
Abstract
Purpose:
This study aims to derive a formula to predict post-operative height increment in Lenke 1 and Lenke 2 adolescent idiopathic scoliosis (AIS) patients using preoperative radiological parameters.
Methods:
This study involved 70 consecutive Lenke 1 and 2 AIS patients who underwent scoliosis correction with alternate-level pedicle screw instrumentation. Preoperative parameters that were measured included main thoracic (MT) Cobb angle, proximal thoracic (PT) Cobb angle, lumbar Cobb angle as well as thoracic kyphosis. Side-bending flexibility (SBF) and fulcrum-bending flexibility (FBF) were derived from the measurements. Preoperative height and post-operative height increment was measured by an independent observer using a standardized method.
Results:
MT Cobb angle and FB Cobb angle were significant predictors (p < 0.001) of height increment from multiple linear regression analysis (R = 0.784, R 2 = 0.615). PT Cobb angle, lumbar, SB Cobb angle, preoperative height and number of fused segment were not significant predictors for the height increment based on the multivariable analysis. Increase in post-operative height could be calculated by the formula: Increase in height (cm) = (0.09 × preoperative MT Cobb angle) – (0.04 x FB Cobb angle) – 0.5.
Conclusion:
The proposed formula of increase in height (cm) = (0.09 × preoperative MT Cobb angle) − (0.04 × FB Cobb angle) – 0.5 could predict post-operative height gain to within 5 mm accuracy in 51% of patients, within 10 mm in 70% and within 15 mm in 86% of patients.
Keywords
Introduction
Curve progression in adolescent idiopathic scoliosis (AIS) will result in height loss in the spinal deformity. 1 One of the main concerns of parents and patients is the effect of spinal fusion on the height of the patients. 2 –5 Although it is known that scoliosis correction surgery will result in the lengthening of the spinal column height, there is little evidence available to quantitatively predict the amount of height gain post-operatively. Several formulas have been proposed by various authors to determine the increase in height after scoliosis correction. 6 –9 However, these formulas are based on a combination of preoperative and post-operative radiological parameters. Using these formulas, the increase in height could only be determined after the surgery. This would limit the clinical use of such formulas. To our knowledge, no study has reported on the prediction of height after scoliosis correction by using preoperative parameters. Therefore, the purpose of this study was to identify preoperative radiological parameters that are predictors of height increment in Lenke 1 and 2 AIS patients who had undergone selective thoracic fusion.
Materials and methods
This is a prospective study involving 70 consecutive Lenke 1 and 2 AIS patients (8 males and 62 females) who underwent scoliosis correction with alternate-level pedicle screw instrumentation. The study was carried out from June 2012 to May 2014. This study obtained approval from the institutional ethical board. The objective of the study was to derive a formula to predict post-operative height increment in Lenke 1 and Lenke 2 AIS patients using preoperative radiological parameters. There were 44 Lenke 1 and 26 Lenke 2 AIS patients. The mean age of the patients was 16.3 ± 6.6 years.
Patient demographics were recorded. All patients underwent anteroposterior (AP) and lateral standing whole spine radiographs, lower limb axis radiographs, supine side-bending (SB) as well as fulcrum-bending (FB) radiographs. Preoperative parameters that were measured included main thoracic (MT) Cobb angle, proximal thoracic (PT) Cobb angle, lumbar Cobb angle as well as thoracic kyphosis. The sagittal profile and lumbar modifier of the patients were also determined as recommended by Lenke classification. Side-bending flexibility (SBF) and fulcrum-bending flexibility (FBF) were derived from the measurements based on the formula stated in Figure 1. Preoperative height of the patient was measured.

Formula to calculate SBF, FBF and correction rate. SBF: side-bending flexibility; FBF: fulcrum-bending flexibility.
