
Abstract
Study Design:
Retrospective single-center study.
Objective:
We investigated the risk factors of postoperative shoulder imbalance (PSI) in patients with Lenke type 2 adolescent idiopathic scoliosis (AIS) including the position of preoperative upper end vertebra (UEV).
Methods:
Seventy-five patients with Lenke type 2 AIS who underwent posterior correction and fusion surgeries from 2008 to 2018 were included. We included only patients whose upper instrumented vertebrae were at T2. The patients were divided into 2 groups based on radiographic shoulder height (RSH) at final follow-up, namely PSI group and non-PSI group, and PSI was defined as RSH > 10 mm. UEV, RSH, Cobb angle, curve flexibility, T1 and T2 tilt, correction rate, Risser grade, Scoliosis Research Society-22 scores, and demographic data were compared between the groups using independent t-tests or chi-square tests. Variables with P value < 0.20 in univariate analysis were assessed in logistic regression analysis.
Results:
Thirty-four patients in the PSI group and 37 patients in the non-PSI group were analyzed. Univariate analysis revealed that there were more patients with UEV at T1 (PSI: 85%, non-PSI: 54%, P < 0.01) and Risser grade ≥ 3 (PSI: 88%, non-PSI: 62%; P < 0.05) in the PSI group than in the non-PSI group. Logistic regression analysis revealed that UEV at T1 (odds ratio [OR] = 4.1 [1.2–14.4], P < 0.05) and Risser grade ≥ 3 (OR = 3.9 [1.1–14.5], P < 0.05) are significantly associated with PSI.
Conclusions:
UEV at T1 and Risser grade ≥ 3 at the time of surgery are significant risk factors of PSI.
Keywords
Introduction
Spinal correction and fusion surgery is recommended as treatment for adolescent idiopathic scoliosis (AIS) in patients with curves > 50° with the purpose of preventing the progression of spinal deformity. 1 The objective of the surgical procedure is to obtain a well-balanced spine in the coronal and sagittal planes while preserving motion segments as much as possible. 2 However, correction surgery for AIS is associated with several radiographical problems such as distal adding-on phenomenon, loss of thoracic kyphosis, postoperative coronal decompensation, and postoperative shoulder imbalance (PSI).3-7 Among them, PSI is one of the risk factors of cosmetic dissatisfaction in AIS patients after surgery.7-9
Several studies have reported the risk factors of PSI in patients with Lenke type 2 AIS, and they included preoperative left shoulder elevation, overcorrection of the main thoracic curve, fusion excluding the proximal thoracic curve, and high Risser grade at the time of surgery.10-14 However, no study has described the influence of the position of the upper end vertebra (UEV) of the proximal thoracic curve on PSI (Figure 1). Therefore, we aimed to investigate the risk factors of PSI in patients with Lenke type 2 AIS including the position of UEV of the proximal thoracic curve.
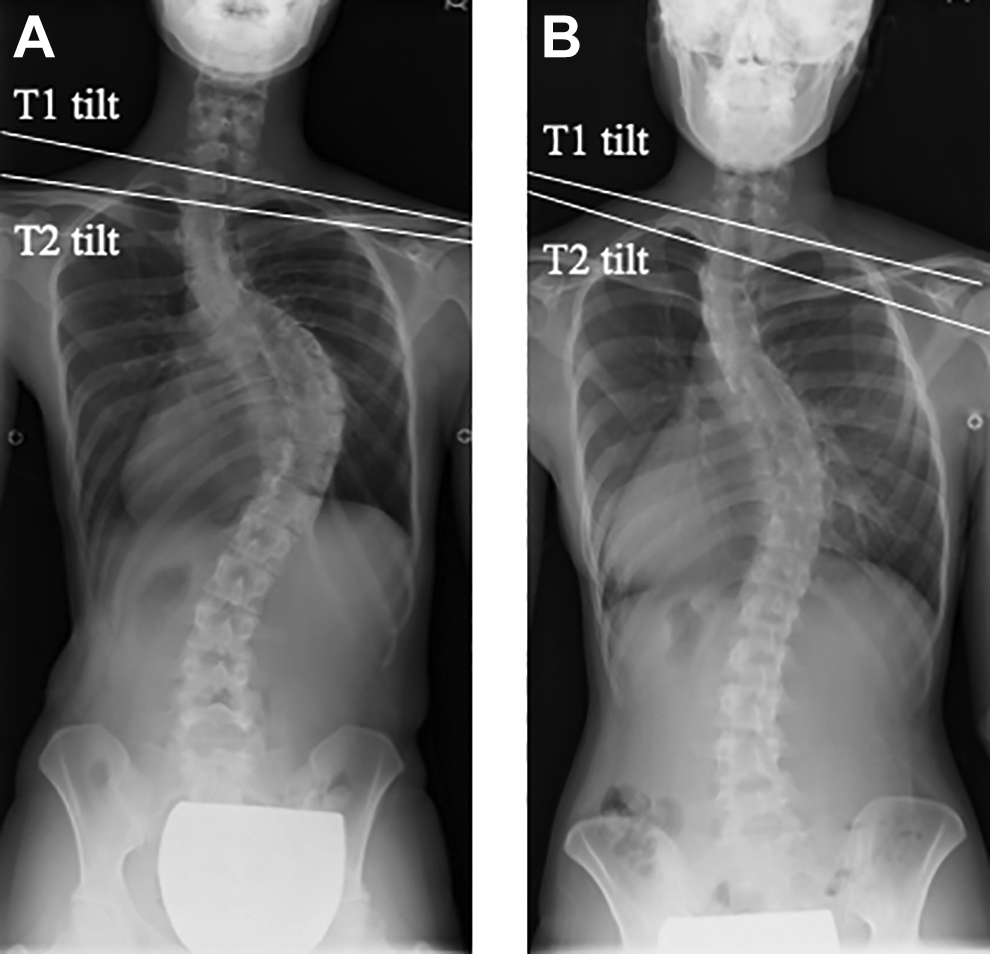
Difference of upper end vertebra of proximal thoracic curve. Inflection point in the frontal plane standing radiograph denotes the upper end vertebra. (A) Upper end vertebra at T1. (B) Upper end vertebra at T2.
