
Abstract
Study design
Meta-analysis.
Objective
To compare the clinical and radiological outcomes in patients with Adolescent Idiopathic scoliosis (AIS) treated by selective thoracic fusion (STF) with lowest instrumented vertebra (LIV) at touched vertebra (TV) vs stable vertebra (SV).
Methods
The databases PubMed, Embase and Google Scholar were searched until November 2020.Studies which had Lenke type 1 curves and Lenke type 2 curves in adolescent population treated by STF and which reported pre- and post-operative curve characteristics including correction percentage and complications were included. Studies which did not report the LIV selection, curve correction percentages and whose full text could not be acquired were excluded.
Results
Eight studies were included for analysis of which seven were found to be retrospective studies (level III evidence) and one was prospective study (level II evidence) each. Overall proportional meta-analysis found no significant difference in correction rate, total srs-22 scores, and complication rates.
Conclusion
The evaluation of SV group and TV group as LIV for selective thoracic fusions in AIS reveals a comparable outcome in terms of curve correction, patient satisfaction scores and complication rates. The TV can be chosen safely as the LIV especially in type A and B Lenke 1&2 curves, as it saves more motion segments when compared to SV.
Keywords
Introduction
Adolescent idiopathic scoliosis (AIS) curves are commonly classified according to the Lenke classification system. 1 Selective thoracic fusion (STF) is one of the surgical modalities to treat the Lenke type 1 and 2 curves. STF includes the fusion of the main thoracic curve ,and saves the motion segments of the lumbar spine.2‐4 Choosing a lower instrumented vertebra (LIV) too proximal may lead to decompensation and progression of unfused curves, whereas choosing a LIV too distal leads to reduced motion segments .Striking a perfect balance between saving the motion segments and preventing the curve decompensation is vital for superior post-operative outcomes.5,6 Majority of the surgeons believe fusion till stable vertebra (SV) is a safe option and is associated with good post-operative outcomes, but few recent studies have propagated that curves can be adequately treated by LIV proximal to SV. 7 Studies done by Lenke et al. showed that selecting the last touched vertebra (TV) as LIV in type 1 and type 2 curves led to good post-operative outcomes. Few other studies done by Cao et al. 8 and Matsumoto et al. 9 put forward the theory that TV can be a safe option to choose LIV in treating Lenke type 1 and type 2 curves. However, there is a lack of consensus in the literature with regards to selection of LIV while performing a STF.
The aim of this meta-analysis is to collect the existing scientific evidence from the literature and to compare the outcomes such as curve correction and clinical outcomes between the two groups which were divided based on LIV selection (TV vs SV). We have tried to incorporate all the available literature from the past two decades and have followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines to help improve the reporting quality of our study.
Methods
Literature Search
The search included extensive electronic and manual literature using PubMed, EMBASE and Google Scholar by two independent reviewers. The literature on target were the articles which reported the outcomes of selective thoracic fusion in AIS for Lenke curves 1 and 2 published from 2000 to 2020.Articles published in a language other than English were not included. Medical subject heading (MeSH) words used for search were ‘scoliosis’ and ‘Scoliosis/surgery’ and non-MeSH words used were ‘selective thoracic fusion’, ‘adding on phenomenon’, ‘Lenke type 1 curve’, ‘Lenke type 2 curve’, ‘touched vertebra’ and ‘lowest instrumented vertebra’. The manual search was done by cross-checking the references of the included citations. Unpublished data was excluded. Duplicates were eliminated by using Zotero’s de-duplication function followed by manual elimination after merging all the references.
Study Selection
The studies having the following criteria were included in the analysis (1) Lenke type 1 curves and Lenke type 2 curves in adolescent population, (2) selective thoracic fusion of the curves, (3) studies with curves less than 70 degrees, (4) retrospective and prospective case studies, (5) studies mentioning LIV, pre- and post-operative curve characteristics including correction percentages and complications.
Studies which did not report the LIV selection, curve correction percentages, follow-up less than 24 months, studies with osteotomy more than Schwab grade 3 10 and whose full text could not be acquired were excluded. Case reports were also excluded.