All patients underwent selective thoracic fusion using alternate-level pedicle screw configuration. Selection of the lower instrumented vertebra was the last vertebra significantly touched by the central sacral vertical line. Selection of the upper-instrumented vertebrae (UIV) was guided by the cervical supine SB film. 10 Our aim in the selection of the UIV was to have an optimal UIV tilt angle of 10° or less. This was determined preoperatively from the cervical supine SB film. 10,11 Further confirmation of the correct UIV tilt was determined intraoperatively using a T-bar method. Four pedicle screws were inserted at consecutive levels as base anchors and four pedicle screws as proximal anchors. Alternate-level paired screws were inserted in between (Figure 2). Radical facet resection was performed to increase the spine flexibility as well as to facilitate spinal fusion. Reduction was performed using translation method as well as direct vertebral rotation. Fusion was augmented using autogenous local bone graft obtained from spinous processes, transverse processes and decorticated lamina of each vertebra. Post-operatively, patients underwent standing AP and lateral whole spine radiographs. Radiological parameters were measured on picture archiving and communications system (Centricity PACs, version 5.0, GE Healthcare, Chicago, Illinois, USA).

Case example of a Lenke 1AN patient with a preoperative standing main thoracic Cobb angle of 53°, fulcrum-bending MT Cobb angle of 10°. Post-operative image showing pedicle screw construct and standing MT Cobb angle of 9°. Predicted height increment was 3.8 cm using the multiple linear regression model (height increment = (0.09 × preoperative MT Cobb angle) − (0.04 × FB Cobb angle) − 0.5). Measured height increment was 3.6 cm. MT: Main thoracic; FB: Fulcrum bending.
Post-operative parameters that were documented included MT Cobb angle, PT Cobb angle and lumbar Cobb angle. The correction rate was then calculated based on the post-operative radiological measurements. The number of fused levels was also included in the analysis. Patient’s height increment after the surgery was measured using the technique described below (Figure 3). The same assessor carried out the height measurement for each patient. To increase the accuracy of the height measurement, the preoperative and post-operative heights were marked on a piece of paper prior to measurement. A square block was used to make sure the marking was perpendicular to the vertical axis. Measurements were made to the closest 1 mm. The interrater reliability of the height measurements was determined using the intraclass correlation coefficient.
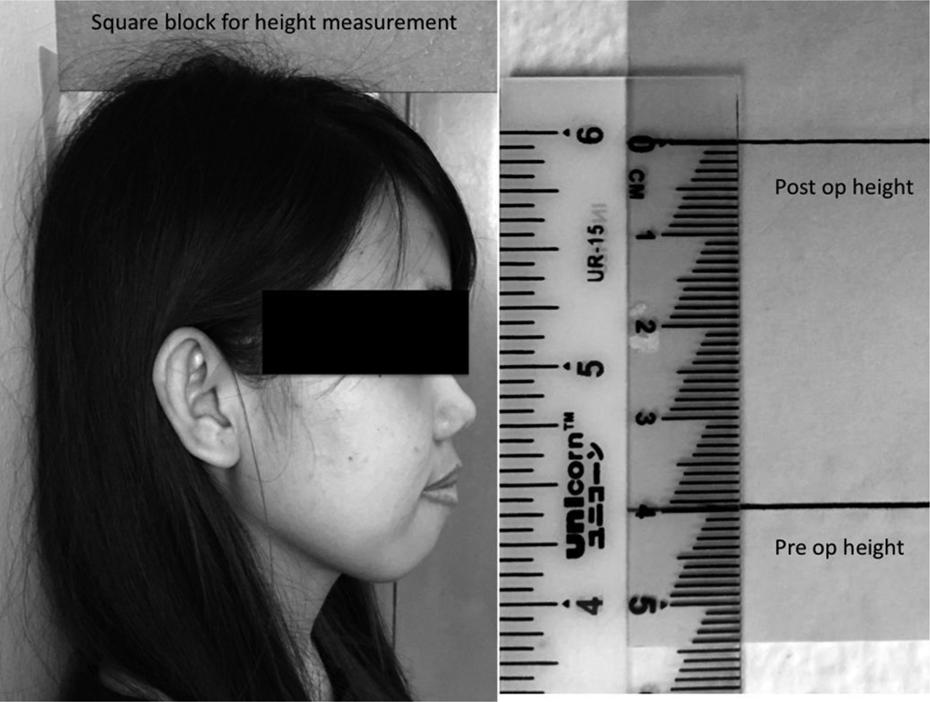
Technique of measuring the height increment pre- and post-operatively.
All the data were analysed using the software Statistical Package for the Social Sciences (SPSS, version 16.0). Paired t-test was used for comparison of means. Simple linear regression was utilized to determine any significant predictors for the height increment from the radiological measurements. A multiple linear regression model was used to find the best predictor that could be used to predict height increment using preoperative parameters. An α value of 0.05 was used to define statistical significance.