Methods
Study Design and Participants
The study was approved by the institutional ethics committee review board, and the approved number was 20 090 042. The informed written consent was received from all patients. This was a retrospective study conducted between 2008 and 2018 at a single hospital in Japan. We investigated 523 AIS patients who underwent posterior correction and fusion surgeries during the period, then patients with Lenke type 2 AIS were included in this study. We only included patients who were followed up for ≥ 2 years and for whom T2 was the upper instrumented vertebrae (UIV) to exclude the effect of UIV selection. We excluded male patients and patients who had previously undergone spine surgery, anterior spinal fusion surgery, combined anterior and posterior spinal fusion surgery, and postoperative distal adding-on associated with PSI. 15 Distal adding-on was defined as an increase of ≥ 5° in the angulation of the first disc below the instrumentation. 16
The patients were divided into 2 groups according to the radiographic shoulder height (RSH) at final follow-up. There were several definitions of PSI including RSH > 10 mm, 15 mm or 20 mm, and the most adopted definition was RSH > 10 mm.2,8,14,15,17-19 In this study, patients with RSH > 10 mm were assigned to the PSI group and the rest of the patients were assigned to the non-PSI group. Demographic data, radiographic data, and clinical outcomes were compared between the 2 groups to determine the risk factors of PSI.
Variables
We collected the following demographic and radiographic data for each patient: height, body mass index, preoperative UEV of proximal thoracic curve, lower end vertebra of main thoracic curve, UIV, lower instrumented vertebra (LIV), RSH, T1 tilt, T2 tilt, clavicle angle, intersection distance of the cervical ribs, coracoid height difference, Cobb angle, curve flexibility, correction rates of proximal and main thoracic curves, sagittal vertical axis (SVA), C2-C7 angle and Risser grade. The radiographic data was evaluated preoperatively and at final follow-up by 2 investigators. Curve flexibility was determined by measuring the curve magnitudes on the preoperative standing posteroanterior radiograph and supine right and left side-bending radiographs, and it was calculated using the following formula: (preoperative standing posteroanterior Cobb angle – side-bending Cobb angle)/preoperative standing posteroanterior Cobb angle × 100 (%). Curve correction rate was calculated using the formula: (preoperative standing posteroanterior Cobb angle – final standing posteroanterior Cobb angle)/preoperative standing posteroanterior Cobb angle × 100 (%). 15 For comparison, the patients were divided into the following 2 groups according to the Risser grade: patients with Risser grades 0–2 and patients with Risser grades 3–5, and this was based on the report of an earlier study. 20
Clinical outcomes were evaluated using the Scoliosis Research Society (SRS)-22 scores determined preoperatively and at final follow-up.
