
Abstract
The aim of this study was to establish that laboratory testing may be impaired by pouring and sorting of centrifuged tubes into a bulk input module. The values of 17 analytes, including albumin, aspartate aminotransferase (AST), bilirubin, urea nitrogen, C-reactive protein (CRP), calcium, chloride, cholesterol, creatine kinase (CK), creatinine, ferritin, glucose, lactate dehydrogenase (LDH), potassium, sodium, total protein, and thyroid-stimulating hormone (TSH), were measured in 29 centrifuged serum samples collected in tubes with gel separator and paired centrifuged lithium-heparin samples collected in tubes with gel separator, with (S-BIM) or without (S-NO-BIM) being poured and sorted by a bulk input module (Inpeco, Lugano, Switzerland). In serum tubes, significant differences were observed in S-BIM values of albumin, AST, cholesterol, ferritin, glucose, LDH, potassium, and sodium compared with S-NO-BIM, with bias of LDH exceeding the total allowable error. In lithium-heparin tubes, statistically significant differences were observed in S-BIM values of all parameters, except urea nitrogen, CRP, and sodium, compared with S-NO-BIM. The percentage bias of AST, LDH, glucose, and creatinine exceeded the total allowable error. These results demonstrate that check-in and sorting of centrifuged serum and lithium-heparin tubes may be unsuitable using a bulk input module.
Introduction
Laboratory automation represents a major opportunity for optimization of several activities in the preanalytical and analytical phase and for increasing the overall quality of diagnostic testing. 1 The current market of in vitro diagnostics provides a kaleidoscope of flexible approaches, which can meet the needs of virtually all laboratories. 2
The check-in and sorting of primary blood tubes represent critical issues in laboratory efficiency. Several types of automatic instruments hence have been developed for check-in and sorting of primary blood tubes, 3 some of which are based on robotic arms that lift the specimens from an input rack, read the barcode, and determine the route of the tubes according to information provided by the laboratory information system (LIS). Another solution for check-in and sorting of primary blood tubes is represented by so-called random loading modules or bulk input modules (BIMs). In this specific type of instrumentation, the tubes are poured into the sorter’s hopper and then re-collected from sorting destinations (i.e., “bins”) in stand-alone devices or directly placed into belts or other conveyers when the input module is integrated within total laboratory automation (TLA) ( Fig. 1 ). These modules have some obvious advantages over traditional robot sorters, since they do not require that tubes are preliminarily placed within input racks, there is less need for human intervention since they do not need to be continuously emptied, and they are much faster and less prone to malfunctioning due to the lack of complex technology (i.e., robots arms). It is noteworthy, however, that the introduction of blood tubes within the BIM also carries some hypothetical risks for sample quality.
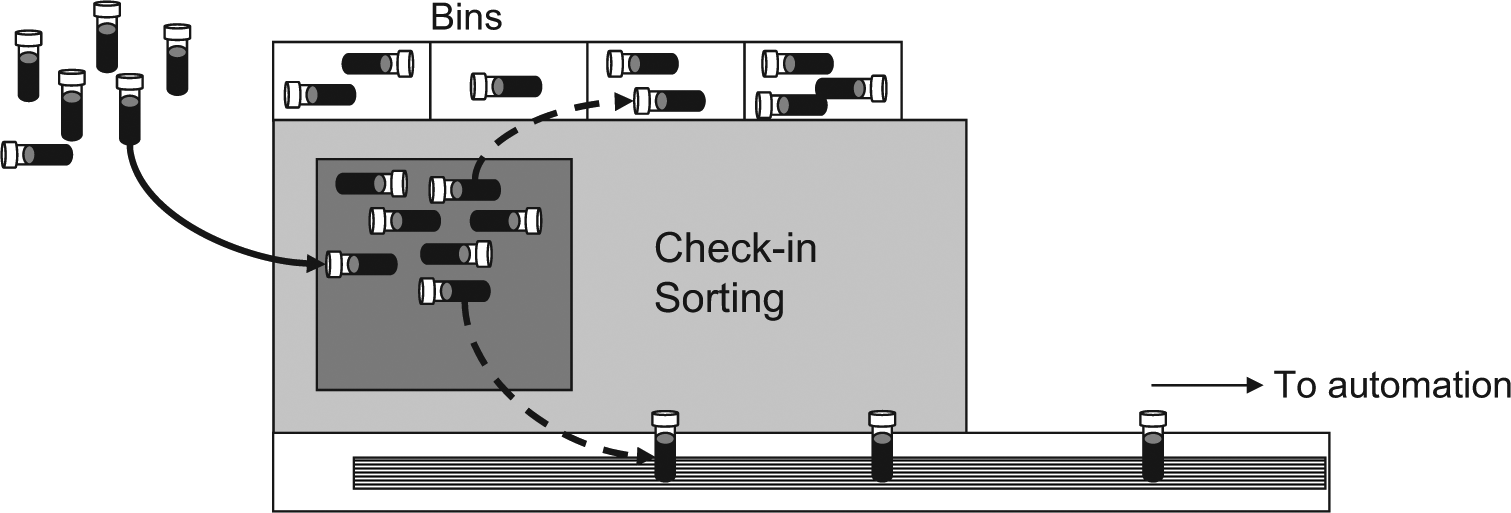
