
Abstract
Study Design
Retrospective cohort study.
Objectives
Patients with trisomy 21 (T21) often have soft tissue differences that lead to greater risk of postoperative wound complications. Our aim was to use a matched cohort of adolescent idiopathic scoliosis (AIS) patients with >2 year outcomes to determine odds of specific wound complications when comparing T21 and AIS patients.
Methods
14 T21 and 544 AIS patients were available for matching. Propensity score matching was conducted using logistic regression models and yielded a 1:5 match of 14 T21 patients and 70 AIS patients. Bivariate analyses were conducted across both patient groups. The proportion of wound complications was estimated along with a 95% confidence interval. Multivariable logistic regression analysis was utilized to determine if there was a significant association between T21 patients and wound outcomes.
Results
64% of T21 patients experienced a wound complication (9/14; 95% CI = 35.63-86.02) while only 3% of the AIS patients experienced a wound complication (2/70; 95% CI = .50-10.86). Patients with T21 had 56.6 times the odds of having a wound complication compared to matched AIS patients (OR = 56.57; 95% CI = 8.12-394.35; P < .001), controlling for age at surgery, BMI percentile, and propensity score. T21 patients had 10.4 times the odds of reoperation compared to AIS patients (OR = 10.36; 95% CI = 1.62-66.02; P = .01).
Conclusion
T21 patients have 10.4× the odds of reoperation and 56.6× the odds of overall wound complication when compared to AIS patients in a 1:5 matched cohort with appropriate controls. This is important for surgical planning, surgeon awareness, and communication with families preoperatively.
Introduction
Trisomy 21 (T21) can lead to a wide spectrum of musculoskeletal pathology largely related to soft tissue differences including hip dysplasia, cervical spine instability and scoliosis, largely attributed to the overexpression of type VI collagen encoded by a gene found on the 21st chromosome.1-6 Prior studies have shown an incidence of scoliosis in T21 patients from 5%–50%.7,8 Despite the increased incidence in this population, the overall rarity of T21 patients with scoliosis means there is limited evidence to determine the natural history of scoliosis as well as guide treatment. Patients with moderate curves have demonstrated benefit from brace treatment whereas surgery has been show to benefit patients with larger curves in order to preserve pulmonary function, prevent deformity progression, and possibly decrease pain.9-12
In addition to predisposing to scoliosis, soft tissue differences also lead to postoperative wound complications. Several case series of T21 patients undergoing scoliosis surgery have identified an increased risk of postoperative complication including infection, wound dehiscence, and pseudarthrosis.13-20 The incidence of wound complications for T21 patients undergoing scoliosis surgery ranges anywhere between .56% to 14% with a mean incidence of 9.4%.14,15,17 Immune system differences may further contribute to the increased infection rate in T21 patients. 21
This single center study aims to add to the knowledge of scoliosis in T21 patients by providing a comparison to a matched AIS cohort with at least 2 years follow-up. Given the paucity of literature on this subject matter, the goal was to provide additional guidance on this complex matter in order to help improve preoperative counseling and possibly guide interventions to reduce the high rates of wound complication in this population. We hypothesized that the T21 cohort of patients would have a higher rate of postoperative wound complications compared to the AIS cohort.
Methods
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Review Board of Boston Children’s Hospital (No. IRB-P00040820). Informed consent was waived due to the retrospective nature of the study and the minimal risk to the subjects.
We retrospectively reviewed the medical records and radiographs of fourteen consecutive female patients with T21 who underwent surgery from 2010 to 2021 with 6 surgeons. These patients were subsequently matched to a total cohort of 544 operative AIS patients based on sex, age, BMI, and major curve magnitude. All 14 T21 patients had a confirmed diagnosis of T21 based on published criteria with additional confirmation from a pediatric geneticist. Inclusion criteria included age <21 years at the time of surgical intervention, confirmed diagnosis of Down Syndrome/Trisomy 21 or AIS, and a history of posterior spinal fusion for correction of scoliosis from 2010 to 2021. Exclusion criteria included patients who had prior spine surgery before undergoing posterior spinal fusion, insufficient follow up time (<2 years), insufficient radiographic data, and age >18. One patient older than 18 at the time of surgery was excluded from the study. Patient distribution was equally spread throughout the group of 6 surgeons without significant differences. All patients received perioperative cephalosporin for infection prophylaxis. Our institution employs the use of a multi-disciplinary Complex Care Service for medically complex patients (including the T21 patients) undergoing major surgery. The Complex Care Service works alongside the orthopedics team to ensure adequate pre-operative optimization in all facets of the patient’s care including aerodigestive health problems, nutrition, Gastrostomy tube management, etc.
