
Abstract
Study Design
Retrospective study.
Objective
To evaluate the surgical outcomes of younger adult idiopathic scoliosis patients (YAdIS) with selective thoracic fusion by comparing them with adolescent idiopathic scoliosis (AIS).
Methods
Seventy-two idiopathic scoliosis patients (36 adults and 36 adolescents) treated by posterior-only all-pedicle screw technique were retrospective reviewed and matched by fusion levels. Radiographic parameters were evaluated preoperatively, postoperatively, and at final follow-up. Operating time, blood loss, transfusion, and complications were noted. The clinical outcome was assessed by the Scoliosis Research Society-22 questionnaire (SRS-22).
Results
The major thoracic curves in YAdIS and AIS groups were 56.3° ± 9.7°, 53.3° ± 10.1° and corrected to 17.2° ± 7.3°, 14.9° ± 7.5° respectively without significant difference in correction rate (69.3% vs 72.0%). For the lumbar curve, Cobb angles in 2 groups were 35.6° ± 10.1°and 31.4 ± 9.2° preoperatively, and were spontaneously corrected to 18.5° ± 9.0° and 12.6° ± 8.2°.Correction rates were 48.0% and 59.8% (P < .05). Preoperative and postoperative coronal vertebra alignments (CVA) in the YAdIS group were 20.6 ± 9.7 mm and 16.8 ± 7.9 mm (P > .05), while in the AIS group was 17.8 ± 10.5 mm and 9.7 ± 8.3 mm (P < .05). However, sagittal parameters showed significant improvements in thoracic kyphosis in both groups (P < .05). Complication rates were 25% vs 11.1% (P = .13) with no significant difference. Preoperative SRS-22 was worse in the YAdIS group than AIS group. All the scores were significantly improved postoperatively in the YAdIS group. However, in the AIS group, only SRS scores improved significantly.
Conclusions
YAdIS can also be treated very well with selective thoracic fusion based on the Lenke rule used for AIS.
Keywords
Introduction
Adult idiopathic scoliosis (AdIS) is a special subcategory of spine deformity that does not develop in patients over 18 years old, which may be due to the worsening of untreated childhood idiopathic scoliosis. The prevalence rate among adults under 45 years old is about 2%-4%. 1 In general, cases of adult idiopathic scoliosis begin in adolescence. The treatment of AdIS involves both surgical and non-surgical options. Brace therapy, 1 of the non-surgical options, is considered to be the only effective way of conservative treatment. 2 However, it is an unpleasant experience that may affect the image, and interpersonal interactions, and ultimately reduce the overall quality of life of patients. For those adult patients, surgery is often required when curve progression, physical pain, and disability occur. However, several reports have shown that there are age-associated differences in radiographic parameters and disability in AdIS patients. It is suggested that pain and disability were the main factors that influenced the treatment modality for older patients with adult scoliosis. However, for younger patients, operative treatment was driven by increased frontal plane deformity.3-5 Most of the AdIS population included in previous studies was treated as a whole without making a distinction between younger adult and older adult patients, which may result in potentially confounding.6-8
As we know, selective thoracic fusion (STF) has been proven to be effective in adolescent idiopathic scoliosis (AIS) when the following criteria are met. Lenke et al suggested that 2 or 3 ratios of thoracic to lumbar curves (Cobb angle ratio > 1.2, AVT ratio > 1.2, AVR ratio > 1.0) should be fulfilled to obtain successful outcomes after STF. In addition, curves not meeting the ratio criteria or those with lumbar curves > 60°, Nash-Moe’s rotation grade > 2.5, or AVT > 4.0 cm should not be treated as STF.9,10 However, for the younger adult idiopathic scoliosis patients (YAdIS), how to choose the best surgical strategy is still unclear. Unlike AIS patients, YAdIS patients have a stiffer curve after skeletal maturation, which may require longer fusion segments and wider release. Thus, the complication rate may be higher and the recovery would be slower because age was proved to be associated with an increased risk of hemorrhage, infection, and reoperation. 11
With younger adult idiopathic scoliosis, they complain less about symptoms related to lumbar spinal stenosis but care more about their appearance, which is very different from older patients who focus more on functional ability. Only 1 paper discussed the relationship between the sagittal plane change and clinical improvement in AdIS older than 40 years of age. However, the surgical outcome of YAdIS may be different from older ones or overall adult patients. Thus, we must discuss the radiographic and clinical characters of younger adult idiopathic scoliosis (YAdIS) under the age of 40 separately.