Quality Assessment
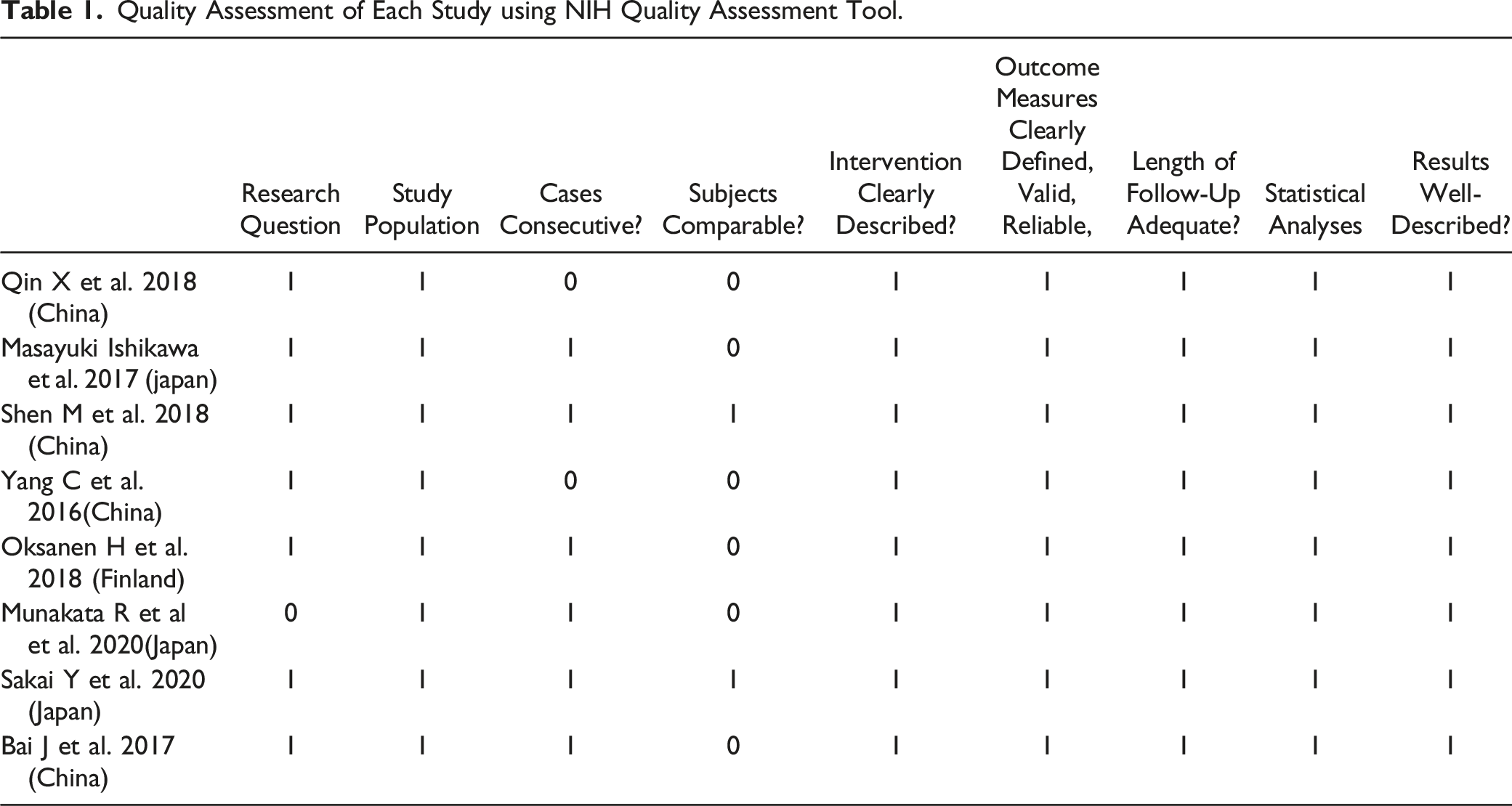
Quality Assessment of Each Study using NIH Quality Assessment Tool.
