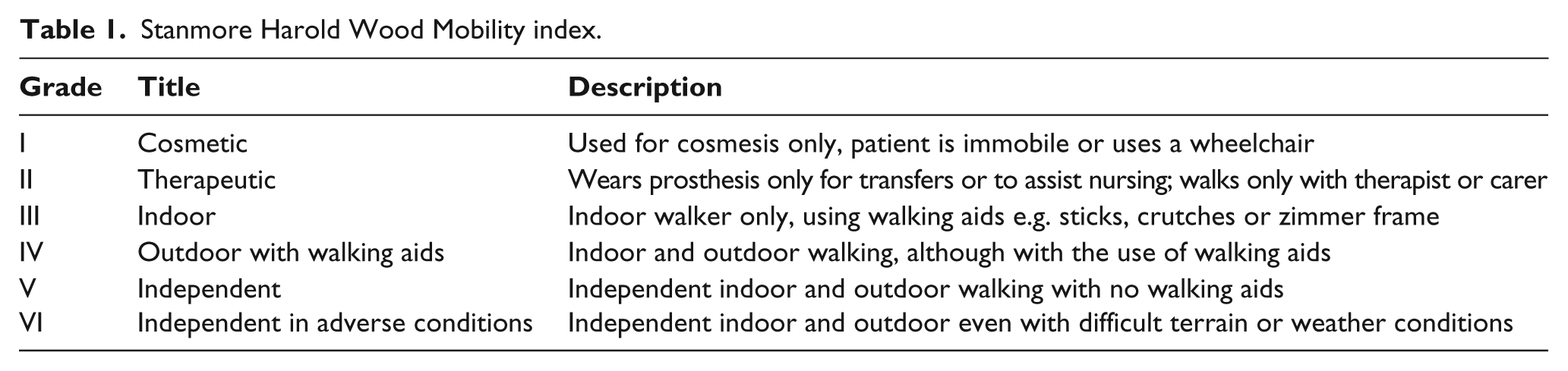
Becoming an amputee can have a major effect on a patients’ quality of life with potential consequences for mobility, social functioning, emotional status and pain level. Primary amputees have been shown to have significantly worse mobility and performance with activities of daily living than those who undergo limb salvage procedures. 15 Literature has shown mobility to singularly have a significant effect on quality of life 16 which has resulted in it becoming the focus for patient rehabilitation and outcome measures. Many mobility scores exist with our rehabilitation centre using the Stanmore Harold Wood Mobility index (see Table 1). However the overall aim of rehabilitation is to restore and preserve maximum independence for the longest period possible and measuring a patient’s mobility only partly reflects this.
Stanmore Harold Wood Mobility index.
The provision of a prosthesis is imperative to successful patient mobility post-amputation and studies have shown 81–85% of patients are supplied with one.4,17 With prosthesis, the indoor mobility ranges from 28 to 79% and outdoor mobility from 21 to 60%.18,19 The level of amputation influences patient mobility with transtibial shown to expend less energy when mobilizing than transfemoral amputees.18,20 This is shown in improved indoor (16–60%) and outdoor (9–50%) mobility in transtibial amputees compared to transfemoral amputees (5–50%) and (4–25%) respectively.21,22 When the decision for level of amputation is taken, these figures should be taken into account with preservation of the knee joint giving the best opportunity for successful mobility and rehabilitation.
Patient mortality is a commonly used end point when analyzing the amputee population with the estimated 30-day perioperative mortality ranging from 9 to 17%.23,24 The transfemoral subgroup have a lower one- and five-year survival rate of 50.6% and 22.5% compared to transtibials 74.5% and 37.8% respectively. 6 A recent Vascular Society publication A quality improvement framework for major amputation surgery states that the current perioperative mortality rates for amputations are ‘unacceptable’ and advises changes with the aim to reduce perioperative mortality rate to less than 5% by 2015.
