
Abstract
High-quality preclinical bioassay models are essential for drug research and development. We reviewed the emerging body-on-a-chip technology, which serves as a promising model to overcome the limitations of traditional bioassay models, and introduced existing models of body-on-a-chip, their constitutional details, application for drug testing, and individual features of these models. We put special emphasis on the latest trend in this field of incorporating barrier tissue into body-on-a-chip and discussed several remaining challenges of current body-on-a-chip.
Introduction
Current pharmaceutical industry is plagued by low-quality preclinical test outcomes, which is mainly caused by the lack of proper drug bioassay models.1–5 For instance, the results taken from animal models often fail to predict a drug’s efficacy and toxicity in clinical trials due to physiological differences.4,6–9 Furthermore, animal models are costly, time-consuming, and raise ethical controversy.4,10 Another approach is to utilize traditional cell culturing models by culturing or co-culturing cells or organ slices in a two-dimensional (2D) static environment.11,12 However, this method fails to restore the three-dimensional (3D) microenvironment that cells reside in in vivo, where cells interact with other cells and the extracellular matrix of the tissue. This interaction has been proven to be crucial for the cell’s sound functionality and physiological behavior.5,13,14 What is more is that this model cannot provide the essential physiological microfluidic environment that is important for proper cellular growth, differentiation, migration, and patterning.15–17
From Organ-on-a-Chip to Body-on-a-Chip
Researchers developed the organ-on-a-chip technology with the combination of microfabrication technology and bioengineering technology.18–32 Applying this technology, researchers are able to culture cells on chips that are set in a microfluidic environment with a more physiological tissue fluid ratio, sheer stress, and tissue residence time.22,33–42 This technology also enables less consumption of cells and reagents, which indicates a better potential for industrial high-throughput application. Researchers can better mimic the physiological cellular composition of organs in vivo by co-culturing primary and supporting cells.43–46 However, the overall bioavailability and metabolism of one drug is a complex process, including interaction and cooperation between different organs’ functions, such as the absorption function of the barrier tissue, metabolism function of the liver, and excretion function of the kidneys.6,38,47 Therefore, researchers attempt to construct and connect multiple organ-on-a-chip into one single microfluidic on-chip system to better mimic the whole body’s response to the ADME of drugs. This system is referred to as body-on-a-chip (or human-on-a-chip or organs-on-chips).48–54
In this review, we introduced the primitive models of body-on-a-chip without a barrier tissue, which could only mimic the metabolism function of different organs and their application for drug testing. Furthermore, we introduced the latest trend in this field of incorporating barrier tissue into body-on-a-chip to mimic the absorption function, existing models of these more sophisticated versions, and their application for drug testing, and discussed several remaining challenges in this field.
Primitive Body-on-a-Chip without Barrier Tissue: Development, Existing Models, and Application
Development of Primitive Body-on-a-Chip without Barrier Tissue
When drugs enter the blood circulation directly, such as through an intravenous injection, apart from direct toxicity on the target organ, indirect drug-induced liver toxicity and toxicity of metabolites by the liver are two main side effects.16,55,56 Organ-on-a-chip technology is not competent to replicate and evaluate this indirect toxicity. Researchers have attempted to overcome this limitation by developing the primitive body-on-a-chip that connects multiple compartments representing target organs, the liver, and other related tissues in a physiological order. Researchers are able to investigate both the direct and indirect toxicities of a target drug by adding the target drug into the culture medium.