Data Extraction
The data was extracted from the retrieved articles by two authors (SI, KA). The data extracted included the study characteristics, outcome variables and demographic data. The study characteristics included the name of the author, title, study design, information on LIV, journal and year of publication, level of evidence and quality of study. The extracted demographic data included the number of patients, mean age and number of males and females. Curve characteristics such as pre- and post-operative Cobbs angle, correction percentages, SRS-22 score with its components and complications constituted the measured outcome variables. Once the data was extracted, the studies were classified into two groups for analysis – (1) with LIV at stable vertebra (SV) and (2) with LIV at touched vertebra (TV). In the case of data being incomplete or unclear, the corresponding author of the study was contacted for complete data sheet.
Statistical Analysis
Descriptive analysis using means, standard deviation (SD) and ranges (minimum, maximum) of the pooled data across the included studies were performed. Meta-analysis was performed using the Metafor package in R statistical software v4.0.0 (R Core Team, Vienna, 2020). Analysis was performed using a random effects model using the DerSemonian Laird method. Forest plots were generated to draw comparisons between the two groups (SV and TV). Weighted mean difference (WMD) and relative risk (RR) were used for analysing continuous and categorical or binary data, respectively. A P-value of less than .05 was considered significant, whereas any overlap within the 95% CI or P-value more than .05 was considered insignificant.
Results
The PRISMA flowchart of study selection is shown in Figure 1. A total of 468 articles were acquired after excluding duplicated articles from various databases. After initial screening, 34 articles were yielded for full-text analysis based on the pre-decided inclusion and exclusion criteria. Further, 26 articles were excluded because of incomplete data, lack of clarity on LIV selection, and studies dealing with sagittal LIV. Subsequently, 8 studies were evaluated for final analysis. PRISMA flowchart showing the selection of studies for the meta-analysis.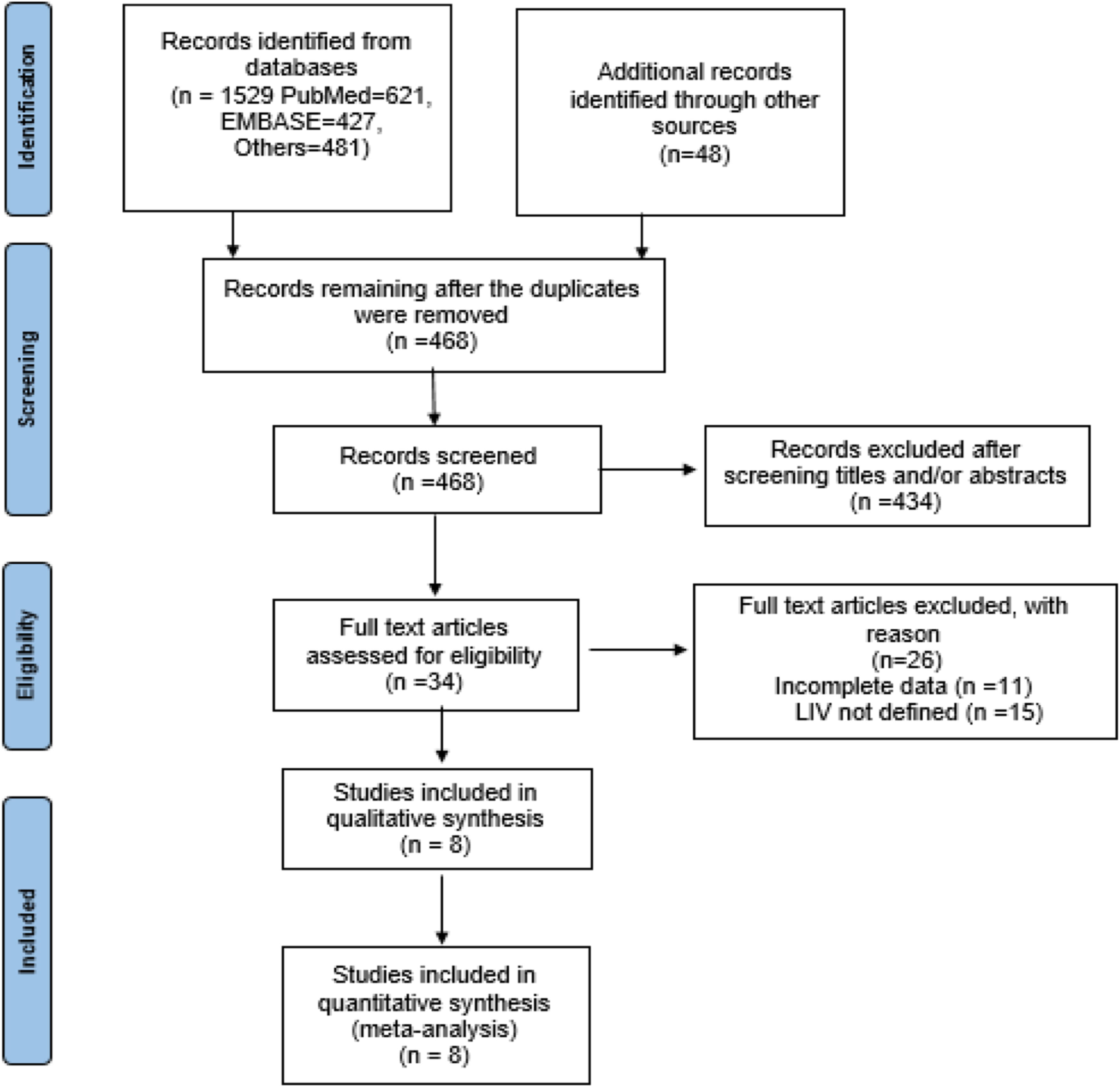
Study Characteristics
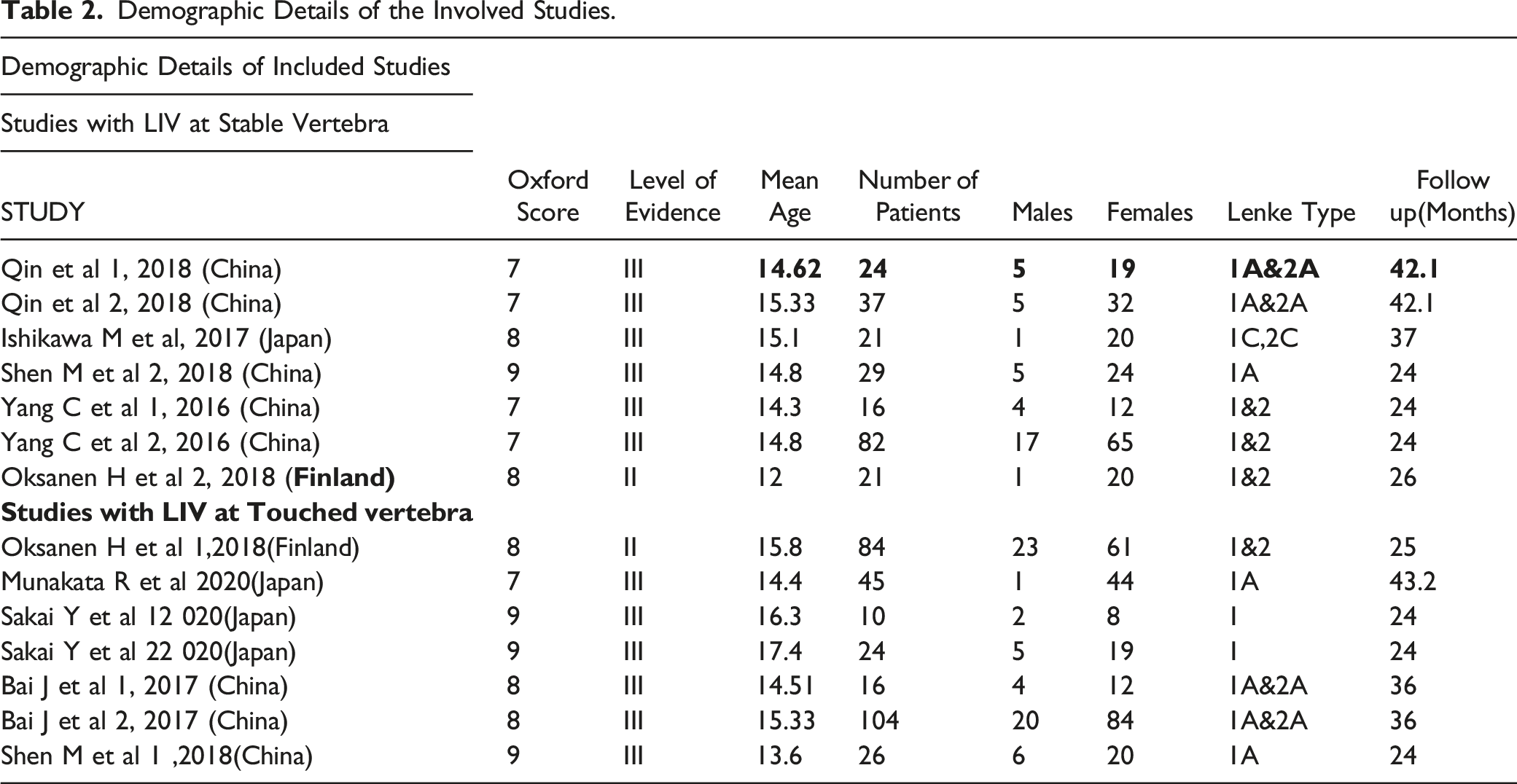