Methods
Using a computerized theatre system all transtibial and transfemoral amputations performed under the care of our lead consultant (DJH) from January 1998 to December 2009 were identified retrospectively. As no intervention was implemented and patients not approached directly, ethical approval and informed consent were not sought or obtained.
This system provided data on patient age, previous vascular surgery, further surgery and dates for admission, procedure and discharge. A separate computerized system was used to obtain information relating to procedure performed, indications, previous revascularization attempts, patient survival and co-morbidities through operation notes, discharge letters, clinic letters and radiology reports. Patients were followed up until they were deceased, discharged from follow up or until April 2011. The mean follow-up period for each individual was three and a half years.
Of these patients, those referred to our separate amputee rehabilitation clinic on discharge were identified and their rehabilitation notes obtained and analyzed for prosthetic provision, best post-procedure mobility achieved using the Stanmore Harold Wood Mobility index and length of follow up.
Results
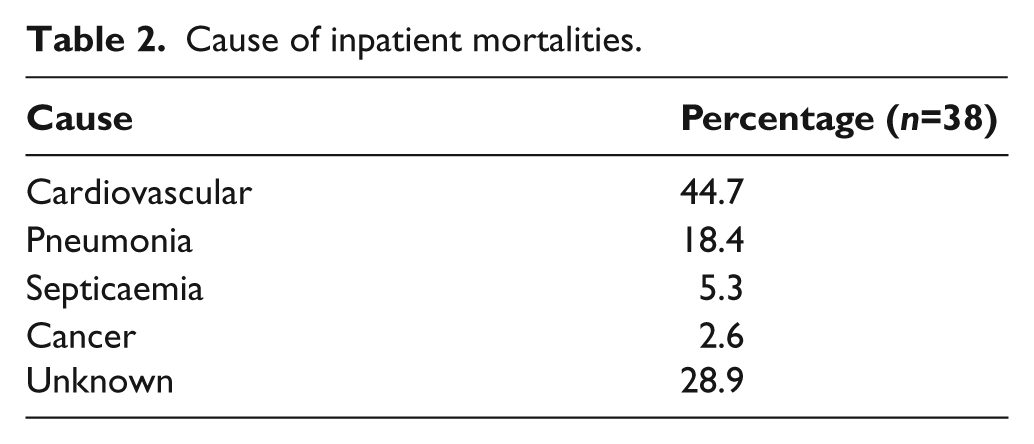
In total, 122 patients underwent a major lower limb amputation during the study period, with eight of these patients having bilateral procedures. Of the amputees 59.2% were male with a mean age of 73 years (range of 23–92). The average length of acute hospitalization was 63 days with a 30-day mortality rate of 15.3% and an overall inpatient mortality of 29.3%. The cause of inpatient mortality is shown in Table 2. At the end of the follow-up period only 29.2% of patients survived, this is illustrated by the Kaplan Meier Curve in Figure 1.
Cause of inpatient mortalities.
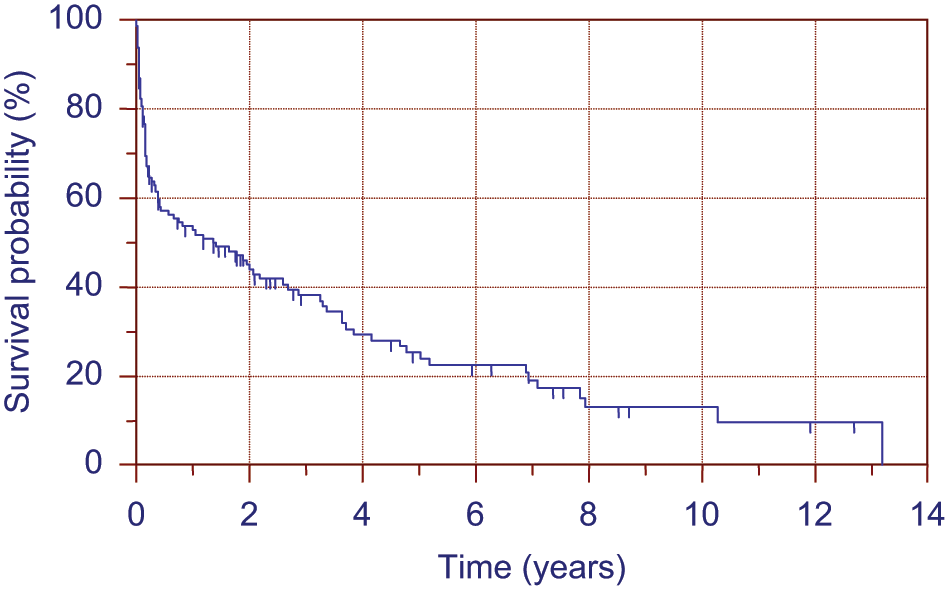
Kaplan-Meier Survival Curve for all amputees.