Patient Demographics (N = 84).
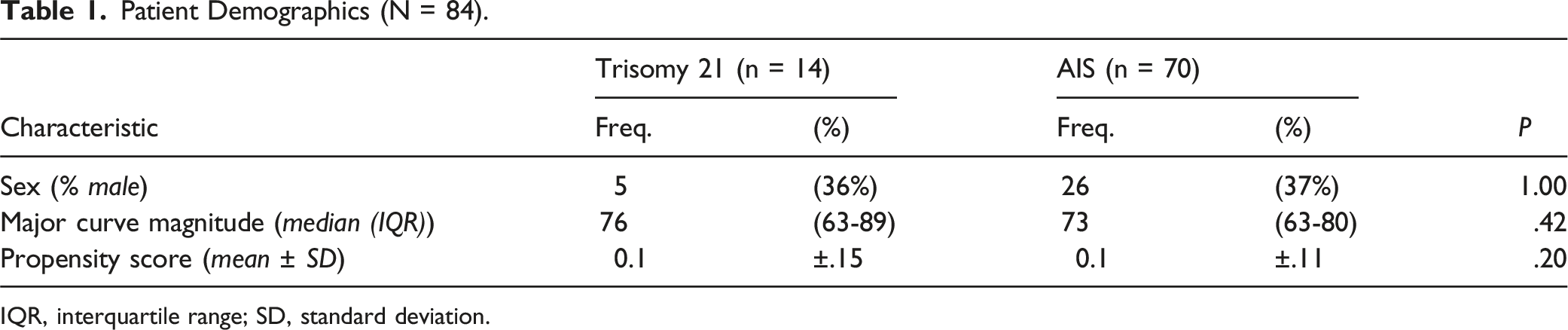
IQR, interquartile range; SD, standard deviation.
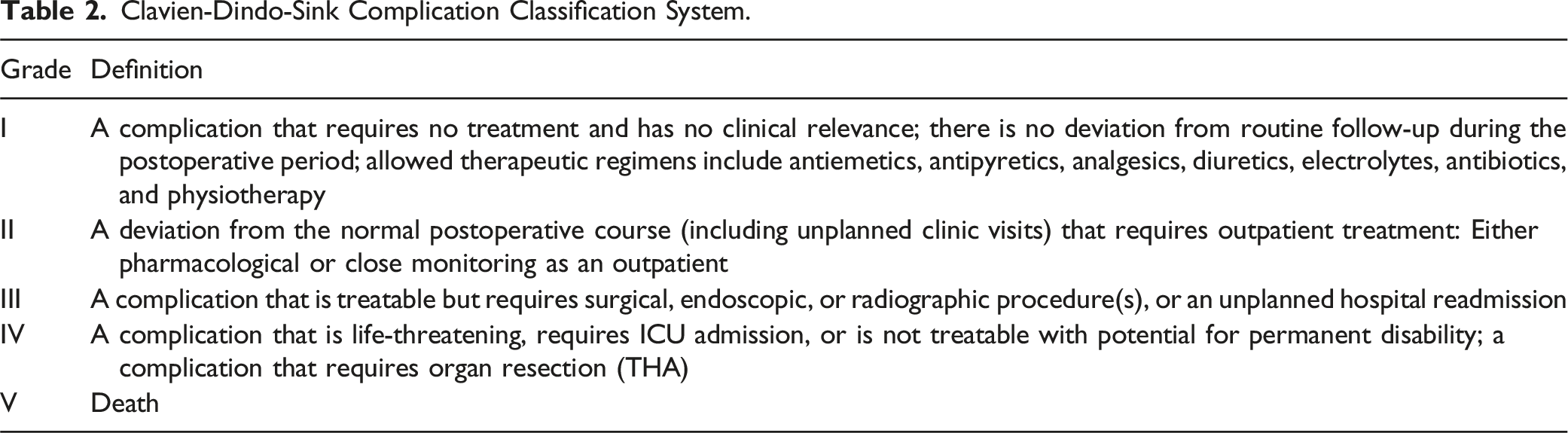
Clavien-Dindo-Sink Complication Classification System.