Of the 8 included studies, 7 were found to be retrospective studies (level III evidence),12‐18 whereas 1 was prospective study (level II evidence) 19 . No RCTs were found in the literature. Of the 8 studies, 2 studies were found to focus their results on comparison of outcomes between the touched vertebra group (TV) and stable vertebra group (SV). Among the remaining 6 studies, three evaluated the outcomes of deformity correction with TV group and SV group each. All the studies were found to have a quality score of 6 or above out of 9 and were subsequently included in analysis (Table 1).
Demographic Data
Demographic Details of the Involved Studies.
Correction Rate
All the studies were included in the primary analysis of correction rate for the main thoracic curve between the two groups (SV and TV). No significant difference was found in the correction percentage between the two groups (MD–70.1; 95% CI–65.15,75.21 vs MD–71.2; 95% CI–66.44, 76.14) (Figure 2). Significant heterogeneity was detected for the outcome (P < .001). Proportional meta-analysis comparing the curve correction rates between the two groups.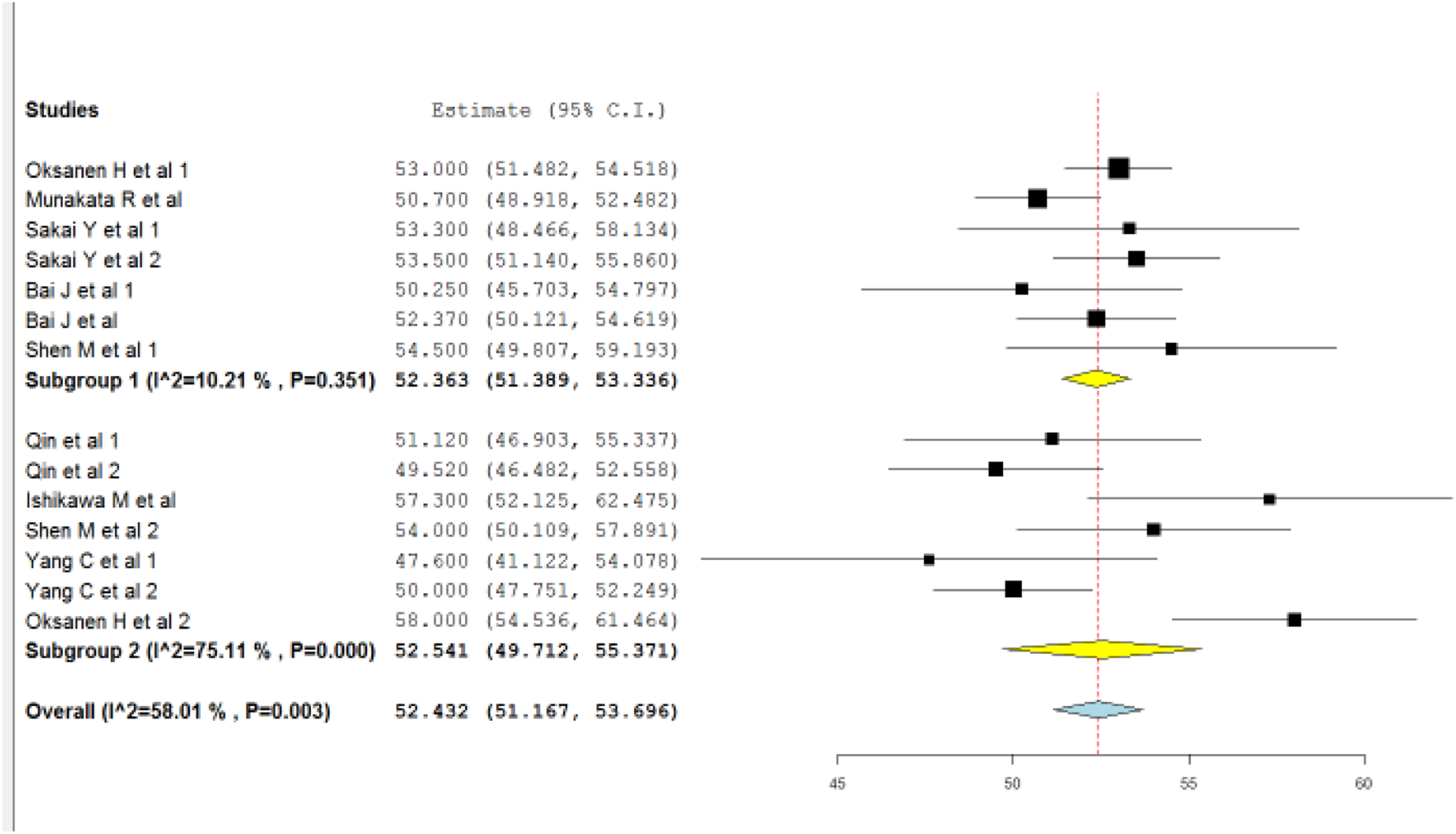