Structure and function of an input bulk module (BIM).
One of the leading paradigms that drives the reorganization of laboratory services entails the creation of networks, where specimens are shipped from peripheral facilities to the central laboratories.4,5 According to the recommendations of the Clinical and Laboratory Standards Institute (CLSI), 6 the specimens should be centrifuged locally when peripheral facilities are located rather far from the central laboratory, so that physical separation of serum or plasma from blood elements by means of physical barriers (typically gel) may prevent the deterioration of several analytes during transportation of whole blood. Once these centrifuged specimens are delivered to the central laboratory, they are also subjected to conventional operations of check-in and sorting, which thus require their introduction into a BIM in laboratories equipped with this instrumentation. Since to our knowledge, no information is available on the stability of the gel barrier when centrifuged tubes are poured and sorted into a random input module, we planned an investigation aimed to establish whether the reliability of testing may be impaired by introduction of centrifuged serum and lithium-heparin tubes into a BIM.
Materials and Methods
Fifty-eight outpatient samples collected in evacuated primary blood tubes were selected from those referred for routine blood testing over a typical working day. Twenty-nine specimens were collected into primary blood tubes with gel containing no additives (Vacuette 5 mL Serum Sep Clot Activator, lot A12100VA; Greiner Bio-One GmbH, Kremsmunster, Austria), whereas the remaining 29 were drawn into primary blood tubes with gel and containing lithium-heparin (Vacuette 5 mL LH Lithium Heparin Sep., lot A131007B; Greiner Bio-One GmbH). Within 1 h after collection, all tubes were placed into a stand-alone centrifuge, where plasma and serum were separated according to the manufacturer’s specifications. The blood tubes were then manually decapped, one aliquot of 1 mL of either serum or plasma was extracted, and the tubes were safely recapped. The 1-mL aliquots of either serum or plasma (i.e., S-NO-BIM) were then manually loaded into clinical chemistry and immunochemistry instruments (Architect C 16000 plus and Architect i2000sr plus; Abbott Diagnostics, Lake Forest, IL) for testing. The recapped blood tubes (S-BIM) were instead poured into a random loading module (BIM [Inpeco, Lugano, Switzerland]; walk-away capability, 800 tubes; throughput, 1000 tubes/h), connected to a track system of total laboratory automation (FlexLab 3.6; Inpeco), 7 and then sorted to the same analyzers used for testing the S-NO-BIM specimens.
The following parameters were assessed in both S-NO- BIM and S-BIM samples: albumin, aspartate aminotransferase (AST), bilirubin, urea nitrogen, C-reactive protein (CRP), calcium, chloride, cholesterol, creatine kinase (CK), creatinine, ferritin, glucose, lactate dehydrogenase (LDH), potassium, sodium, total protein, and thyroid-stimulating hormone (TSH). All measurements were performed using identical lots of reagents and were completed within 2 h from collection.