Existing Models of Primitive Body-on-a-Chip without Barrier Tissue and Their Application
Microscale cell culture analog
The microscale cell culture analog (mCCA) system is the first body-on-a-chip model to investigate multiorgan interactions in drug testing.14,34,57 The model is fabricated on a silicon chip with multiple chambers mimicking different organs on it. Chambers are interconnected by microchannels in a physiological order to mimic connections between different organs by blood vessels in vivo. The recirculating culture medium in microchannels, which is powered by an external peristaltic pump, serves as the blood surrogate. By adding a target drug into the culture medium, researchers are able to investigate the effect of the drug’s toxicity on different organs and the effect of physiological upstream organs’ metabolites on downstream organs. A significant advantage of the mCCA against former models is that the developers have incorporated multiple sensors into the model. This improvement enables mCCA to provide rigorous parameters for researchers to evaluate the kinetics of a drug’s metabolism more accurately, rather than just mimic the rough response to a drug. The data obtained from mCCA could thus provide more detailed information, such as half-life and EC50 (concentration for 50% of maximal effect), for further animal or clinical experiment design. Researchers first utilized a four-chamber (lung–rat lung type II epithelial cell, liver–human hepatocyte, other tissue–no cell, fat–no cell) mCCA system to study the toxicity of naphthalene. 34 Results showed that naphthalene was first metabolized into its reactive metabolites in the liver chamber and then circulated into the lung chamber, causing toxicity, which was indicated by the depletion of glutathione in the lung cells. The mCCA system was further improved and applied for different drug testing; for detailed information, refer to Table 1 .
Development of mCCA without Barrier Tissue.
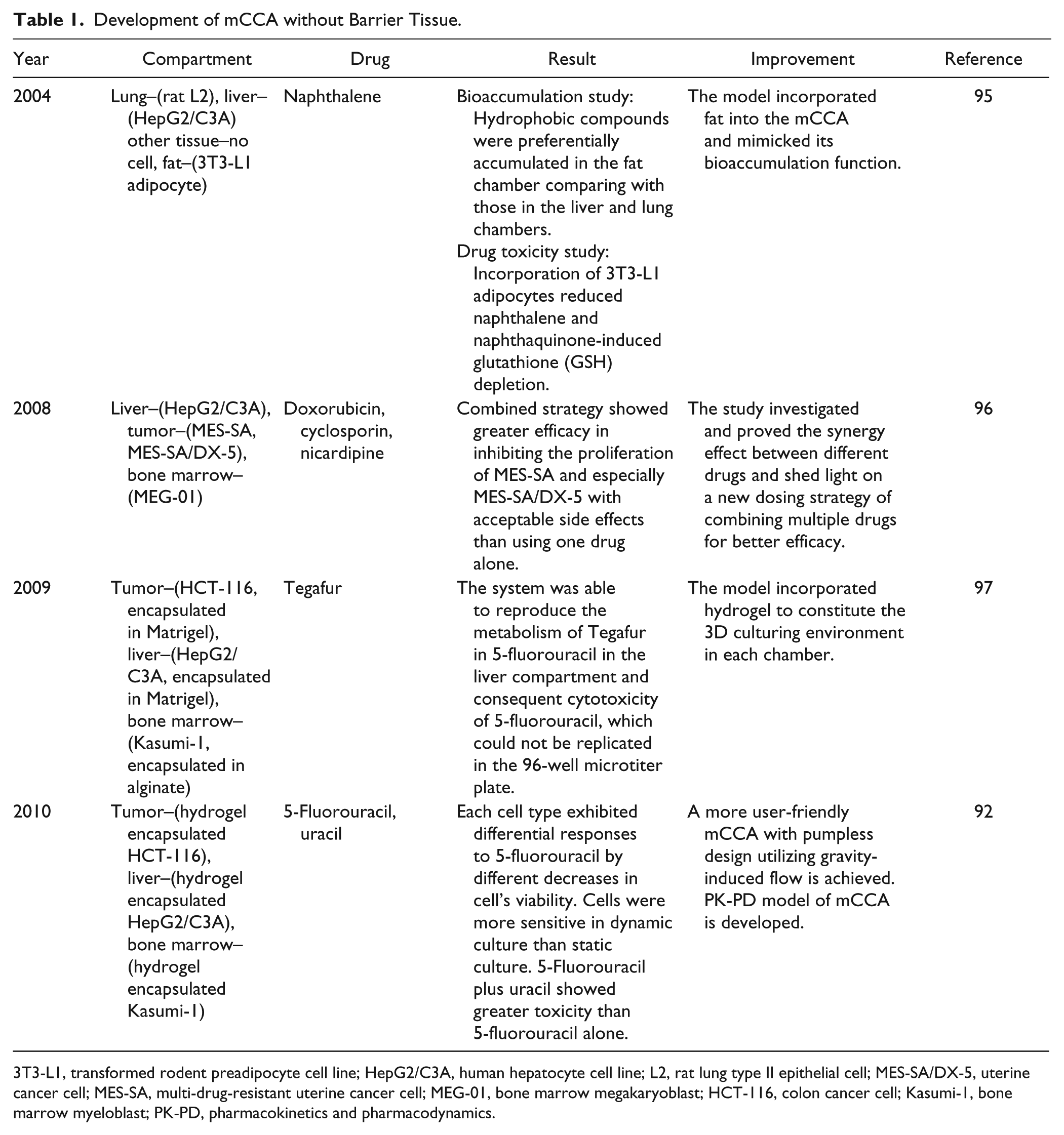
3T3-L1, transformed rodent preadipocyte cell line; HepG2/C3A, human hepatocyte cell line; L2, rat lung type II epithelial cell; MES-SA/DX-5, uterine cancer cell; MES-SA, multi-drug-resistant uterine cancer cell; MEG-01, bone marrow megakaryoblast; HCT-116, colon cancer cell; Kasumi-1, bone marrow myeloblast; PK-PD, pharmacokinetics and pharmacodynamics.