Surgical Technique
All the patients underwent posterior correction surgery with segmental pedicle screw construct. With the exception of the narrowed pedicle at the concave side of the proximal thoracic curve, pedicle screws were inserted at the concave and convex sides using the ball tip technique. 21 Ponte osteotomies were added at proximal thoracic curve to gain maximum correction and inferior facetectomies were added at every level in the fusion area. A 5.5 mm diameter titanium alloy rod contoured to the thoracic kyphosis was then placed on the concave side of the main thoracic curve and rotated for scoliosis correction and thoracic kyphosis creation. An under-bent 5.5 mm diameter titanium alloy rod was placed on the convex side, and segmental distraction and compression were performed to correct the proximal thoracic curve and prevent PSI.
Statistical Analysis
Differences between the PSI and non-PSI groups were compared using the unpaired t-test, chi-square test, or Fisher’s exact test as appropriate. Cronbach’s alpha was used to assess interobserver reliability and the value more than 0.9 was considered as excellent reliability. Cutoff values were determined based on the clinical objective and the result of univariate analysis. P variables < 0.20 in the univariate analysis were included in the multiple logistic regression model. Variables that were highly correlated with each other (correlation coefficient > 0.6) were excluded from the multiple logistic regression model. P variables < 0.05 with a confidence interval (CI) of 95% were considered statistically significant in the univariate analysis and multiple logistic regression analysis. All statistical analyses were performed using the Statistical Package for the Social Sciences (statistics version 25.0., IBM Corp., Armonk, NY).
Results
Descriptive Statistics
In total, 71 patients were included in this study (mean age: 14.1 ± 2.0 years, range: 10–19). Four patients with distal adding-on was excluded from this study. The patient characteristics are summarized in Table 1. Thirty-four patients (48%) were assigned to the PSI group and 37 patients (52%) were assigned to the non-PSI group. The preoperative UEV was T1 in 49 patients and T2 in 22 patients. The mean Cobb angles of the proximal and main thoracic curves were significantly corrected (P < 0.01), and the mean RSH was found to have increased significantly at final follow-up (P < 0.01). There were no significant differences in the mean values of T1 tilt and T2 tilt before surgery and at final follow-up. The selected LIV was T10 in 1 patient (1%), T11 in 7 patients (4%), T12 in 16 patients (48%), L1 in 17 patients (22%), L2 in 19 patients (18%), and L3 in 11 patients (7%). There was an excellent interobserver reliability with Cronbach’s alpha for Cobb angles of the proximal thoracic curve (0.90), Cobb angles of the main thoracic curve (0.94), RSH (0.93), T1 tilt (0.95), T2 tilt (0.98), clavicle angle (0.90), intersection distance of the cervical ribs (0.90), coracoid height difference (0.91), SVA (0.94), and C2-C7 angle (0.93).
Patient Characteristics and Comparison of the PSI and Non-PSI Groups.