Up to now, there is little information about the surgical outcome of younger adult idiopathic scoliosis patients (under aged 40) (YAdIS). This study tried to demonstrate the surgical outcome of YAdIS under the age of 40 by comparing it with AIS.We propose a retrospective matched cohort study to compare YAdIS with AIS treated with STF strategy to demonstrate whether this Lenke rule is applicable for the YAdIS patients.
Materials and Methods
After approval by the institution review board (IRB) of the hospital, participants or, where participants are children, a parent or guardian, who signed the Informed Consent Form were taken into this retrospective study. The inclusion criteria were as follows: (i) scoliosis patients met the criteria of STF (T/L cobb angle ratio> 1.2) stated by Lenke; (ii)underwent posterior-only all-pedicle screw technique. (iii) absence of spinal disease. (iv) follow-up for 12 months or more. Patients who had a history of spine surgery were excluded. From Jan 2008 to Jul 2012, a consecutive population of 36 adolescents and 36 younger adults with single or double thoracic scoliosis were reviewed retrospectively and matched by the magnitude and pattern of the curve. Major curves ranged from 45 to 75°.
In the YAdIS Group, the average age was 29.1 ± 2.5 years. Five cases were male and 31 cases were female, with an average follow-up of 32.7 ± 5.3 months (24–36 months). According to the SRS classification system, 12 25 cases were single thoracic scoliosis and 11 cases were double thoracic scoliosis. The indication of surgery for these patients was curve progression and cosmetic problems. Meanwhile, some of them suffered from back pain. Most of these patients chose to delay surgery because they were worried about the effect on children’s spinal growth, patients’ studies, daily activities, and psychological states. 13 Unfortunately, these untreated spinal deformities still progressed as patients aged. Patients included in Group AIS were from 10 to 18 years old with an average age of 13.8 ± 2.8 years. Based on the Lenke classification system, 14 28 patients were typed Lenke 1(21 of 1A,5 of 1B,2 of 1C) and 8 patients were typed Lenke 2(5 of 2A, 2 of 2B, 1 of 2C).
Surgical Procedure
For the AIS Group, all patients were placed in a prone position after general anesthesia. After a posterior midline incision was made, the subperiosteal paraspinal muscle was dissected to expose the posterior bone structure. Pedicle screws were inserted into the fusion segments bilaterally with the freehand technique. Fusion strategy was performed by the principle of Lenke classification. All the structural major and minor curves were fused while non-structural compensatory curves were not included. For 10 patients with fixed deformity, multiple Ponte osteotomies 15 were used to attain correction via a posterior approach. Curve correction was achieved using the direct vertebral derotation maneuver, followed by slight convex compression and concave distraction. Decortication of the posterior elements was performed after the correction, and poster-lateral fusion was done with allograft, and autograft, followed by wound closure gradually and drainage retained.
For the YAdIS group, the same procedure was done. As patients in our research didn’t have radicular symptoms of the lower extremity, nerve root and spinal canal decompression were not performed. Multi-segmental Ponte osteotomies 15 were done in 20 patients because of the stiffer curves in younger adults.
Somatosensory-evoked potentials and motor evoked potential were routinely assessed for intraoperative monitoring of spinal cord function. Self-transfusion was used. All patients in the study were operated on by the same group of surgeons. The average operation time, fusion levels, intraoperative blood loss, blood transfusion, hospital days were recorded.
Radiographic and Clinical Evaluation
All patients had pre-and post-operative standing AP and lateral radiographs. Parameters of clinic evaluation were noted, including coronal curves, T5–T12, L1-sacrum sagittal Cobb, proximal junctional angle, coronal vertical alignment (CVA), sagittal vertical alignment (SVA), and Scoliosis Research Society-22. The first 3 were routine measurements for scoliosis patients. We pointed out the other parameters. In addition, preoperative fulcrum lateral bending X-ray films were used to evaluate the flexibility of the curve.16,17
Statistical Analysis
All data were analyzed by SPSS version 22.0 statistical analysis software (SPSS Inc., Chicago, USA). Continuous variables were presented as mean standard deviation and ordinal variables as median (interquartile range). Paired t-test was used to compare all the variables between the 2 groups. Fisher’s exact test was used to test for significance of categorical variables. All statistical assessments were 2-sided and evaluated at the .05 level of significance.