Multichannel 3D microfluidic cell culture system
A brilliant model further improving the mCCA is the multichannel 3D microfluidic cell culture system (multichannel 3D-mFCCS).58,59 The most significant improvement achieved by this model is the creation of a cell-specific microenvironment in each compartment. Human tissue’s cells reside in their specific physical environment in vivo, which possesses a different constitution and concentration of cytokines, enzymes, and other chemical substances. Although all the tissues are connected by blood circulation, each tissue is able to maintain its specific cellular microenvironment, which is critical for the cells to perform their physical functions normally. Former models could not mimic specific microenvironments because all the compartments share one fluidic circulation. This situation leads to identical microenvironments in each compartment, which will further compromise the cells’ normal functioning. Multichannel 3D-mFCCS shows a promising step in overcoming this dilemma. The model connected the liver (C3A), lung (A549), kidney (HK-2), and fat (HPA) together. Concerning the fact that TGFβ1 enhances A549 cell’s function but inhibits C3A cell’s function, gelatin microspheres containing TGFβ1 were specially placed inside the A549 cell’s compartment for controlled release of TGFβ1. The results showed that A549 cell’s function was enhanced, while C3A, HK-2, and HPA cells’ functions were uncompromised, thus indicating that the specific microenvironment in each compartment was successfully achieved. This model is not utilized for drug testing yet; however, its controlled-release technology holds promising potential for further application.
There are many other models developed by different groups. We present the details of these models in Table 2 divided by their application type.
Body-on-a-Chip Models without Barrier Tissue.

3T3-L1, transformed rodent preadipocyte cell line; CYP, cytochrome P450; GBM, glioblastoma multiforme brain cancer cell; HepG2/C3A, human hepatocyte cell line; HepaRG, human hepatic cell line; HHSteC, primary human hepatic stellate cell; L2, rat lung type II epithelial cell; MCF-7, Michigan Cancer Foundation–7 human breast adenocarcinoma cell line; MDCK, Madin–Darby canine kidney cell; NT2, NTera-2/cl.D1 cell, cell line derived from human teratocarcinoma; NMR, nuclear magnetic resonance.