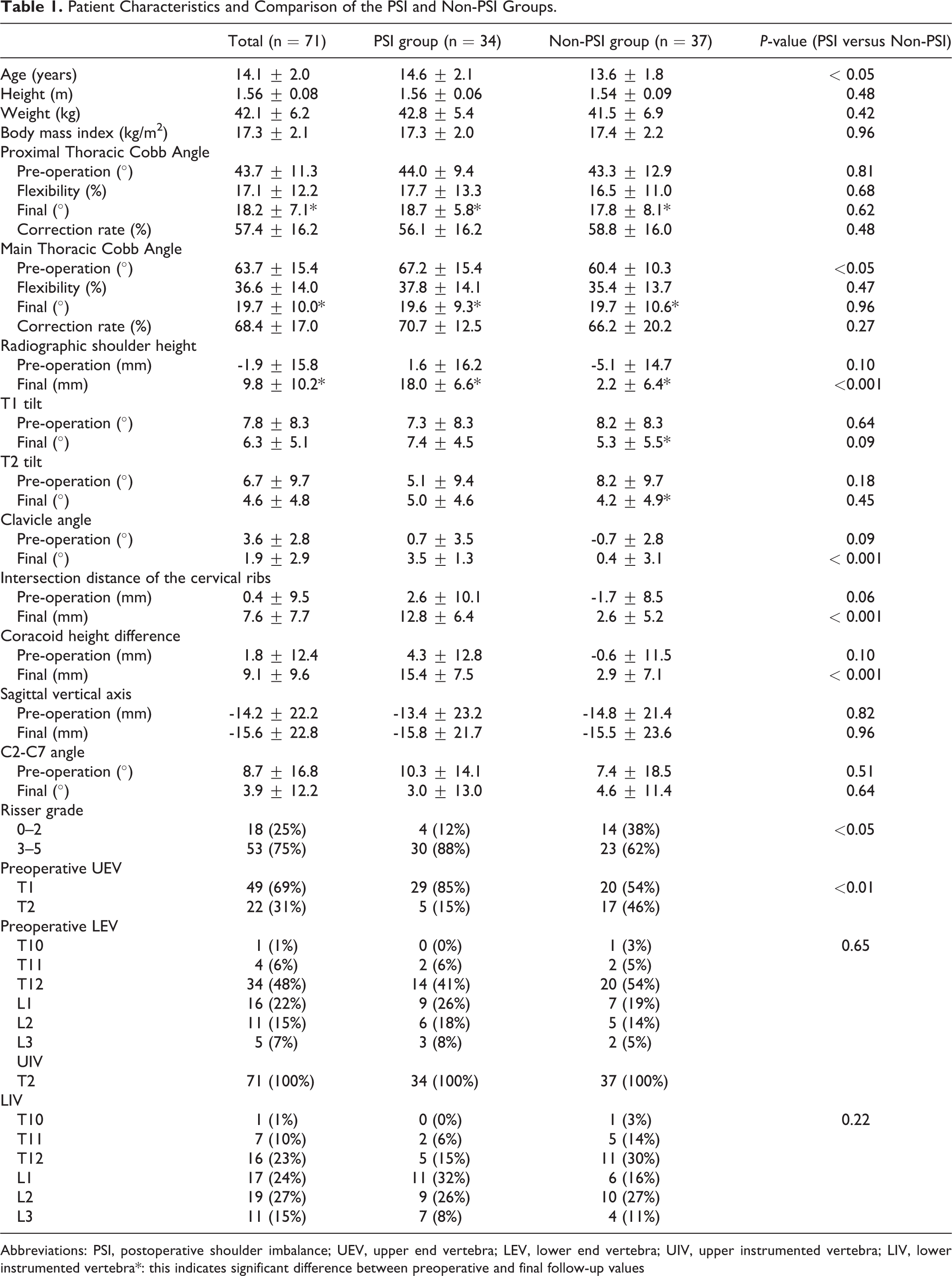
Abbreviations: PSI, postoperative shoulder imbalance; UEV, upper end vertebra; LEV, lower end vertebra; UIV, upper instrumented vertebra; LIV, lower instrumented vertebra*: this indicates significant difference between preoperative and final follow-up values
Univariate analysis revealed that there were more patients with UEV at T1 (PSI: 85%, non-PSI: 54%; P < 0.01) and Risser grade ≥ 3 (PSI: 88%, non-PSI: 62%; P < 0.05) in the PSI group than in the non-PSI group. Regarding preoperative radiographic parameters, the mean Cobb angle of the main thoracic curve, RSH, clavicle angle, intersection distance of the cervical ribs, and coracoid height difference tended to be larger and the mean T2 tilt tended to be smaller in the PSI group than in the non-PSI group. Regarding radiographic parameters at final follow-up, the mean T1 tilt tended to be higher in the PSI group than in the non-PSI group (PSI: 7.4 ± 4.5°, non-PSI: 5.3 ± 5.5°; P = 0.09), but the mean Cobb angles of the proximal and main thoracic curves and the mean T2 tilt were comparable in both groups. The mean clavicle angle, intersection distance of the cervical ribs, and coracoid height difference were significantly higher in the PSI group than in the non-PSI group. There were no differences in the preoperative and final SVA and C2-7 angle between the 2 groups.
There were no differences in the preoperative and final SRS-22 scores, in total or in any domain, between the 2 groups (Table 2).
Postoperative Shoulder Imbalance and SRS-22 Outcome Scores.