Results
The mean preoperative Cobb angle for the MT, PT and lumbar curve was 69.3 ± 21.8°, 36.2 ± 15.7° and 39.9 ± 13.4°, respectively. The MT curve showed an SBF and FBF of 52.8 ± 13.9% and 58.2 ± 16.6%, respectively, with significant differences between Lenke 1 and 2 curves. There was also significant difference in the level of the UIV for Lenke 1 and Lenke 2 curves. About 72.7% of patients had fusion extended to T3 in Lenke 1 curves compared to 76.9% of patients having the UIV at T2 in Lenke 2 curves (p = 0.000). Other preoperative parameters are shown in Table 1. The mean of preoperative height was 157.2 ± 7.8 cm. Table 2 depicts the post-operative parameters and clinical parameters of patients. Intraclass correlation coefficient showed that there was a strong agreement between the raters (0.99, p = 0.001) when measuring the preoperative and post-operative heights.
Patient demographics and preoperative radiological and clinical parameters.

MT: main thoracic; PT: proximal thoracic; MT SB: main thoracic side bending; PT SB: proximal thoracic side bending; UIV: upper-instrumented vertebrae.
Post-operative radiological parameters and clinical measurement.

MT: main thoracic; PT: proximal thoracic.
The post-operative Cobb angle for the MT and PT Cobb was 23.4 ± 12.9° and 16.6 ± 9.3°, respectively, with a correction rate of 66.4 ± 12.5% and 54.2 ± 16.5%. The mean post-operative height was 161.7 ± 7.9 cm and the mean height increment was 4.52 ± 1.6 cm. Comparison between Lenke 1 and 2 curves showed significant differences in terms of post-operative MT and PT Cobb angle, MT correction rate, number of fused level and post-operative height increment (Table 2). The post-operative MT and PT Cobb angle was higher in Lenke 2 curves. The number of fused levels for Lenke 1 curves was 9.9 ± 1.4 and for Lenke 2 curves, it was 11.6 ± 1.7 (p = 0.001). There was a higher correction rate for MT curve in Lenke 1 curves with a correction rate of 69.1 ± 10.7%. However, the correction rate for PT curve was similar in Lenke 1 and Lenke 2 curves (Table 2). The height increment was also higher in Lenke 2 curves. From the radiological analysis, the mean preoperative Cobb was analyzed.
Simple linear regression of the preoperative parameters
In simple linear regression analysis (Table 3), PT, MT, lumbar, SB, FB Cobb angles, preoperative height and number of fused segment were analysed. From the analysis, some of the variables of the preoperative radiological measurements were significant predictors (p < 0.05) for the height increment. Cobb angle for the main thoracic curve measured from the standing, SB and FB radiographs were the strongest predictors (p = 0.001) for height increment with an r value of 0.721, 0.563 and 0.544, respectively. Other variables that were significant predictors for height increment were lumbar Cobb angle from the standing radiographs (p = 0.002), number of fused segment (p = 0.001) and Cobb angle of PT from standing and SB radiographs (p = 0.001). However, preoperative height (p = 0.783) and the lumbar Cobb angle from the SB radiographs (p = 0.249) were not significant predictors for height increment.
Simple linear regression analysis of the preoperative parameters (n = 70).

CI: confidence interval; MT: main thoracic; PT: proximal thoracic; β = coefficient regression.
aSignificant predictor when p < 0.05.
Height increment prediction from multiple linear regressions
The analysis was then continued with multiple linear regression method in order to choose the best predictor for the height increment. Table 4 shows the outcome of the analysis, and the best predictor for the height increment was determined (p < 0.05).
