
Abstract
Denervation by electrocauterization was proposed to be efficient in preventing anterior knee pain (AKP) following arthroplasty. The purpose of this study was to evaluate the effects of patellar denervation (PD) in primary knee arthroplasty. Systematic search was performed in PubMed, ScienceDirect, Cochrane Library, and ClinicalKey databases until July 2022 for published articles. The quantitative analyses were carried out by Review Manager 5.4 software. Twenty-one studies were included. Overall incidence of AKP, visual analog scale (VAS), and knee society score were significantly superior in PD group. Denervation also showed better outcomes in incidence of AKP at each follow-up time point, and in VAS and range of motion (ROM) at ≤3 months. Subanalyses based on depth of electrocautery showed statistically better results with 2–3 mm depth in VAS and PS compared to ≤1 mm. This study concluded that PD might contribute to lower incidence of knee pain. Patients who expect quicker recovery in pain and ROM may benefit from this procedure.
Introduction
Knee arthroplasty is one of the most common surgery globally. Its numbers are expected to increase each year, that by 2030, it was projected to increase by approximately 600% compared to 2005.1,2 Knee arthroplasty is most commonly indicated for and is the method of choice for debilitating knee osteoarthritis. The main objectives are to relieve pain and optimize functional status.3,4 Unfortunately, anterior knee pain (AKP) following arthroplasty was reported in up to 34% patients. 5 This is a concerning health issue as post-arthroplasty pain would have negative impact on patients’ quality of life, daily function, and mental health. 6
Knee pain after arthroplasty has perplexing mechanisms. Various modifications have been proposed to overcome this matter.7,8 Patellar resurfacing was reported to be effective in reducing post-arthroplasty knee pain. However, risk of other complications may also arise from this measure. Patellar resurfacing has been associated with patellar fracture, maltracking, patellar ligament rupture, osteonecrosis, component loosening, etc.9,10
A safer approach, namely patellar denervation (PD), has been suggested. This simple electrocautery procedure was reported to result in comparable outcomes to patellar resurfacing, but without significant complications. 11 However, the benefit of PD is still debatable. In their randomized controlled trial (RCT), Alomran 12 reported PD reduced incidence of AKP, and improved WOMAC score and range of motion (ROM) post-arthroplasty. Meanwhile, another RCT by Kwon et al. 13 concluded that there were no significant outcomes between denervation and non-denervation groups.
Although previous survey revealed that 32% orthopedic surgeon preferred including PD during knee arthroplasty, the advantage of denervation itself has not reached an agreement. 14 The aim of this meta-analysis was to analyze the outcomes of PD in primary knee arthroplasty without resurfacing to provide a better conclusion regarding the benefit of denervation.
Methods
Search strategy
A computerized search was systematically performed in PubMed, Cochrane Library, ClinicalKey, and Science Direct databases in June 2022 for published articles. The following keywords were used for the search: (denervation OR neurectomy OR electrocautery) AND (knee arthroplasty OR knee replacement).
Article selection
The inclusion criteria were: (i) patients underwent primary knee arthroplasty without patellar resurfacing; (ii) subjects with and without PD were groups as experimental and control groups, respectively; (iii) minimal one of these outcomes have to be reported: incidence of post-operative AKP, visual analog scale (VAS), ROM, patellar score (PS), knee society score (KSS), knee society score function (KSSF) subscale, and complications. Exclusion criteria were: (i) studies which included patients with knee deformity, lower limb fracture, or previous surgery of lower limb; and (ii) studies without pre-operative data, aside from incidence of AKP and complications; and (iii) incomplete data.
Two reviewers independently assessed titles and abstracts for initial screening. Full texts of selected articles were then evaluated. Disagreement was resolved by discussion and consensus. When the decision was still not reached, a third reviewer's opinion was sought.
Assessment of risk of bias
The risk of bias of RCT was graded as high, low, or unclear according to the Cochrane Risk of Bias Tool based on the following domains: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other bias. Other bias was defined if there was unbalanced baseline characteristics of subjects between the PD and non-PD (NPD) group.
Data extraction
Lead author, publication year, participants’ characteristics, number of knees, characteristics of electrocautery, and follow-up time were extracted from each included study by two independent reviewers.
Primary outcomes included incidence of AKP and VAS for AKP. Secondary outcomes included ROM, PS, KSS, KSSF, complications, and difference in outcomes by the depth of cauterization. For VAS, ROM, PS, KSS, and KSSF, analyses were carried out by comparing the change from pre- to post-operative values between PD and NPD groups.