Results
Characteristics and Surgical Variables
Preoperative characteristics and surgical variables for the YAdIS and AIS group.
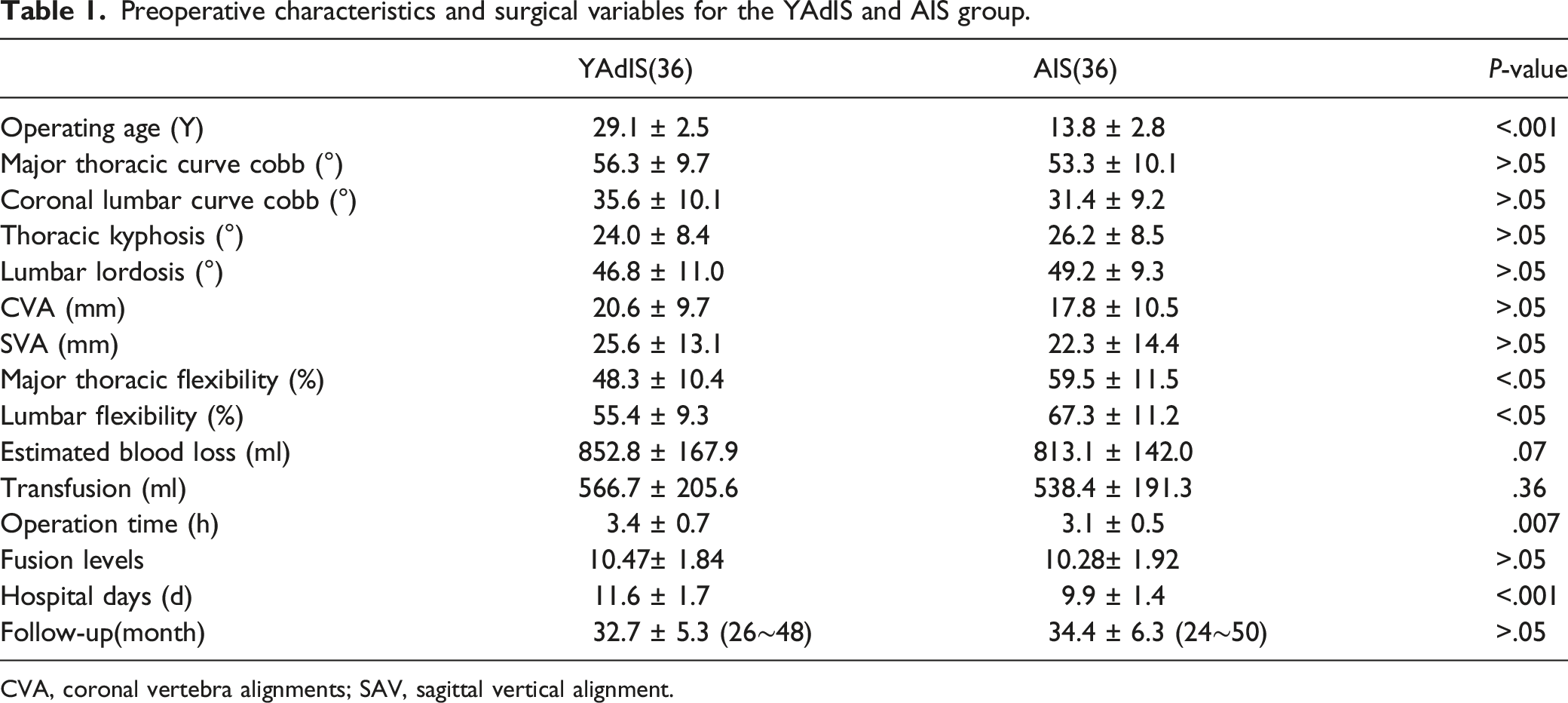
CVA, coronal vertebra alignments; SAV, sagittal vertical alignment.