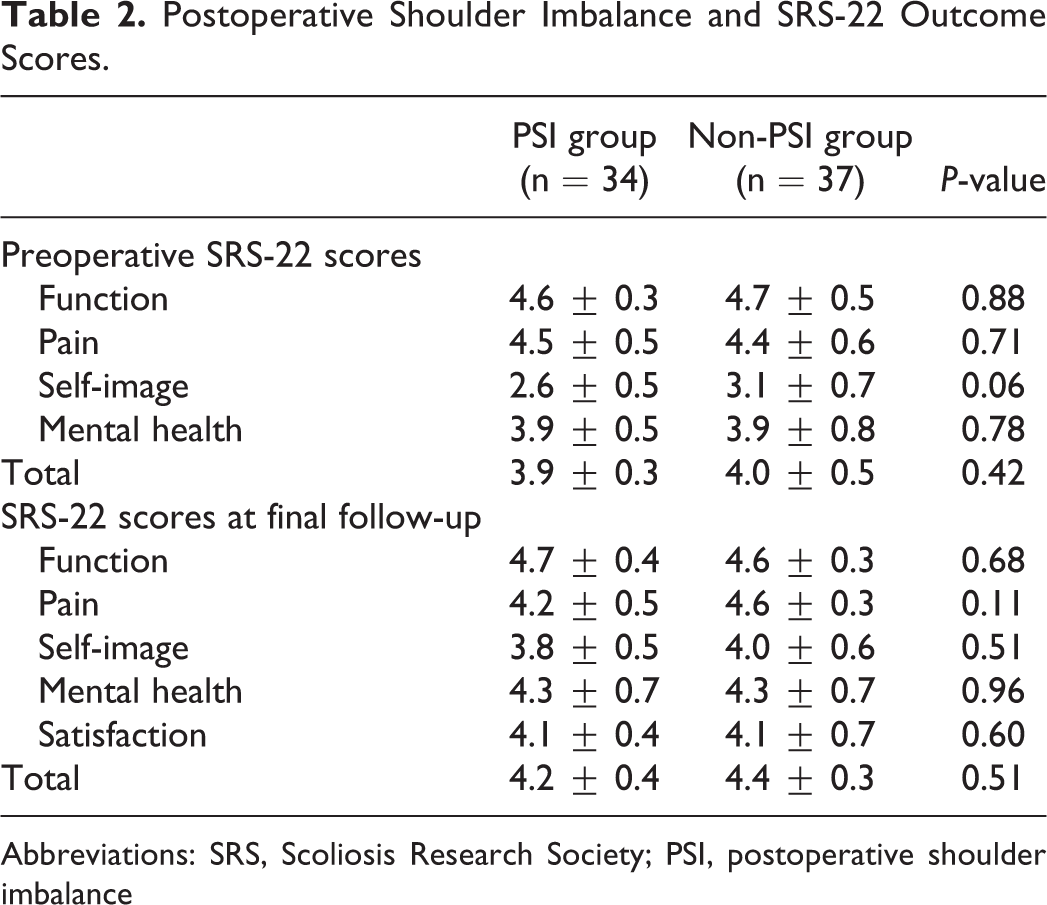
Abbreviations: SRS, Scoliosis Research Society; PSI, postoperative shoulder imbalance
Multivariate logistic regression analysis revealed that, of the variables with P < 0.20 in the univariate analysis (which include UEV at T1, Risser grade ≥ 3, RSH, T2 tilt, and Cobb angle of main thoracic curve), preoperative UEV at T1 (OR = 4.1 [95% CI: 1.2–14.4], P < 0.05) and Risser grade ≥ 3 (OR = 3.9 [95% CI: 1.1–14.5], P < 0.05) are significant risk factors of PSI (Table 3). Preoperative clavicle angle, intersection distance of the cervical ribs, and coracoid height difference which were highly correlated with preoperative RSH (correlation coefficient: 0.62, 0.70, 0.97, respectively), and age that was highly correlated with Risser grade (correlation coefficient: 0.69), were excluded from the multivariate logistic regression analysis.
Logistic Regression Analysis for Postoperative Shoulder Imbalance.