Of our sample population, 79 were referred to be seen at the separate rehabilitation centre for assessment. Of the 51 patients not referred, 40 died as an inpatient with only 11 being discharged from acute care without follow up with the rehabilitation service.
We analyzed the 79 patients referred for rehabilitation further with 65.8% being male with an average age of 69.9 years (range 23 to 91). In total, 65.8% had previously undergone an attempted revascularization procedure; 53.2% angioplasty, 39.2% bypass grafting and 13.6% either a failed embolectomy or thrombectomy. The indications for amputations were critical ischaemia (78.5%), infected ulcer (15.2%), fixed flexion deformity (2.5%), osteomyelitis (1.3%), frostbite (1.3%) and post-compartment syndrome (1.3%). This population had significant co-morbidities with the most common being diabetes mellitus (46.8%), hypertension (44.3%), ischaemic heart disease (36.7%), atrial fibrillation (19%), cerebrovascular accident (17.7%), dialysis (5.1%) and unknown history (2.5%).
The majority of amputations occurred at the transtibial level (58.2 %). The post-operative complication rate was 27.8% with 6.3% suffering from a wound infection, 8.9% requiring same level stump revision and 12.7% conversion of stump to a higher level. When looking solely at the 46 patients who had a below knee amputation, 21.7% of these required conversion to an above knee amputation.
In total, 63.3% of patients were issued with a prosthesis with the mean time till delivery being 182 days. Of the remainder, 21.5% were deemed unsuitable, 3.8% declined and 11.4% died prior to assessment. A higher proportion of below knee amputees (82.6%) compared to above (36.4%) were issued with a prosthesis.
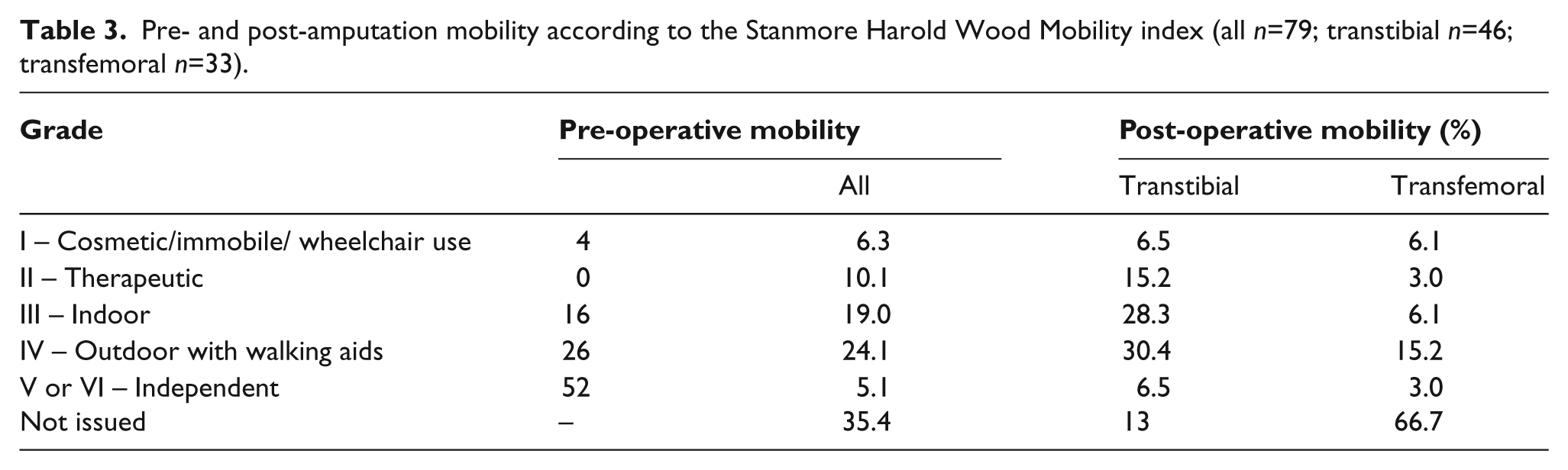
The Stanmore Harold Wood Mobility Index was used at our rehabilitation centre to measure patient’s progress with mobility (Table 3)
Pre- and post-amputation mobility according to the Stanmore Harold Wood Mobility index (all n=79; transtibial n=46; transfemoral n=33).