Preoperative, postoperative, and final follow-up radiographic measurements in 2 groups
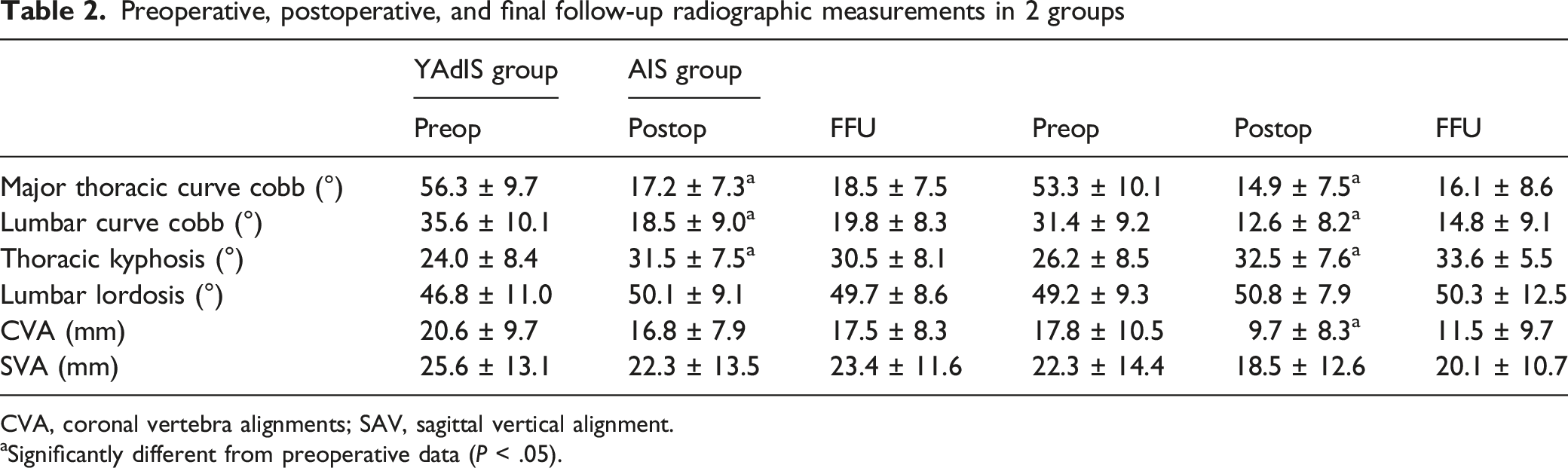
CVA, coronal vertebra alignments; SAV, sagittal vertical alignment.
aSignificantly different from preoperative data (P < .05).
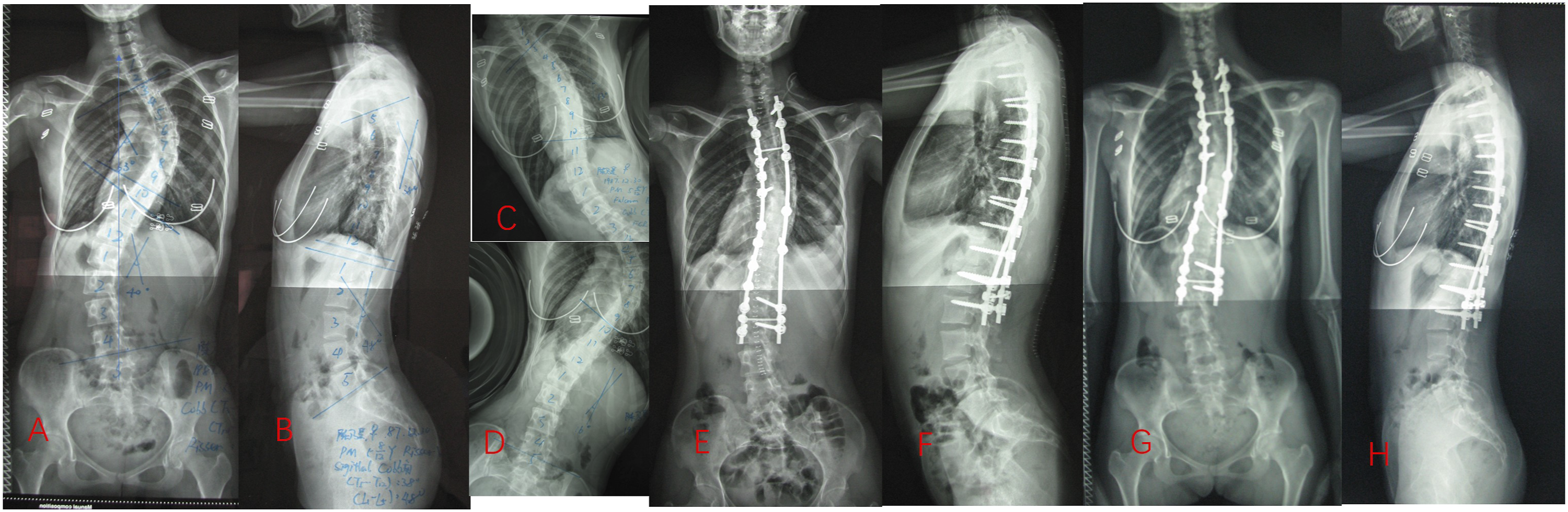
A 23+8-year-old female (Major thoracic curve, SRS system) was treated with posterior spinal fusion with pedicle screw instrumentation from T2 to L2. (A, B): preoperatively, the major thoracic curve Cobb angle was 63°. Lumbar curve was 40°. Thoracic kyphosis (T5 to T12) was 32°. SVA was 0 mm and CVA was 10mm. (C,D): Fulcrum bending, thoracic curve Cobb angle decreased to 40° with flexibility of 36.5%.Lumbar curve cobb decreased to 16 degress with flexibility of 60%. (E, F): Postoperatively, the major thoracic Cobb angle was 22° with correction rate of 