The difference of values between S-NO-BIM and S-BIM samples was assessed by the Student t test for paired samples and Bland-Altman plots, as well as through direct comparison with the desirable specifications for total allowable error, 8 using Analyse-it (Analyse-it Software Ltd, Leeds, UK). Results were finally expressed as mean and standard error of the mean (SEM). The study was based on preexisting samples, so informed consent or ethics committee approval was unnecessary.
Results
The results of this study are shown in Tables 1 and 2 . With regard to serum tubes, significant differences were observed for S-BIM values of albumin, AST, cholesterol, ferritin, glucose, LDH, potassium, and sodium compared with S-NO-BIM ( Table 1 ). However, when the percentage bias recorded in tubes reintroduced in the bulk was compared with the total allowable error, significant variations over baseline measurements were recorded only for LDH ( Table 1 ). With regard to the lithium-heparin tubes, statistically significant differences were observed in S-BIM values for all parameters except urea nitrogen, CRP, and sodium compared with S-NO-BIM. Interestingly, the percentage bias of four analytes (i.e., AST, creatinine, glucose, and LDH) exceeded the total allowable error in samples processed by the BIM ( Table 2 ).
Values (Mean ± Standard Error of the Mean) of 17 Parameters Measured in 29 Centrifuged Serum Samples without (S-NO-BIM) or with (S-BIM) Being Poured and Sorted by a Bulk Input Module (BIM).
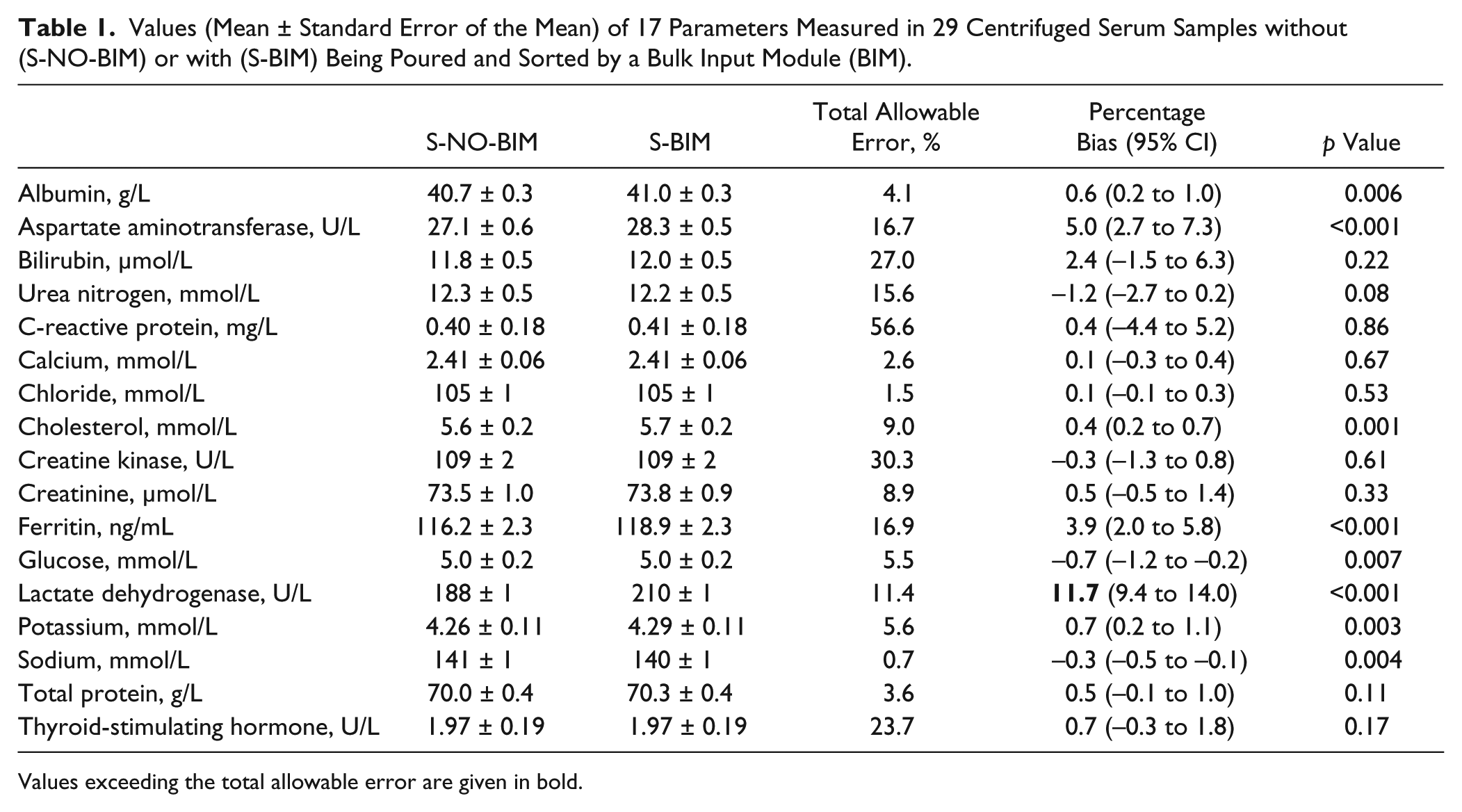
Values exceeding the total allowable error are given in bold.