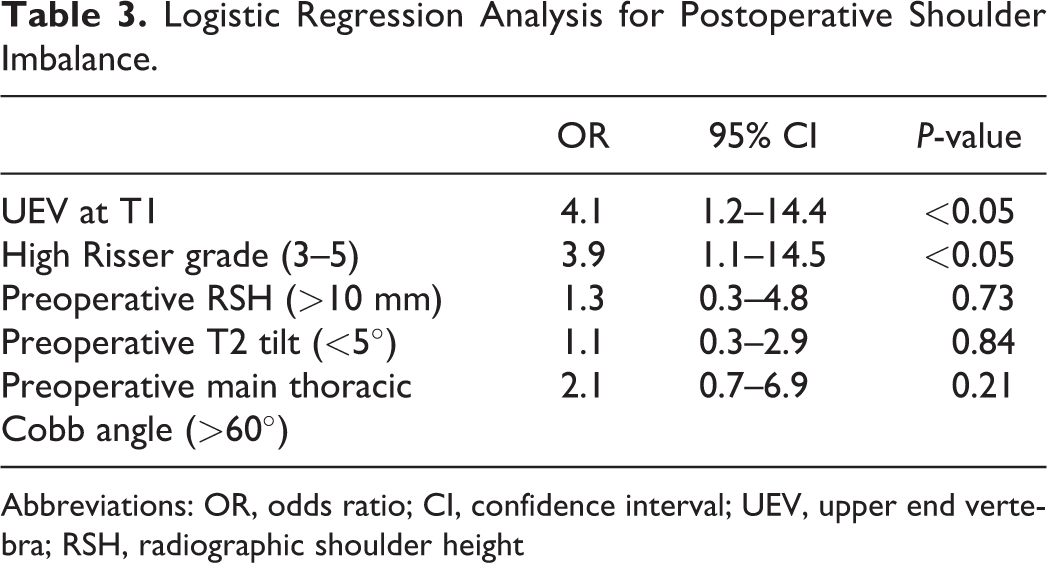
Abbreviations: OR, odds ratio; CI, confidence interval; UEV, upper end vertebra; RSH, radiographic shoulder height
Case Presentation
A 16-year-old female patient with Lenke type 2 AIS underwent posterior correction surgery with segmental pedicle screw construct. Her preoperative RSH was 2.0 mm, UEV of proximal thoracic curve was T1, and Risser grade was grade 4. The proximal thoracic curve was corrected from a Cobb angle of 52° to 29° and the main thoracic curve was corrected from a Cobb angle of 76° to 29°, but her RSH was 25.1 mm at final follow-up. She was assigned to the PSI group (Figure 2).
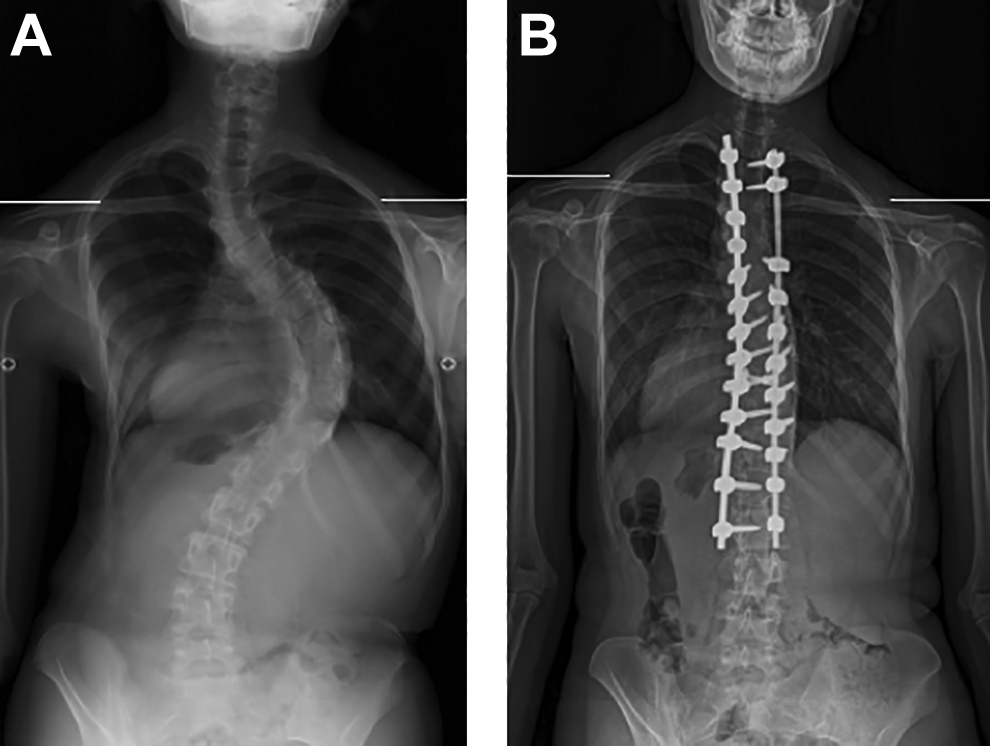
A 16-year-old female patient with postoperative shoulder imbalance. (A) Preoperative radiographic shoulder height is 2.0 mm. (B) Final radiographic shoulder height is 25.1 mm. Preoperative upper end vertebra of proximal thoracic curve is T1.