65.1%. Lumbar curve was 14°. The thoracic kyphosis was 35°. SVA was -10mm mm and CVA was 0 mm. G,H,32 months after surgery,correction maintained well.
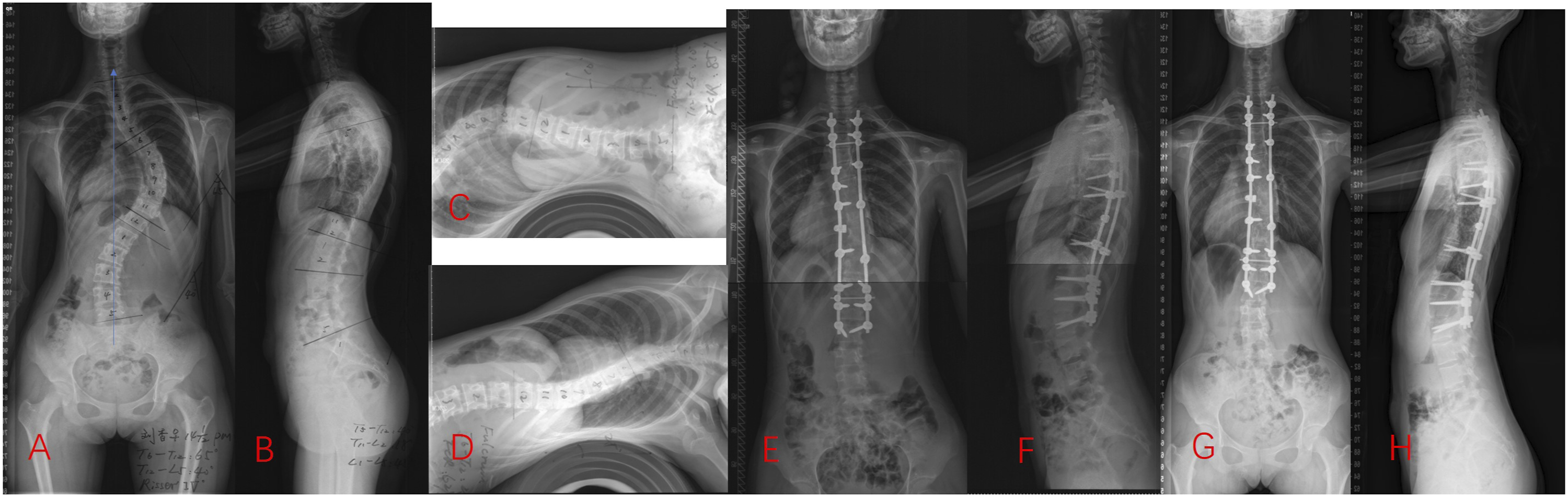
A 14+1-year-old boy (Lenke type 1AN) was treated with posterior spinal fusion with pedicle screw instrumentation from T2 to L2.(A, B): Preoperatively, the major thoracic curve Cobb angle was 65°. Lumbar curve was 40°. Thoracic kyphosis (T5 to T12) was 40°. Both SVA and CVA were 0 mm. (C, D): Fulcrum bending, thoracic curve Cobb angle decreased to 25° with flexibility of 61.5%. Lumbar curve decreased to 10° with flexibility of 84.6%. (E, F): Postoperatively, the major thoracic Cobb angle was 18° with correction rate of 76.9%. Lumbar curve was 10°. The thoracic kyphosis was 38°. Both SVA and CVA were 0 mm. (G, H):At 26-month-follow-up,correction maintained well.