Results
Patient Characteristics (N = 84).
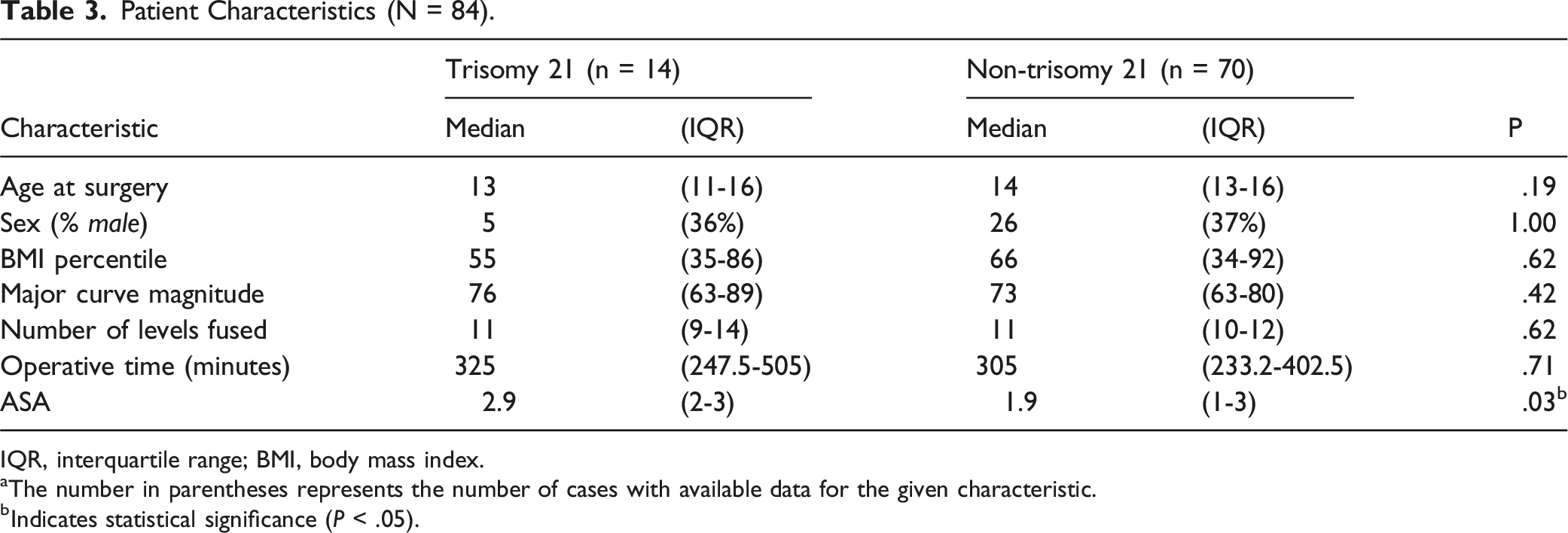
IQR, interquartile range; BMI, body mass index.
aThe number in parentheses represents the number of cases with available data for the given characteristic.
bIndicates statistical significance (P < .05).
Cohort Outcomes (N = 84).

Wound Complications in Trisomy 21 Patients (N = 9).