Multiple linear regression analysis for independent variables that are predictors of the height increment.a
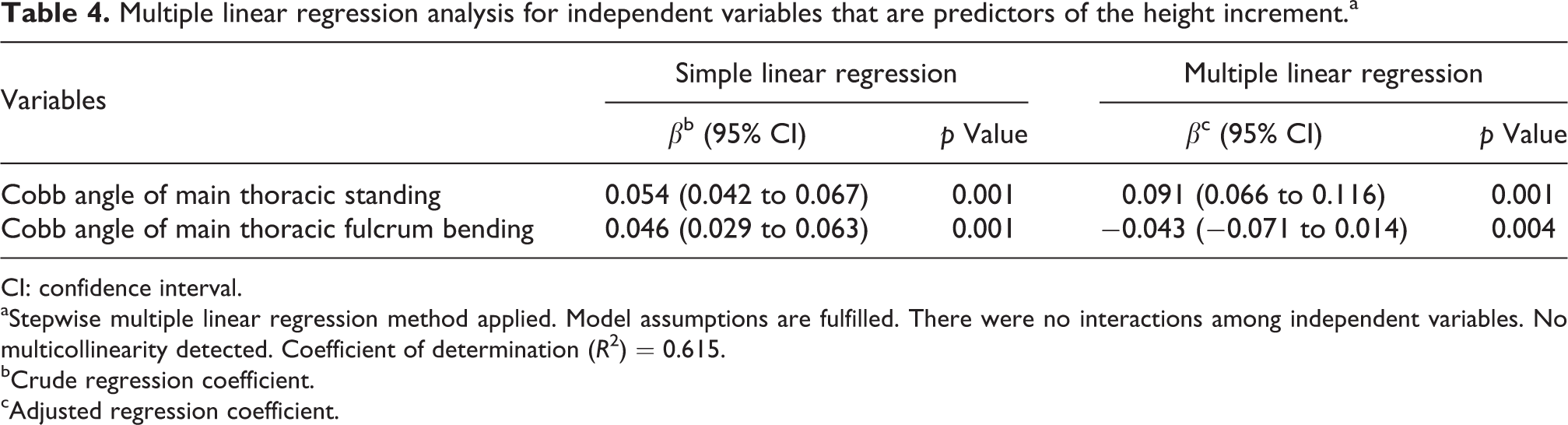
CI: confidence interval.
aStepwise multiple linear regression method applied. Model assumptions are fulfilled. There were no interactions among independent variables. No multicollinearity detected. Coefficient of determination (R 2) = 0.615.
bCrude regression coefficient.
cAdjusted regression coefficient.
Based on the multiple linear regression model, the best predictor for the height increment was chosen. Multivariable linear regression demonstrated that Cobb angle of MT standing (p = 0.001) and Cobb angle MT FB (p = 0.004) were significant predictors of height gain (R 2 = 0.615). The equation describing this multivariable relationship is as follows: increase in height in centimetres (cm) = (0.09 × preoperative MT Cobb angle) − (0.04 × FB Cobb angle) − 0.5.
The other variables were not significant predictors for the height increment based on the multivariable analysis. Thus, all these variables were excluded in the equation. The formula was again applied to the same data to compare the accuracy and the difference between the observed value and the predicted value. Based on this result, we found that 51.4% of the overall data could predict the height with a difference of less than 5 mm while 70.0% could predict the height with a difference of less than 10 mm. Meanwhile, 85.7% from the overall data could predict the height with a difference within 15 mm.
Discussion
The primary indication for scoliosis correction is for prevention of curve progression. 12 However, cosmesis is a strong motivation for both parents as well as patients to undergo surgery. This could be contributed by a higher prevalence of AIS among females. 13 –15 Bridwell et al. reported that cosmesis ranked second as the reason for surgery among both parents and patients. 16 Patients’ perception of their body image affects their psychosocial health as scoliosis patients have been shown to have lower scores in various quality-of-life questionnaires compared to healthy adolescents. 17,18
Patients will closely observe their own physical appearance and make a comparison with adolescents without scoliosis in terms of negative body image, body shape and body size. 2 This will lead them to unhappier lives, more physical complaints, lower self-esteem and higher rate of depression. 19 Thus, the cosmesis of the back, shoulder and the straight standing stature after surgery are among the factors affecting patients’ satisfaction in scoliosis surgery. 20 Another physical attribute that parents and patients are most concerned about is the effect of surgery on height. It is known that surgery for scoliosis will lead to cessation of growth for the fused segment. This, coupled with loss of height due to progression of the deformity could potentially lead to diminished trunk length after surgery. Babu et al. studied 28 women with AIS who underwent posterior spinal fusion using Harrington instrumentation and sublaminar wires. The authors concluded that the standing height was diminished by 3.2 cm compared to the normal population and the sitting height was reduced by 2.6 cm, even after posterior spinal fusion and correction. 21 Thus, the prediction of spinal height loss or the original body height loss in scoliosis patients has been reported. 1,22 –24 Several equations have been proposed in predicting height gain after scoliosis correction as described in Table 5.