Clinical Outcomes
Comparison of the SRS-22 scores before and after surgery.
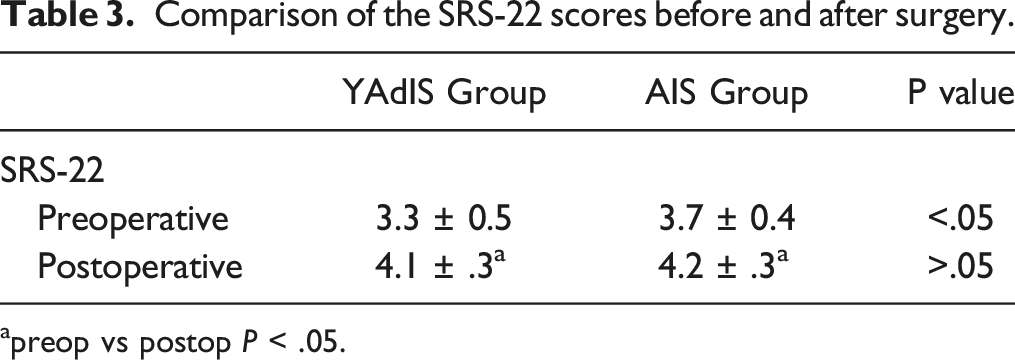
apreop vs postop P < .05.
Complication
In both groups, zero patients had a neurologic deficit, construct failure, or pseudarthrosis. One patient in the YAdIS group experienced a deep wound infection that needed debridement. Nevertheless, 4 patients experienced postoperative coronal imbalance at the most recent follow-up in the YAdIS Group, while 2 patients showed postoperative coronal decompensation in the AIS group. No cases of sagittal decompensation were observed in either group. The complication rate in the YAdIS group was higher than the AIS group (13.9% vs 5.6%), but no significant difference was found (P = .49).
Discussion
This retrospective matched cohort study included 72 cases of younger adult and adolescent idiopathic thoracic scoliosis operated with STF according to Lenke rules mentioned in AIS.9-11,18 Correction rates of the major thoracic curve in 2 groups were 69.3% and 72.0% respectively without significant difference, though statistical differences were shown in fulcrum flexibility of the major thoracic curve (48.5% vs 59.5%). The results are accordant with other studies. Peelle reported the thoracic correction rate of 62% using selective thoracic fusion for adult idiopathic scoliosis. 8 Our previous study demonstrated the correction rate was from 52% to 55% depending on the different age groups of AdIS. 7 The slightly lower correction rate in that study may be due to more severe curves with a mean Cobb of 72°. The other reason may be that more patients in the YAdIS group (20/36) had been done posterior Ponte osteotomies to increase flexibility. 19 Even for the severe and rigid adult idiopathic scoliosis, Ponte osteotomies were effective to gain satisfactory correction despite major complications. 20 This was also associated with a little longer operation time and blood loss in the YAdIS group.