Post-Operative Functional Outcomes (SRS-22 Scores)
Functional outcomes in terms of SRS scores were reported in 5 out of 8 studies. A primary analysis was done between the two groups for all the domains of srs-22 scores viz function, pain, image, mental health and satisfaction. Both the groups were also compared for the total srs scores. No significant difference was found between the two groups for function (MD–3.9; 95% CI–3.59, 4.36, I2 = 87.7% vs MD–4.3; 95% CI–4.08, 4.67, I2 = 96.7%), pain (MD–4.1; 95% CI–4.04, 4.81, I2 = 0% vs MD–4.3; 95% CI–4.32, 4.43, I2 = 36.4%), self-image (MD–3.0; 95% CI–2.16, 3.93, I2 = 98.8% vs MD–4.0; 95% CI–3.76, 4.25, I2 = 94.7%), mental health (MD–3.9; 95% CI–3.71, 4.10, I2 = 71.3% vs MD–4.1; 95% CI–4.07, 4.29, I2 = 36.1%), and satisfaction (MD–3.8; 95% CI–3.54, 4.12, I2 = 78.4% vs MD–4.1; 95% CI–4.03, 4.26, I2 = 47.6%). There was no significant difference when the total srs scores were compared between the two groups (MD–3.7; 95% CI–3.46, 4.05, I2 = 89.4% vs MD–4.1; 95% CI–4.09, 4.26, I2 = 93.4%).
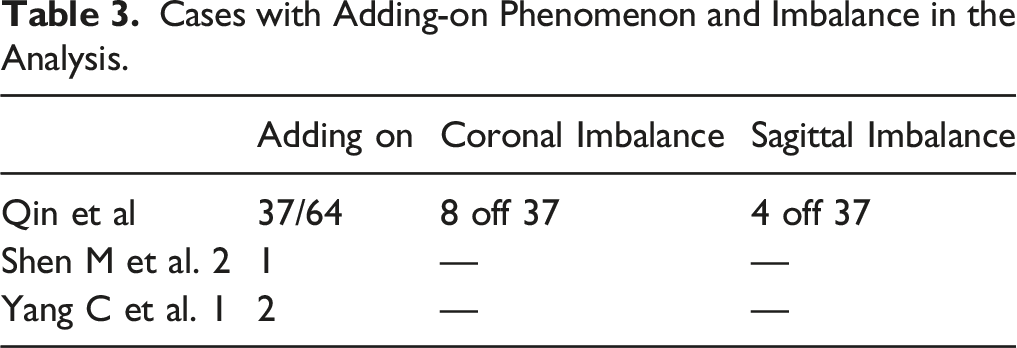
Complications
Cases with Adding-on Phenomenon and Imbalance in the Analysis.
