
Abstract
The aim of this study was to assess whether preanalytical management of coagulation samples through an open total laboratory automation system may impair the reliability of routine hemostasis tests as compared with loading of centrifuged plasma specimens directly into the coagulation analyzer for routine testing. Forty inpatient samples were divided into two aliquots. The former was centrifuged and directly loaded in a hemostasis analyzer, whereas the latter was entered into a 16.5 m long track-line system (FlexLab), where it was automatically centrifuged and conveyed to the same coagulation analyzer. An analytically significant difference was found between values of samples directly loaded in the coagulation analyzer and those entered in the track-line system for prothombin time (19.6 ± 1.7 versus 19.2 ± 1.6 s; p < 0.001) and activated partial thromboplastin time (38.0 ± 1.4 versus 37.5 ± 1.3 s; p = 0.021) but not for fibrinogen (305 ± 12 versus 304 ± 12 mg/dL; p = 0.97). Nevertheless, the mean percentage bias of prothombin time (–1.8%), activated partial thromboplastin time (–1.0%), and fibrinogen (0.4%) was modest and always lower than the total allowable error and was thereby considered not clinically significant. The results of this study confirm that connection of coagulation analyzers to track-line systems is a viable solution for modern clinical laboratories.
Introduction
Laboratory automation is becoming a virtually unavoidable solution for saving human and economic resources in a world of limited resources, which is now also facing an unprecedented economic crisis. 1 Laboratory automation is a highly tailored process that spans from automation of only a few activities of the analytical process to automation of a large number of preanalytical, analytical, and postanalytical steps, depending on needs and resources of local facilities.2,3 Total laboratory automation (TLA), defined as the combination of analyzers or work cells with a preanalytical specimen management and transportation system governed by process control software, 4 is a key aspect for improving the efficiency of laboratory services and containing costs. 2 It is noteworthy that the implementation of a fully integrated preanalytical and analytical system not only improves the efficiency of specimen processing and reduces the number of laboratory errors that may occur during sorting, labelling, and aliquoting but also preserves sample quality and even improves the reliability of clinical chemistry testing. 5 Recent studies also suggest that TLA can substantially improve turnaround time (TAT), improve length of stay in the emergency department, and accelerate the overall diagnostic process, thus ultimately improving the quality of care. 6
Despite a constantly growing number of TLA installations worldwide, the transportation of centrifuged coagulation plasma samples by means of tracks, belts, conveyors, and even robots remains an important issue that challenges the minds of laboratory professionals. It has recently been shown that preanalytical processing may in fact influence the quality of results of several coagulation tests, 7 thus confirming that sample preparation and transportation remain critical steps in routine and specialized hemostasis testing. 8 Although some features of laboratory automation are now increasingly embracing areas of laboratory diagnostics that have remained mostly neglected for decades, including hemostasis testing, 9 there is widespread perception that a long and complex track-line system may somehow influence the stability of centrifuged plasma specimens and potentially lead to partial resuspension of cells from the pellet to the upper plasma, especially when traveling at high speed; passing over switches, turnouts, and slots; or colliding with other tubes during transportation. The physical connection of coagulation instrumentation to the TLA thus remains a matter of concern, especially in those laboratories in which coagulation testing has been traditionally performed with stand-alone analyzers. Therefore, the aim of this study was to assess whether preanalytical management of samples for routine hemostasis testing through an open TLA system may affect the reliability of test results as compared with loading of plasma specimens directly into coagulation analyzers.