Studies on height increment after scoliosis correction by surgery.

MT: main thoracic; FB: fulcrum bending.
Watanabe et al. (2012) proposed that increase in T1–L5 length (mm) equal to correction of the Cobb angle × 0.77. In this formula, they showed an increase in spinal length correlated with a correction of the Cobb angle, which can be only obtained after the surgery. 6 However, this prospective study used a single post-operative radiological parameter as a predictor to the height increment. This was comparable with a previous study that focused on Cobb angle alone. 1 This caused the actual height gain obtained from this formula to vary widely. Sarlak et al. then proposed a new predictive formula for the height gain in scoliotic deformity correction. 8 From this formula, they found that preoperative and post-operative Cobb angle, preoperative apical vertebral translation and number of instrumented vertebra were among the significant factors associated with height gain.
In another series, Hwang et al. suggested a formula of height increment from their prospective study involving 447 patients. From the analysis, they concluded that thoracic curve magnitude, number of levels fused, change in sagittal curvature and number of osteotomy were among the significant predictors for the height increment. 9 In 2014, Spencer et al. derived a new formula on multivariable analysis from both preoperative and post-operative radiological parameters. 7 Based on this formula, height gain after scoliosis correction could be predicted from Cobb angle correction, number of levels fused and preoperative stature. All the above studies utilized some of the ‘post-operative parameters’ to predict the height increment. The usage of post-operative parameters would preclude the ability to predict the height gain preoperatively. This is important as parents and patients would always enquire regarding this issue during preoperative counselling. So far, there has been no study that uses only preoperative parameters as a prediction of height gain after scoliosis surgery. All the above studies listed in Table 5 utilize radiographic measurements from post-operative radiographs to predict the post-operative gain in spinal length. This is in contrast with the current study that uses only the preoperative radiographic parameters.
In this study, we found that the MT Cobb angle and the FB Cobb angle were significant predictors for height increment. Other preoperative radiological factors were not found to be significant from the multiple variable regression model. The ability of the FB radiograph to predict post-operative correction using pedicle screw systems have been reported in previous published papers. 25 –28 This could possibly account for its ability to contribute towards prediction of height gain post-operatively as well. In this study, we did not analyse the contribution of change in thoracic kyphosis as a predictor because there was no significant difference in preoperative and post-operative kyphosis in our cohort of patients.
This study also focused on height increment prediction in Lenke 1 and 2 curves only. Inclusion of patients with structural lumbar curve would reduce the accuracy of the formula as more variation would exist within the study group. We included Lenke 2 curves in our study but we found that preoperative PT Cobb angle as well as PT SB Cobb angle were not significant predictors for post-operative height gain. This could be explained by the number of vertebral segments within the PT segment as well as the stiffness of the PT segment. The PT segment has less correctability from the SB radiograph and therefore the contribution to height gain would be less. Therefore, the proposed formula can be applied in both Lenke 1 as well as Lenke 2 AIS curves.
The present study has some limitations. First, the equation proposed in this study is based on the clinical height measurement instead of using spinal height measured from radiographs. However, standardizing the method of measurement as described earlier could minimize measurement error. Secondly, this formula could only be used in predicting the height increment immediately after the surgery. Height changes during follow-up could not be accounted for due to growth of the patient as well as possible loss of correction. We also found that using the formula proposed, we could accurately predict height gain within 5 mm difference with the actual height gain in 51.4% of patients and within 10 mm in 70.0% of patients.
Conclusion
In conclusion, the present study showed that MT Cobb angle and FB Cobb angle were significant predictors for post-operative height gain after scoliosis correction with pedicle screw instrumentation. The proposed formula of increase in height (cm) = (0.09 × preoperative MT Cobb angle) − (0.04 × FB Cobb angle) − 0.5 could predict post-operative height gain to within 5 mm accuracy in 51% of patients, within 10 mm in 70% and within 15 mm in 86% of patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.