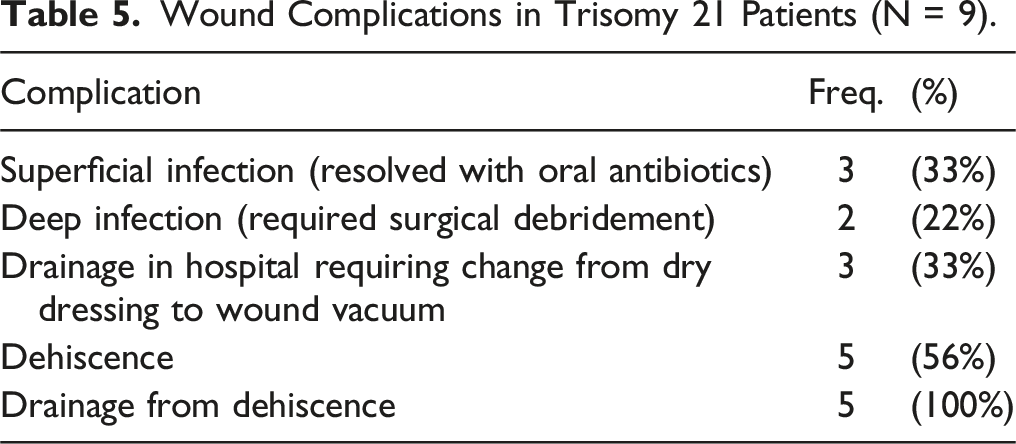
Patients with T21 had a significantly higher proportion of wound complications compared to the sex and major curve magnitude matched non-trisomy 21 patients (P < .001). Patients with T21 had 56.6 times the odds of having a wound complication compared to non T21 patients (OR = 56.57; 95% CI = 8.12-394.35; P < .001), controlling for age at surgery, BMI, and propensity score. T21 patients had 10.4 times the odds of reoperation compared to non-trisomy 21 patients (OR = 10.36; 95% CI = 1.62-66.02; P = .01), controlling for age at surgery, BMI, and propensity score. Of the patients requiring reoperation among T21 patients, 1 developed a culture negative seroma and drainage with wound dehiscence, 1 developed for deep infection, and 2 had hardware failure greater than 1 year after surgery. There were no long-term complications among either population.
Discussion
In this current study, we demonstrated that T21 patients have a dramatically higher rate of wound complications compared to matched AIS patients. T21 leads to a 10-fold increased risk of reoperation at 29% and more than 50-fold increased risk of overall wound complication at 64%. These increased risks are even greater than those previously published and demonstrate a need for improved soft tissue management in the T21 population.14-17,27
Surgical correction of scoliosis in T21 patients is wrought with complications, especially compared to the adolescent idiopathic scoliosis population.15,17,27 Fraser et al 17 detailed the postoperative outcomes of 23 T21 patients in a 2022 retrospective case series. 12 of the 23 patients sustained a postoperative complication. Six of those complications were categorized as CDS Type III or IV (including 2 wound complications requiring I/D). In a separate study, Milbrandt et al reviewed 33 T21 patients with associated scoliosis. 15 Seven patients in their study underwent spinal fusion and 1 patient was reported to having a wound complication/infection requiring revision surgery. In 2003, Lerman et al 27 examined 7 T21 and scoliosis operated over a 16 year period. The authors found a high rate of overall complications (71.4%), with 2 cases of wound infections requiring I/D as well as 2 additional episodes (28.6%) of delayed wound healing without infection.
The higher rate of wound complications found in this study may be due to the larger curve magnitude (mean 76° in our study vs mean 61° in the study by Fraser et al 17 ), differences in comorbidities including neuromuscular and immunologic disease, surgical technique, or possibly statistical variation due to small patient cohorts. It has been well documented that patients with T21 have significant immune dysregulation. Several studies investigating the biochemical etiology of immune dysregulation in T21 patients have pointed towards overexpression the SOD gene along with impaired prostaglandin production as potential culprits for altered structure/function of skin and soft tissue leading to increased susceptibility to bacterial and fungal infections.1,5,6 Preoperative counseling on the increased risks and likelihood of reoperation is also an important part of caring for this high-risk population. Care in soft tissue handling and closure including initial application of an incisional negative pressure dressing as the primary dressing could potentially be helpful in reducing both infection and dehiscence rates and have been shown to decrease wound complications including infection in other high risk orthopedic surgeries.28-31 It is unclear whether the use of a deep drain in this population has any role in increasing or decreasing complication rates.