Coronal correction rates of the unfused lumbar curve after selective thoracic fusion were 48.0% and 59.8% in the YAdIS group and AIS group, respectively. As was reported in the study of selective thoracic fusion by Peelle 8 , there was 50% spontaneous correction of lumbar curves, which was comparable to 48% in our YAdIS group. However, the spontaneous correction rate of the lumbar curve in the YAdIS group was significantly less than in the AIS group (59.8%), which may be due to the different flexibility of the lumbar curve in the 2 groups (55.4% vs 67.3%). The importance of the lumbar curve flexibility is advocated in the selective thoracic fusion for the AIS population. 21 The ratio of the flexibility of thoracic vs lumbar curves has also been deemed predictive of successful thoracic fusions. 22 For adult patients, there is not a ‘‘cut-off’’ value for lumbar curve flexibility, as adults with presumably stiffer curves may possess less intrinsic elasticity for correction. However, some lumbar curves in adults may mimic the response of adolescent curves, whereas others may exhibit considerably more rigidity.
Furthermore, different lumbar curve spontaneous correction rates may lead to the different incidence of coronal decompensation in the YAdIS group and AIS group (11.1% vs 5.5%). The incidence of coronal decompensation has been reported to range from 10% to 40% by hooks or hybrid constructs, while 5-16% by pedicle screw constructs.23-25 It’s postulated that excessive thoracic curve correction and the relative inability of the lumbar curve to accommodate the correction of the thoracic were factors in postoperative trunk decompensation. 25 Although this conclusion was made by Suk in AIS patients, this theory may also be suitable for the selective thoracic fusion for the treatment of YAdIS patients too. Carefully evaluating the flexibility of the thoracic/lumbar curve and predicting the ability of the minor curve spontaneous correction preoperatively is very important to minimize decompensation.
Sagittal plane alignment was also evaluated in these 2 groups. We did not find thoracic kyphosis reduced postoperatively. Suk et al. 26 also reported good correction of preoperative hyperkyphosis (from 9° to 27°) in their study. This result was contrary to several other independent studies which noted an average loss of between 10° and 12°in thoracic kyphosis in pedicle screws treatment of AIS.23,27,28 Better sagittal thoracic hyperkyphosis correction in the present study may be due to sparse pedicle screws instead of all pedicle screws. Furthermore, Ponte osteotomy helps to release the posterior elements and may contribute to the restoration of sagittal alignment. 18 The clinical improvement potential for sagittal lordotic change provided by Ponte osteotomies has been reported to be in the range of 9.3–10.78 per level.19,29 Restoring of normal thoracic kyphosis is of great importance for maintaining lumbar lordosis and preventing sagittal imbalance with aging, especially for adult scoliosis. 30 Sagittal parameters have been proved to be strongly correlated with health-related quality of life and positive sagittal balance has been considered the most reliable predictor of clinical symptoms in operated adult scoliosis patients. 2
In this study, statistically significant improvement in SRS scores from preoperative to postoperative was seen in both groups. Although the SRS score before surgery was worse in the YAdIS group than the AIS group, the health-related quality of life outcome was almost the same at the final follow-up.
Limitation
The limitations of the study are its retrospective nature, short-term follow-up, and the small number of patients in this series.
Conclusions
Younger adult idiopathic scoliosis patients patients gained similar correction of the major thoracic curves as AIS patients by selective thoracic fusion although the curve was stiffer. However, a more extensive release technique was needed which was associated with a longer operation time. SRS scores for YAdIS were lower preoperatively but not different in postoperative improvement. This result suggested that YAdIS can also be treated very well with selective thoracic fusion based on the Lenke rule used for AIS.
Footnotes
Author Contributions
All authors contributed to the surgery that the data was collected from. The first draft of the manuscript was written by HL Y. All authors commented on previous versions of the manuscript. Data collection and analysis were performed by HC. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Natural Science Foundation of China (81972080), the Science and Technology Planning Project of Guangdong Province (2017B030314139), the Natural Science Foundation of Guangdong Province (2015A030312004). The authors declare that they have no other financial support.
Ethics Approval
This research program was approved by the institutional review committee of the People's Liberation Army (PLA) General Hospital of Southern Theatre Command.
Consent to Participate
Informed consent was obtained for publication of patient data.
Consent for Publication
All authors read and approved the final manuscript for publication.
Availability of Data and Material
Informed consent was obtained for publication of patient data. We have full control of all primary data and agree to allow the journal to review their data if requested.