Current Body-on-a-Chip with Barrier Tissue: Development, Existing Models, and Application
Development of Body-on-a-Chip Incorporating Gastrointestinal Duct
The oral drug dosing strategy is relatively easy and safe with better patient compliance, convenience, and comfort.60,61 However, it has been broadly accepted that the multiple functions of the human gastrointestinal duct and first-pass metabolism have a pronounced effect on a drug’s bioavailability, biotransformation, and efficacy. Researchers have already made multiple efforts to mimic the gastrointestinal duct in vitro, such as transwell technology62–67 and microfluidic bioreactor technology.68–71 By incorporating corresponding compartments mimicking the function of the gastrointestinal duct into the primitive body-on-a-chip, researchers are able to evaluate the biotransformation, bioavailability, efficacy, and toxicity of the target drug itself and its metabolites. The data obtained by this advanced body-on-a-chip will serve as a reliable reference for further clinical experiments, such as deciding oral drug dosage, dosing interval, and other parameters.
Existing Models of Body-on-a-Chip Incorporating Gastrointestinal Duct and Their Applications
Micro total bioassay system
In 2009, researchers developed a microfluidic system aiming to mimic the intestinal absorption function for drug testing. 72 Researchers chose Caco-2 as the cell source, and the results showed that cells formed an intact barrier with desirable barrier function and different permeabilities toward different substances. Results obtained by this model were consistent with those obtained by the conventional method. Researchers further connected this microintestine with the microliver and target compartment on one on-chip device to constitute a system called the micro total bioassay system for oral substances bioassay. 73 The microchip consisted of a slide glass and polydimethylsiloxane sheets with microchannels fabricated on it by photolithography. Researchers co-cultured Caco-2 cells (intestine), HepG2 cells (liver), and human breast carcinoma MCF-7 cells (target organ) in their respective compartments in a physiological order. After researchers added a target drug into the system, it first went through the intestine compartment, then the liver compartment, and finally the target organ compartment. Researchers further improved this micro total bioassay system by adding artificial gastric juice, neutralization buffer, and artificial intestinal juice to mimic the functions of the stomach. 74 The rest of the design was the same as the original design. Researchers tested the effects of digestion, absorption, and hepatic metabolism on the bioactivity of anticancer prodrugs, cyclophosphamide and tegafur, with the model. Results obtained by this system were consistent with the known properties of these two drugs, indicating that the micro total bioassay system could serve as a valid tool for oral drug testing.
Microscale cell culture analog
The aforementioned mCCA system was also developed to mimic the gastrointestinal absorption. Researchers designed an independent gastrointestinal duct mCCA and further incorporated it into a multichamber mCCA (lung–L2 cell line, liver–HepG2/C3A cell line, other tissues–no cell). 60 The gastrointestinal duct mCCA consisted of two chambers separated by a microporous membrane on which intestinal Caco-2 cells were cultured to mimic the intestinal wall. The toxicity of acetaminophen was studied with this multichamber mCCA, and results showed that acetaminophen could pass through the Caco-2 monolayer, further causing cell damage in the lung and liver chambers. Researchers further improved the initial design by co-culturing Caco-2 and HT29-MTX (to mimic the function of Goblet cells), which formed a mucus layer covering the Caco-2 cell layer to better mimic the physiological realistic intestinal cell composition. 75 This improved intestine mCCA was tested with an iron bioavailability experiment, 75 a toxicity experiment of acetaminophen, 61 and a toxicity experiment of nanoparticles. 76 Data obtained by this mCCA system were consistent with in vivo measurements using mice, indicating that this mCCA system could be broadly used for studies on orally ingested drugs or chemicals with potential toxicity.