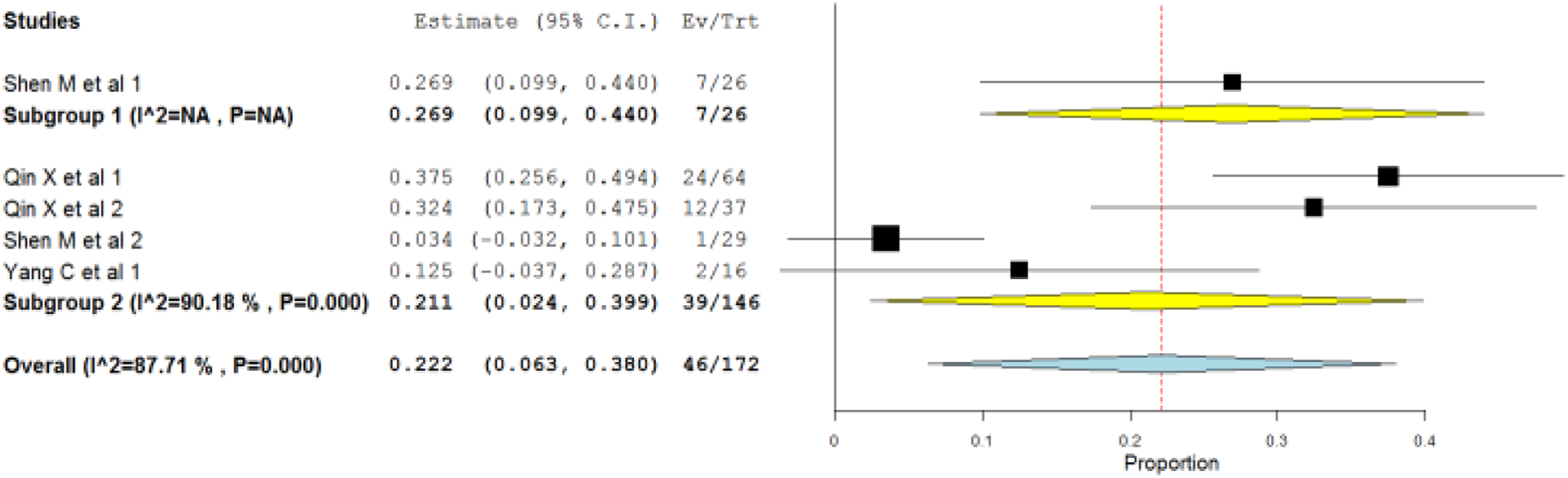
Proportional meta-analysis comparing the complications between the two groups.
Discussion
The standard treatment of progressive AIS curves is by surgical fusion of the curve. The most important factor influencing the post-operative outcomes in AIS curve corrections are the fusion levels.20,21 Incorrect selection of fusion levels , especially incorrect selection of LIV may cause either under correction of the curve or may involve more motion segments thereby reducing mobility and overall functional outcomes.20,22 The treatment has evolved over few decades and the current focus is on preserving as many motion segments as possible while obtaining optimum correction of the deformity. This led to the concept of selective fusion of curves, especially in Lenke type 1& 2 curves. The concept of selective thoracic fusion was first popularised by King et al. where the study group fused the major curve and hoped for the spontaneous correction of other curves. 22 The study group noticed that the lumbar curves did correct spontaneously when only the thoracic curves were fused. 22 As the selective thoracic fusion started gaining popularity, there was a debate among the surgeons with respect to choosing the LIV. King et al. advocated that choosing the LIV at the stable or neutral vertebra led to spontaneous correction of lumbar curve and modest correction of the thoracic deformity. 22 Subsequently, studies were done by Cao et al. and Matsumoto et al. in which TV was used as the LIV and the study groups reported good clinical results.8,9 The authors in the current article compared the curve correction percentage between the two groups based on LIV (TV and SV) and found no significant difference in the curve correction rates between the two groups. It must be noted that all the studies involved in the analysis had Lenke curve modifier ‘A’, with exception of only one study by Ishikawa et al. 18 Further, due to differences between sample size and length of follow-up period, some interpretations may be limited. The curve correction does not serve the purpose if the correction does not translate into better functional outcomes. Five of the eight studies reported the improvement of functional status in terms of srs scores. When sub group analysis was done, there was no significant difference between the two groups for all the domains of srs-22 scores. The total srs scores were compared between the two groups and there was no significant difference between the two groups. The data for pain modality was homogenous, whereas the data for other modalities was heterogenous. Boniello J et al. did a study to compare the functional outcomes of selective vs non-selective fusion in Lenke 1 curves and compared the SRS scores between the two groups. The study group came out with conclusions that selective thoracic fusions have good functional outcomes which are similar to non-selective fusions and selective fusions can be done in curves even with lumbar ‘C’ modifier. 23 Though most of the studies included in our analysis had either lumbar ‘A’ or ‘B’ modifier, the good functional outcomes which were statistically similar in both the groups indicate that selective fusions which are stopped short at TV can give similar functional results to those fusions stopped at SV.