Materials and Methods
We randomly selected 40 inpatient plasma samples (half of them on oral anticoagulant therapy) collected in evacuated primary blood tubes containing 3.2% buffered sodium citrate (Greiner Bio-One GmbH, Kremsmünster, Austria) from those referred for routine hemostasis testing over one routine working morning. Upon arrival in the laboratory, the samples were divided into two identical aliquots, in 2.0 mL plastic tubes. The former aliquot was centrifuged with a dedicated stand-alone centrifuge according to Clinical Laboratory Standards Institute (CLSI) recommendations (i.e., 1500g for 15 min at room temperature) 10 and directly loaded in the instrument used for routine hemostasis testing (i.e., “direct loading”), whereas the latter aliquot was entered into the TLA (i.e., “track”), where it was automatically centrifuged according to CLSI recommendations by using an identical centrifuge as that used for stand-alone centrifugation and then conveyed to the same coagulation analyzer. In brief, the physical configuration of the TLA of the laboratory where this study was carried out is based on FlexLab 3.6 (Inpeco, Lugano, Switzerland), a track system that consists of a random loading module (BIN), an input/output module, a selective output module, two centrifuges, one decapper, sealer, aliquotor, and desealer module, combined with two clinical chemistry systems (Architect C 16000 plus; Abbott Diagnostics, Lake Forest, IL), three immunochemistry systems (Architect i2000sr plus; Abbott Diagnostics), two integrated hematological analyzers (Sysmex XE5000; Sysmex Inc, Kobe, Japan), two coagulation analyzers (ACL TOP 700; Instrumentation Laboratory, Bedford, MA), and a refrigerated storage and retrieval system. The length of the track from the random loading module and the instrument used for routine coagulation testing is 16.5 m, which is usually covered by samples during routine testing in approximately 105 s, with 13 stops for radiofrequency identification reading. Routine hemostasis testing was performed on the same ACL TOP 700 analyzer and using an identical lot of reagents: RecombiPlasTin (Instrumentation Laboratory) for prothrombin time (PT), SynthASil (Instrumentation Laboratory) for activated partial thromboplastin time (APTT), and FibrinogenC-XL (Instrumentation Laboratory) for fibrinogen. In a previous study, the imprecision has been reported to be comprised between 0.9% and 1.0% for RecombiPlasTin, 1.6% and 2.0% for SynthASil, and 3.5% and 7.7% for FibrinogenC-XL. 9 According to the manufacturer’s specification, the minimal sample volume for routine coagulation testing is approximately 200 µL, so that the use of an aliquot with a lower volume than usual does not influence the quality of data. The total time elapsed between sample collection and processing was always lower than 2 h and thereby in agreement with the current CLSI specifications. 10 The distribution of values was verified with the Shapiro-Wilk test, whereas the difference and the bias were assessed with a Student t test for paired samples and Bland and Altman plots and through direct comparison with the desirable specifications for total allowable error calculated from data on within-subject and between-subject biologic variation, 11 using the software Analyse-it for Microsoft Excel (Analyse-it Software Ltd, Leeds, UK). Results were finally expressed as mean and standard error of the mean. The study was based on preexisting samples, and no additional tests over those originally prescribed were performed, so that informed consent or ethics committee approval were unnecessary.
Results