Multiorgan chip
Researchers from Germany developed a body-on-a-chip protocol, also called multiorgan chip (MOC) for different studies.77,78 Respective microchannels, micropumps, and openings for culture compartments were fabricated on a single 2 mm high polydimethylsiloxane layer that was boned to a glass microscope slide by low-pressure plasma oxidation. Several different variations of MOC were fabricated to culture 3D tissues derived from cell lines, primary cells, or biopsies of various human organs. 78 Researchers studied the oral substance exposure by co-culturing liver (HepaRG cells, HHSteC) and intestine (primary small intestine epithelial cells) together and adding troglitazone onto the apical compartment of the intestine chamber. The results showed that troglitazone passed through the intestine and was pumped into the liver. Then it was metabolized and caused damage in the liver, which was indicated by a decrease in the mRNA expression of multiple substances. 77
Finally, an on-chip model connecting liver (HepG2), intestine (Caco-2), and lung (A549) was developed for the study of multiorgan interaction. 79 Epirubicin, irinotecan, and cyclophosphamide were applied orally as anticancer drugs. Results showed this model was able to replicate the physiological phenomenon of these drugs on target organs. This model shows promising potential for application as in vitro model to predict drugs’ pharmacokinetics.
Development of Body-on-a-Chip Incorporating Skin or Lung
Skin and lung serve as the target tissues for drugs to enter the human body, especially for drugs in forms such as cream or spray. For example, most of the clinically applied drugs for asthma are inhaled, such as beclomethasone. The role of the skin and lung is crucial in allergic testing for drugs and cosmetics, for most allergic reactions occur by inhaling or contacting the allergen. 80 Moreover, most environment pollutants attack the human body through skin by contact or through lung by inhalation. Advanced body-on-a-chip with compartments mimicking the function of skin or lung could mimic the whole ADME pathway of substances entering human body through the lung or skin. Thus, it could be applied as drug screening model for dermal or inhaled drugs, allergic test model for new cosmetics, or toxicity test model for environment pollutants. 81 However, as of this writing, there are no publications on incorporating lung tissue as a barrier tissue in body-on-a-chip. With the maturation of lung-on-a-chip and body-on-a-chip technology, we believe the breakthrough toward solving this problem is on the horizon.
As for skin, there are several publications on incorporating skin as a barrier tissue in body-on-a-chip.77,78 Shuler’s team published a pumpless microfluidic platform of a human skin equivalent for drug testing in 2015; it might be incorporated into the mCCA system designed by the team in the future. 82
Existing Models of Body-on-a-Chip Incorporating Skin and Their Applications
The aforementioned MOC system was developed to co-culture skin (human juvenile prepuce biopsy) and liver (HepaRG cell) for long-term cultivation and substance testing. 78 In this study, there were two parallel designs, as tissues directly exposed to fluid flow or tissues shielded from underlying fluid flow by standard Transwell cultures. The latter design was able to provide an air–liquid interface for skin biopsy. For Transwell-based co-cultures, results showed a stable long-term performance over 28 days. Researchers did not perform drug testing for this design. For co-cultures exposed to fluid flow, cross talk between two tissues was observed in 14 days and liver microtissue showed sensitivity to toxicant troglitazone at different molecular levels during a 6-day exposure. This MOC system could be applied to measure the penetration of a substance or cosmetic (e.g., cream) applied on the skin, its effects on the liver, its metabolites by the liver, and furthermore, the effects of the metabolites on the skin.
In 2015, a more advanced design of MOC co-culturing skin (human juvenile prepuce) and liver (HepaRG cell, HHSteC) was published. The most pronounced improvement is the establishment of an entirely endothelialized microchannel system marking a milestone toward blood-perfused MOCs. 77 Endothelialization was achieved by seeding human dermal microvascular endothelial cells isolated from prepuce samples into the MOC. Troglitazone was chosen as the toxicant for systemic substance exposure. Results showed that the endothelial cells covered all the surfaces of the channel circuit and established a confluent monolayer maintaining stability even after 14 days of dynamic co-culture. The liver compartment responded properly to respective troglitazone exposure, as demonstrated by analysis in mRNA and immunohistochemistry level.
Discussion
Although there are multiple developments in different aspects of body-on-a-chip for drug testing, there still remain several general challenges in this field.