Statistical analysis
Risk ratio (RR) and 95% confidence intervals (CI) were calculated for dichotomous variable by using the Mantel-Haenszel method. Mean difference and 95% CI were calculated for continuous variables by inverse variance method. Heterogeneity among studies was measured by I2, for I2 > 50% was considered to represent significant heterogeneity. For incidence of AKP, if studies reported zero events, number of events was changed into one, in order for the application to process the data. To evaluate whether the comparisons of clinical effects between PD and NPD change along with time, subgroup analyses were performed according to follow-up periods ( ≤ 3 months, > 3–12 months, and >12 months). Lastly, subgroup analysis was carried out according to depth of electrocautery. The level of significance was defined as p-value < 0.05. Statistical analyses were performed by Review Manager 5.4 software.
Results
Study selection
The flow of literature searching is shown in Figure 1. Initially, a total of 1719 studies were obtained. After duplicates were removed, titles and abstracts of 1624 studies were screened, and yielded in exclusion of 1592 studies. Thirty-two studies were evaluated for full-text article, and 21 studies were included in qualitative synthesis as well as quantitative analysis in the end.
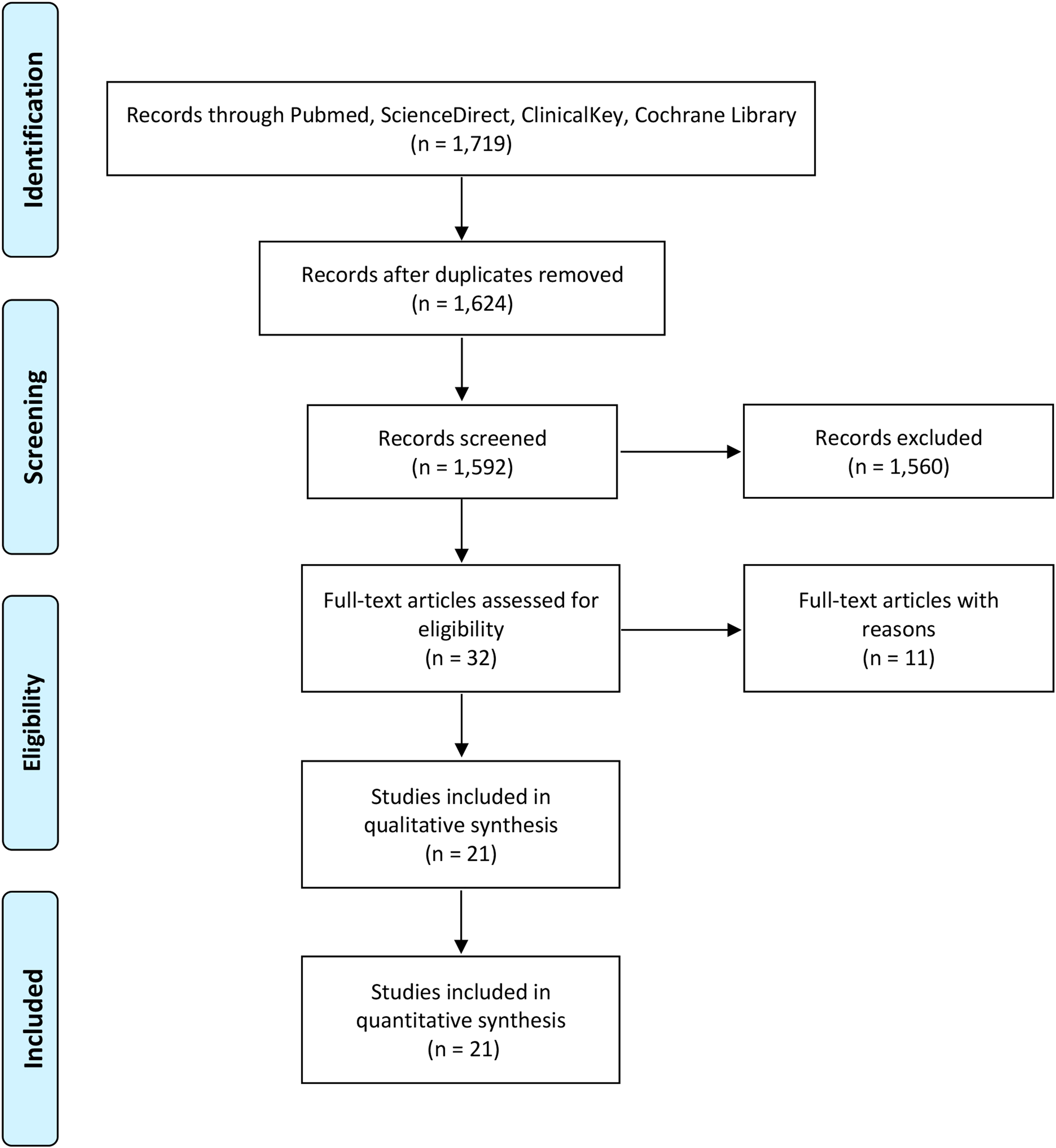
PRISMA flow diagram for study selection.