Discussion
UEV of proximal thoracic curve at T1 was found to be a significant risk factor of PSI. Previous reports showed that extension of the fusion to T1 is not recommended for type 2 AIS, due to increased operative time and blood loss, and upper extensor muscle dissection.22,23 A longer skin incision is needed for unencumbered visualization of the entire dorsal surface of the laminae for pedicle screw insertion at T1 than those at T2 or below, since transverse pedicle angle from midline at T1 is the widest in the thoracic spine between 25° and 35°. 24 In addition, the malpositioned screw at T1 may injure the nerve roots that will cause critical neurological deficit of the motion in hand. 25 However, the transverse pedicle width at T1 is the widest in the upper thoracic spine, and T1 pedicle screw might be a rigid UIV fixation. 24 Then, the extension of the fusion up to T1 may be effective solution in correcting the wedging angle between T1 and T2 as well as shoulder balance in patients with UEV at T1,?although sufficient exposure of posterior elements is needed for accuracy of pedicle screw insertion at T1.
Risser grade ≥ 3 was found to be another significant risk factor of PSI. Although the rigid flexibility of scoliosis curves that was more likely observed in skeletally mature patients might induce PSI, 14 no significant differences in curve flexibility and surgical correction rate were observed between the 2 groups in this study. However, several studies have reported that a higher Risser grade is an independent risk factor of PSI.14,17 In addition, if the Risser grade is higher, the ability to compensate for a shoulder imbalance may be reduced, underpinning the correlation between the Risser grade and PSI. 14
Overcorrection of the main thoracic curve, which has been reported to be a cause of PSI. 11 In our series of the patients, we applied maximum correction at proximal thoracic curve by additional Ponte osteotomies and horizontalization of UIV and below to obtain balanced shoulders during surgeries. Nevertheless, PSI was observed in 47% of patients in the present study. Sielatycki et al. suggested that the main thoracic curve should be corrected relative to the amount of correction of the proximal thoracic curve to avoid postoperative left shoulder elevation. 26 Thus, from the present results of the significant risk factors for PSI, the main thoracic curve correction should be adjusted relative to the amount of correction of the proximal thoracic curve and preoperative shoulder balance to avoid PSI considering position of UEV and Risser grade. We should establish a formula which can decide the adequate correction of the main thoracic curve for AIS type 2 before or during surgeries.
Larger preoperative RSH, which has also been reported to be a risk factor of PSI, 10 was not the significant risk factor of PSI in this study. However, preoperative RSH in the PSI group tended to be larger than that in the non-PSI group, and preoperative RSH with the patients with final RSH more than 20 mm was significantly greater than that with the other patients (data not shown). Hence, although it has not been replicated in the present study, larger preoperative RSH should be considered a risk factor of PSI.
There are several limitations to this study. The LIV of the patients ranged from T10 to L3. This variation in LIV may have been caused by various stable vertebrae and lumbar modifiers. Although the patient with postoperative adding-on was excluded from this study, future studies are needed to investigate PSI in patients with unified LIV and lumbar modifier.
In conclusion, UEV of proximal thoracic curve at T1 and Risser grade ≥ 3 were found to be significant risk factors of PSI in patients with Lenke type 2 AIS. Although we still have not yet established the solutions to prevent PSI with high risk for PSI, extension up to T1 and control the correction of the main thoracic curve may be solutions to adjust the amount of intraoperative correction of the proximal thoracic curve, and preoperative shoulder balance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.