Better Quality and Quantity of Organoids in Body-on-a-Chip
Many researchers have made great efforts in improving the quality of organoids in body-on-a-chip, such as co-culturing multiple cells together to better mimic the physiological cellular composition in vivo 75 and using 3D hydrogel scaffolds or other technologies to better mimic the 3D environment.5,37,42,83–85 Furthermore, there is a growing interest in investigating the potential of using stem cells from patients as the cell source to create a patient-specific body-on-a-chip for drug testing or disease model.50,86 On the other hand, it is also necessary to increase the quantity of organoids in body-on-a-chip to better mimic the physiological whole-body response to drugs. Researchers to date have successfully integrated two, three, or four organs together into body-on-a-chip. Interactions between more than four organs have not been achieved. 14 All of the body-on-a-chip models introduced in this review contain the liver compartment, putting special emphasis on the effect of liver’s metabolism on a drug. However, the function of the immune system and the need to incorporate it into a body-on-a-chip system to test both the metabolic and immune toxicity of drugs are understated.80,87–89 Our lab is currently working on this problem of incorporating lymph nodes into body-on-a-chip.
Achieving Entire Vascularization of Body-on-a-Chip
Another critical issue is to achieve the vascularization of body-on-a-chip. A step toward this goal is the endothelialization of microchannels.90,91 Endothelialized microchannels show better capability to mimic the physiological physical environment and endocrine function of blood vessels than microchannels only. A promising step toward this goal is achieved by the aforementioned endothelialized MOC. 77 With endothelized microchannels, together with a more advanced blood surrogate, it is possible to mimic the blood circulatory system in body-on-a-chip.
A More User-Friendly Body-on-a-Chip
Finally, it is essential to develop a more user-friendly body-on-a-chip. Various auxiliary devices such as external pumps and bubble traps, together with the complex preparation process of the system itself, make body-on-a-chip suitable only for skilled researchers. This limits broad utilization of this technology for high-content analysis in the pharmaceutical industry. Many improvements have been achieved on this problem, such as a pumpless design,82,92 disposable design, 93 and paper-supported 3D design. 94
Summary
Body-on-a-chip has irreplaceable advantages compared with current preclinical drug testing tools. Its capability of low cost, low material consumption, high-throughput screening, and less ethical controversy matches perfectly with the requirements of the current pharmaceutical industry. The most valuable advantage of body-on-a-chip is its capability of providing more authentic data for clinical trials, especially data concerning safety, to ensure the safety of clinical trials. With further development, a mature body-on-a-chip will play an important role in drug development by reducing clinical testing failure rates and total investment in the pharmaceutical industry.
Footnotes
Abbreviations
3T3-L1, transformed rodent preadipocyte cell line; A549, adenocarcinomic human alveolar basal epithelial cell; ADME, absorption, distribution, metabolism, and elimination; Caco-2, heterogeneous human epithelial colorectal adenocarcinoma cell; CPT-11, irinotecan; CYP, cytochrome P450; GBM, glioblastoma multiforme brain cancer cell; GSH, glutathione; HCT-116, colon cancer cell; HepaRG, human hepatic cell line; HepG2, human liver carcinoma cell line; HepG2/C3A, derivative of HepG2; HHSteC, primary human hepatic stellate cell; HK-2, human kidney proximal tubular cell line; HPA, primary human preadipocyte; HT29-MTX, subpopulation of HT29 human colonic adenocarcinoma cells selected for resistance to methotrexate; Kasumi-1, bone marrow myeloblast; L2, rat lung type II epithelial cell; MCF-7, Michigan Cancer Foundation–7 human breast adenocarcinoma cell line; MDCK, Madin–Darby canine kidney cell; MEG-01, bone marrow megakaryoblast; MES-SA, multi-drug-resistant uterine cancer cell; MES-SA/DX-5, uterine cancer cell; NT2, NTera-2/cl.D1 cell, cell line derived from human teratocarcinoma; PK-PD, pharmacokinetics and pharmacodynamics; TGFβ1, transforming growth factor beta 1
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the National Natural Science Foundation of China (31200730).