Discussion
We have presented an overview of the clinical journey taken by 122 amputees from procedure through to rehabilitation and mortality. We have highlighted both the high input these patients require as an inpatient perioperatively and the long-term rehabilitation and support that they require after. Differences in our population demographics from other studies may partly be explained by our patients all being under the care of a vascular consultant. This may have affected the patient age, co-morbidities and indication for amputation.
Our 30-day mortality rate of 15.3% and total inpatient mortality rate of 29.3% provides further evidence that amputees are an at-risk population perioperatively. Differences with US 30-day mortality figures of 8.6% and 10.4%6,23 may be explained through differences in population and the healthcare systems with patients remaining as acute inpatients for longer in the UK. The National Vascular Society of Great Britain and Ireland quotes figures for UK perioperative mortality from the National Vascular Database of 9% and the Hospital Episode Statistics of 17%. 24 Although these figures are useful to compare against, the National Vascular Database is currently optional to complete and the lower figure produced may be biased by those trusts producing favourable data submitting information more readily. The care of the amputee population is being targeted for improvement with the National Vascular Society of Great Britain and Ireland seeking to reduce perioperative mortality to less than 5% by 2015 with the production of its guidance Quality Improvement Framework for Major Amputation Surgery. 24
Our centre provides a good rehabilitation service with comparable levels of prosthesis provision and usage to other studies. 23 The service also managed to provide long-term support for patients with the mean follow-up period being over three years. Reports in the literature suggest a wide variation in mobility outcome post-amputation with indoor mobility from 28 to 79% and outdoor mobility from 21 to 60%.18,19 This disparity may be partly produced by differences in patient populations, rehabilitation services, outcome measures and timing of these measurements. Table 4 shows that our data are comparable to another UK study that used the Stanmore Harold Wood Mobility index. When comparing our post-operative mobility with US data we also have good results; grade I and II our 51.4% versus 51%, grade III 19% versus 28%, grade IV, V and VI 29.2% versus 21%. 23
Our post-operative mobility compared to another UK centre, including transtibial and transfemoral subgroups.