Adding-on phenomenon(AO) is one of the common complications after STF in AIS curves, which often leads to poor clinical outcomes.8,24 This was first reported by Suk et al. where they found that after STF, the lumbar curve corrected spontaneously in the immediate post-operative period. However, there was an extension of main thoracic curve into spontaneously corrected lumbar curve in the follow-up period. 25 The selection of LIV highly correlated with AO and the incidence increased as the LIV selection moved proximally. 26 The other reasons for AO suggested were over correction of main thoracic curve. 27 Anticipation of AO phenomenon was one of the main arguments by the surgeons group who chose distal LIV(SV) in preference to proximal LIV(TV).Wang et al. studied 10 different factors that may be responsible for AO and found LIV selection and immaturity as the only factors which highly correlated with AO. 27 The authors in this study found that 46 patients(26.7%) out of 172 patients developed AO during follow-up. When the incidence of AO was compared between the two groups, there was no significant difference between the two groups. It is worth noting that studies in TV group did not report of AO except for one study. 14 Tan et al. proposed another hypothesis for the development of AO that this phenomenon may likely be generated due to the residual uncorrected and unsupported rotational deformities of main thoracic curves despite the instrumentation extended to the stable vertebra. 28 There were no incidences of transient or permanent neurological deficits in any of the patients in the entire study. There are reports of coronal and sagittal decompensation after STF in AIS.29,30 However, our study had a total of 12 cases which showed decompensation among all the patients. The overall complications were not significant between the two study groups. The main goal of STF is maintenance of a balanced spine, spontaneous correction of compensatory curves, and saving more mobile lumbar segments. 31 All these goals can be achieved by choosing either SV or TV as the LIV. As the TV allows for the saving of more motion segments, TV can safely be chosen as LIV with similar satisfaction and complication rates to SV as LIV.
A few limitations of this study are noteworthy. All the studies included in the analysis except one are retrospective studies which amount to level III evidence in the literature. Randomised control studies with two arms (SV, TV) would have been ideal to be analysed for this study, but paucity of such evidence in the literature made the authors choose the available evidence for the analysis. Homogeneity of the involved studies in this meta-analysis was questionable in terms of surgical techniques, outcome measures and countries where the studies were done. Though AO phenomenon is the major determinant of choosing the distal fusion levels, our study had only few studies which had AO phenomenon as major outcome. More studies concentrated on this complication are warranted for better understanding of the distal fusion level. Majority of the literature involved in this review is recent which indicates that a lot of research is being done in the recent times on these topics of ambiguity and this review provides a decent evidence on choosing the distal fusion levels while considering STF for AIS curves.
Conclusions
The current review with evaluation of SV group and TV group as LIV for selective thoracic fusions in AIS reveals a comparable outcome in terms of curve correction, patient satisfaction scores and complication rates. The TV can be safely chosen as the LIV especially in type A and B Lenke 1&2 curves. This saves more lumbar motion segments when compared to SV. Further analysis with good quality RCTs involving both the groups can establish a definite consensus among the surgeons in choosing LIV.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.