Given the high postoperative complication rate associated with surgical correction of scoliosis in T21 patients, it is fair to question if the benefits of surgical intervention outweigh the risks, which Milbrandt et al hinted to at the conclusion of their study in 2005. 15 However, several studies have demonstrated the objective improvement in curve correction that surgery can bring out in this patient population. Fraser et al 17 demonstrated a change in major Cobb angle from pre to postop of 61.7° ± 17.6° to 19.4° ± 14.8° with maintenance of correction at 2 years at 22.0° ± 10.3°. Similarly, Abousamra et al 14 demonstrated in a 2017 retrospective cohort study that T21 patients undergoing surgical correction for scoliosis achieved immediate postoperative correction of 68% at the thoracic and 71% at the lumbar level with maintenance of this correction at final follow up (mean follow up of 2.6 years). Milbrandt et al achieved a mean postoperative magnitude of 31° in the thoracic curve and 37° in the lumbar curve, while Lerman et al achieved a mean postop magnitude of 22° in the thoracic and 34° in the lumbar curve.15,27 Additionally, none of the studies documenting the outcomes of scoliosis surgery in T21 patients noted any intraoperative complications, which suggest that scoliosis surgery in this patient population is not necessarily any more technically demanding or challenging compared to a non T21 cohort of patients.14,15,17,27 The deleterious effects of scoliosis progression on cardiopulmonary function have been well documented in the literature including restrictive lung disease, pulmonary hypertension, reduced exercise capacity, and right ventricular dysfunction.32,33 As the life expectancy for individuals with Down’s syndrome continues to improve along with increased participation in athletic endeavors such as sports, the potential gains achieved from surgical correction of moderate to severe curves becomes even more beneficial to avoid functional limitations associated with scoliosis progression.1,34,35 The studies on bracing in T21 patients has been limited to very small case series with mixed results.14,15 It is well known that the effectiveness of bracing depends on patient compliance, which can be difficult in certain T21 patients depending on the severity of cognitive limitation.36,37
This study had several limitations. First and foremost, the retrospective nature of this study portends inherent biases including selection bias. Additionally, due to the low incidence of T21 patients undergoing scoliosis surgery, the sample size for the T21 cohort in this study was small. However, given the paucity of literature on postoperative outcomes after scoliosis surgery in pediatric T21 patients, we felt that the significantly higher postoperative wound complication rate in this population is still valuable information and should be shared with the orthopedic community to help shed additional light to the unique set of challenges that T21 patients bring about. This study further builds adds to previously published literature that has demonstrated increased wound complications in T21 patients when undergoing total hip arthroplasty, cervical spine surgery, adenoidectomy, and tonsillectomy.38-40 While this sample size was small, this study is the second largest study to date focusing on the outcomes of pediatric T21 patients undergoing scoliosis correction surgery. Because we do not routinely obtain preoperative nutritional labs for our patients, we were unable to evaluate how preoperative lab values such as albumin, pre-albumin, total lymphocyte count could potentially correlate to postoperative outcomes. This is certainly an avenue for future studies to investigate because nutritional status has been shown to correlate with postoperative wound complications in orthopedic surgery.41-44 However, one manner in which we did attempt to optimize preoperative nutrition in the T21 patients is through the use of our multidisciplinary Complex Care Service, with previous literature demonstrating that preoperative comanagmeent with complex care pediatricians in children with neuromuscular scoliosis undergoing spinal fusion aiding in reducing postoperative complications. 45
Overall, this retrospective single center study comparing outcomes in T21 patients vs age and curve matched AIS patients found that T21 patients are at a significantly higher risk for postoperative wound complications. The matched cohort of patients with AIS in this study provided additional context for understanding the increased wound complications associated with T21. The increased rate of wound complications in this cohort compared to prior studies in the literature should serve as precaution to surgeons treating these types of patients and emphasizes the importance on improved soft tissue care and increased postoperative surveillance in preventing such complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.