The values of PT, APTT, and fibrinogen of the samples selected for this study were broadly distributed, thus covering the vast majority of data obtained in routine testing ( Fig. 1 ). An analytically significant difference was found between the values of samples directly loaded in the coagulation analyzer and those entered in the TLA for PT (19.6 ± 1.7 versus 19.2 ± 1.6 s; p < 0.001) and APTT (38.0 ± 1.4 versus 37.5 ± 1.3 s; p = 0.021) but not for fibrinogen (305 ± 12 versus 304 ± 12 mg/dL; p = 0.97). An excellent Pearson’s correlation between values of sample directly loaded in the analyzer and those conveyed through the belt-line system was, however, observed for all parameters: r = 0.999 (p < 0.001) for PT, r = 0.992 (p < 0.001) for APTT, and r = 0.980 (p < 0.001) for fibrinogen, respectively. The mean (and 95% confidence interval [CI]) percentage bias was −1.8% (95% CI, −2.3% to −1.2%) for PT, −1.0% (95% CI, −1.9% to −0.1%) for APTT, and 0.4% (95% CI, −1.2% to 1.9%) for fibrinogen, respectively ( Fig. 1 ). In no case did the bias and its 95% CI exceed the total allowable error for PT (±5.3%), APTT (±4.5%), or fibrinogen (±13.6%). 11
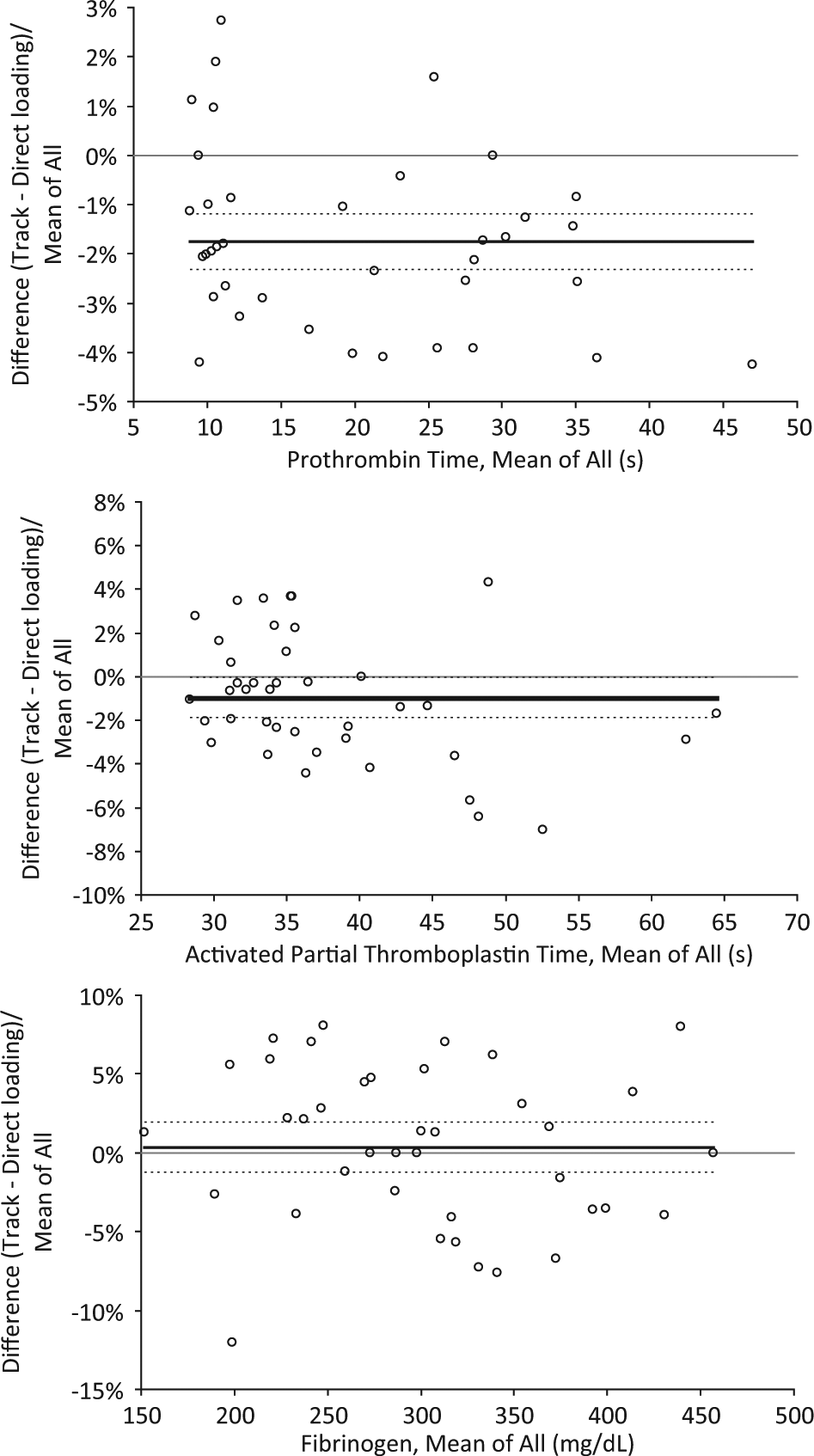
Bland and Altman plots for values of prothrombin time (PT), activated partial thromboplastin time (APTT), and fibrinogen of plasma coagulation samples directly loaded in the coagulation analyzer and transported to the same instrument by the FlexiLab track.
Discussion
Several repetitive and potentially hazardous activities that are typically performed in routine clinical laboratories can lead to operator errors and injuries, causing procedure failures and delayed process. 12 The potential automation of the entire sample processing may hence generate a number of tangible advantages, including tube consolidation, standardization of operating procedures, sample and data traceability, process monitoring and streamlining, consistency and reduction of TAT, prevention of human errors, increase in operator safety and laboratory efficiency, and, last but not least, overall cost reduction. 13
The progressive diffusion of TLA is engendering substantial opportunities to optimize laboratory workflow but is also generating brand new problems. 14 Noticeably, the great advancements that have occurred in TLA over the past decades have mainly targeted the so-called “serum area” and have only marginally involved coagulation testing, which still remains a virtually segregate area in the complex and multifaceted environment of laboratory diagnostics. Only recently has the perspective to combine fully automated coagulation instruments with open automation systems in a physical continuum of preanalytical and analytical modules emerged as a potential organizational solution for hemostasis testing. 15 It is undeniable that the peculiarity of the specimen required for clotting tests (i.e., a sample with lack of physical separation between cells and upper plasma after centrifugation) requires a detailed analysis of the potential impact on test results of introducing plasma specimens within complex models of TLA, thus generating a widespread perplexity about this potential approach.
The results of our investigation using FlexLab 3.6 (i.e., a largely diffused model of TLA) clearly attest that plasma sample processing through an extensive track-line system generates a very modest, constant, and definitely not clinically meaningful bias on results of routine hemostasis testing. In fact, the overall bias that we have recorded was substantially lower than the current quality specifications, thus confirming that the physical connection of coagulation analyzers to open automation systems does not affect sample quality and test results, thus representing a viable perspective for modern clinical laboratories.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.