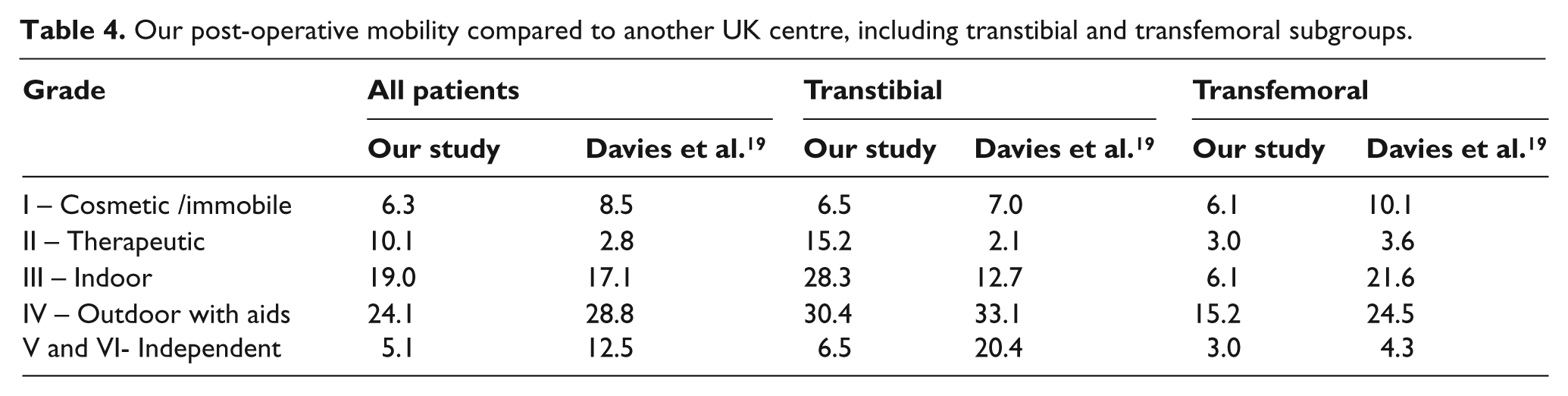
Our data support patients with below knee amputations achieving a higher level of mobility than patients with above knee amputations (see Table 4). This supports previous studies that show transtibial prosthetic users expend less energy,18–20 although the tendency of transfemoral amputees to be more medically unfit and have less rehabilitation potential is a possible confounding factor. This highlights the importance of maintaining the knee joint if feasible to aid the long-term mobility of the patient. Our initial rate of below knee amputation (58.2%) was higher than previous US and UK studies, 54.7% and 50.5% respectively.21,23 During the follow-up period our 21.7% conversion rate to transfemoral amputations was higher than other centres, 9.4 to 19%.5,23,25 This higher complication rate may partly explain the prolonged mean stay at our centre. 4
We could reason that an initial poor or unrealistic choice of amputation level reflected by our higher initial proportion of transtibial amputations may have led to more revisions. The decision of whether a transtibial amputation is achievable is not simple and relies on the surgeon’s ability to predict stump healing. Although the traditional method of clinical assessment at the time of surgery may be useful in expert hands, evidence suggests that factors such as poor skin edge bleeding or absent pulses are not predictive of healing. 26 Information gained from preoperative angiograms has been seen by some authors to be unhelpful, 27 while others maintain that a patent profunda femoris is paramount for successful healing after a transtibial amputation. 28 Both the use of doppler produced segmental pressures29,30 and transcutaneous oxygen pressure have received much support in predicting stump healing31,32 but these were not used at our centre.
The amputee population has been shown to be a strain on NHS resources,9-12 with the large proportion being used to fund protracted inpatient stay, rehabilitation and long-term care.12,33 Our study highlights this problem with the average stay over two months. In addition, the majority are involved in the rehabilitation process with prosthesis provision and follow up for a mean of three and a half years which again is costly. As has been shown by other centres, if the care of these patients is targeted then efficiency cuts can be made. 34 This proactive management may allow patient transfer from acute hospital beds to be expedited and has the potential to save a significant amount of resources. The debate of when to offer primary amputation will continue and although recent evidence suggests that attempts at limb salvage are economical,8-10 there is a subgroup of patients where these measures fail and further intervention raises the cost of care above primary amputation.
Conclusion
Perioperative mortality in the amputee population is unacceptably high with our data showing a 30-day mortality of 15.3% and an inpatient mortality rate at 29.3%. Action needs to be taken to improve these figures and target an at-risk population, we believe the steps suggested by the National Vascular Society in their Quality Improvement Framework need implementation. In addition the financial cost of amputation is high with long-term support and rehabilitation needed, current practice offers scope to improve efficiency and significantly reduce this impact.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.