Values (Mean ± Standard Error of the Mean) of 17 Parameters Measured in 29 Centrifuged Lithium-Heparin Samples without (S-NO-BIM) or with (S-BIM) Being Poured and Sorted by a Bulk Input Module (BIM).
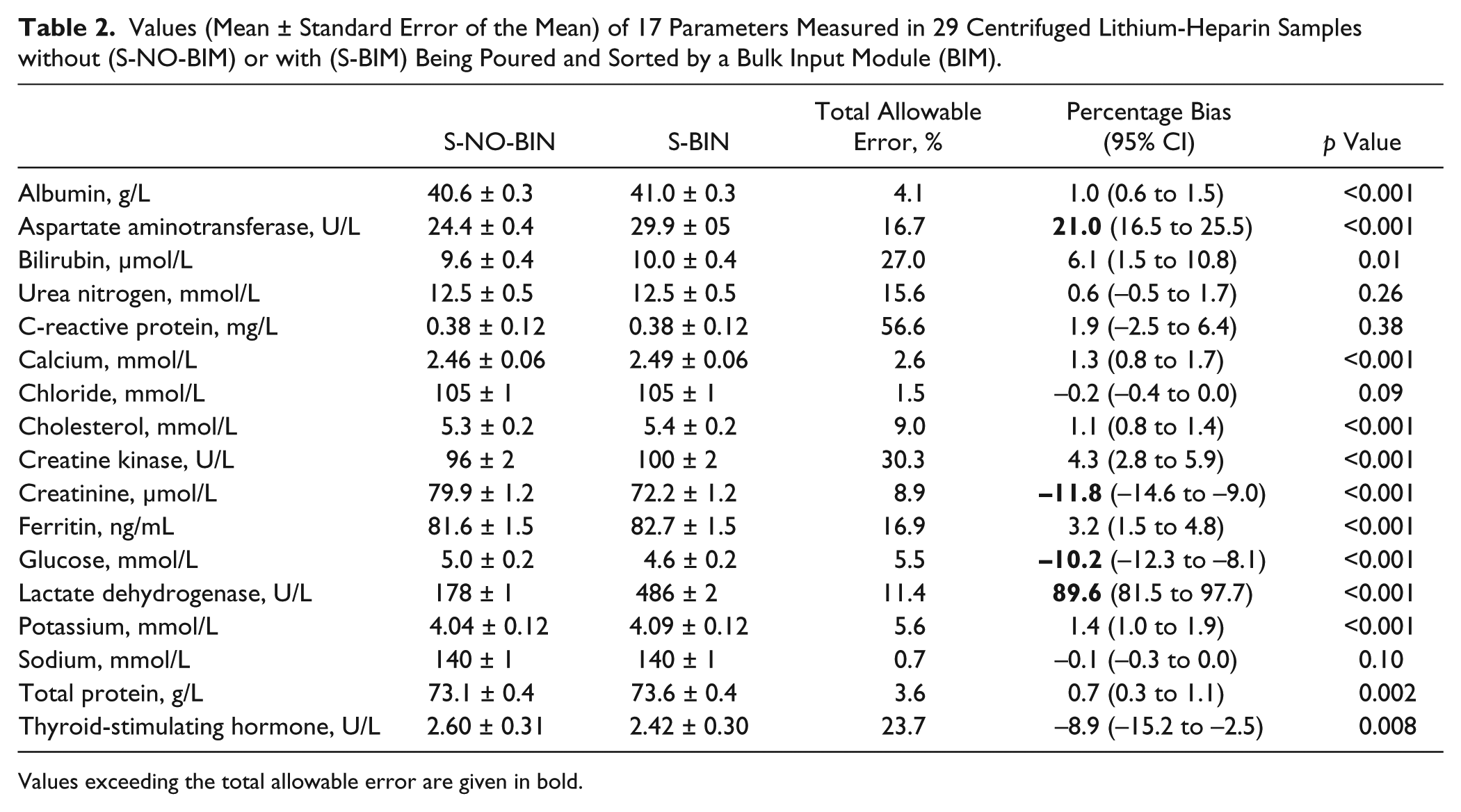
Values exceeding the total allowable error are given in bold.
Discussion
Random input modules for automatic check-in and sorting of blood samples are specifically designed to improve the workflow in clinical laboratories, particularly in the preanalytical phase, and contextually improve operator safety and reduce the chance of errors, which are inherent to manual processing of the specimens ( Fig. 1 ). 9 Regardless of the local organization, random input modules properly blended with automation represent valuable tools for saving human resources and reducing the turnaround time, since blood tubes can be sorted to the right place more efficiently and faster. These remarkable advantages, however, should be balanced by preservation of a high degree of sample quality throughout the process of pouring and sorting of blood tubes into the module.
The results of this study clearly show that check-in and sorting of centrifuged serum and lithium-heparin samples may be unsuitable using random loading modules. This is particularly true for samples collected in lithium-heparin blood tubes, since significant variation could be recorded in 14 of the 17 parameters that we have tested, reaching clinically meaningful bias for AST, LDH, glucose, and creatinine. Interestingly, AST and LDH displayed a remarkable increase (approximately 21% and 90%, respectively), whereas glucose and creatinine were substantially decreased (i.e., approximately −10% and −12%, respectively). Although we did not measure the hemolysis index in these samples, the absolute changes of AST, LDH, and glucose, combined with the slight but significant increase of potassium ( Table 2 ), are highly suggestive of a hemolysis-dependent bias.10,11 It is in fact well established that the values of AST, LDH, and potassium tend to increase after hemolysis, as a consequence of intracellular release from damaged erythrocytes, whereas glucose is metabolized after leakage of intracellular glycolytic enzymes such as hexokinase. 12 Hence, it seems reasonable to suggest that the gel of the blood tubes that we have used in this study was unsuitable to prevent the leakage of intracellular molecules from the blood elements underneath the gel barrier when lithium-heparin samples were poured and sorted into the BIM. A similar but less clinically significant effect was also observed in serum samples, wherein increased values of AST, LDH, and potassium were also recorded, in association with a decrease of glucose concentration. In such case, however, a clinically significant bias was found only for LDH. The discrepancy observed between serum and lithium-heparin tubes may be attributed to the fact that the corpuscular elements entrapped into a stable clot underneath the gel barrier of serum tubes may be less vulnerable to cell injuries occurring when samples are poured and sorted into the BIM.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.