Study characteristics
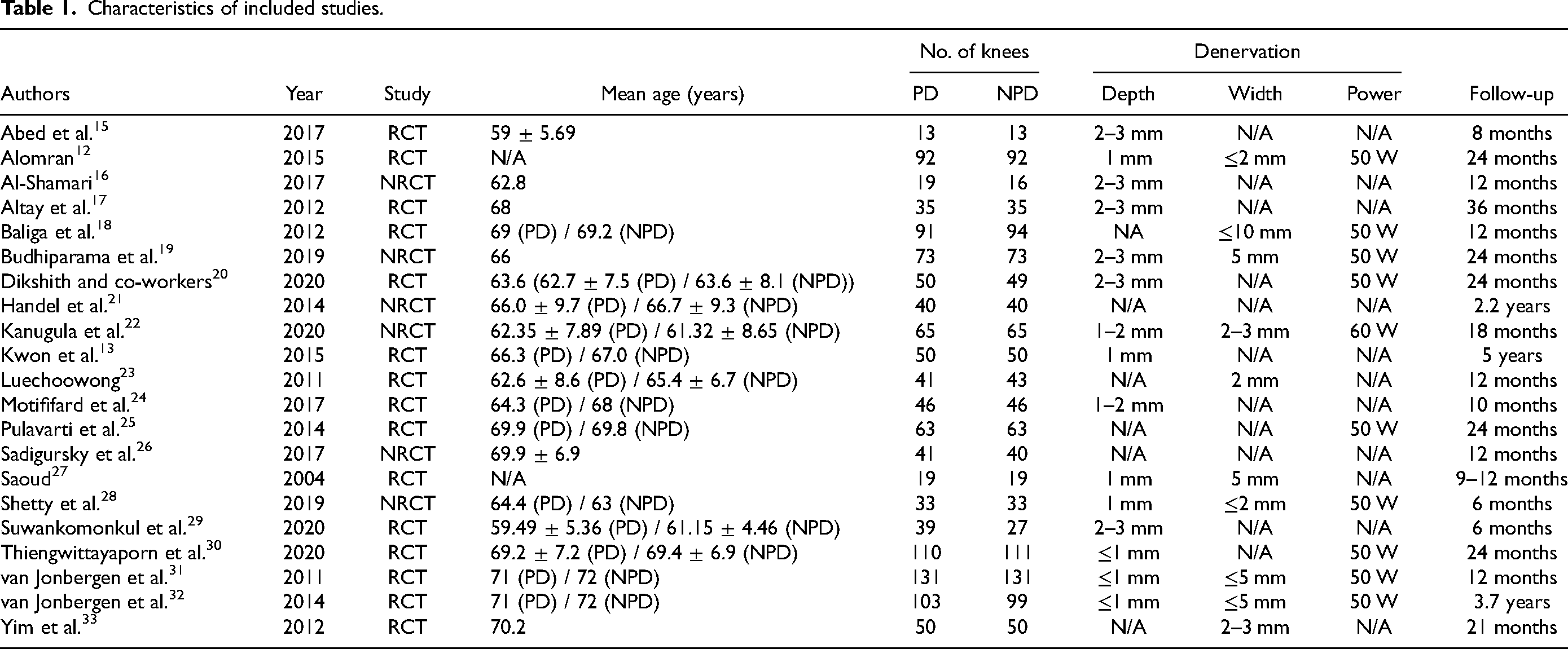
We included 21 studied in the final analysis. The characteristics of each study were presented in Table 1. Arthroplasty was performed in 2393 knees, which were divided into 1204 knees in PD group and 1189 knees in NPD group. Summary of risk of bias of included studies is shown in Figure 2.
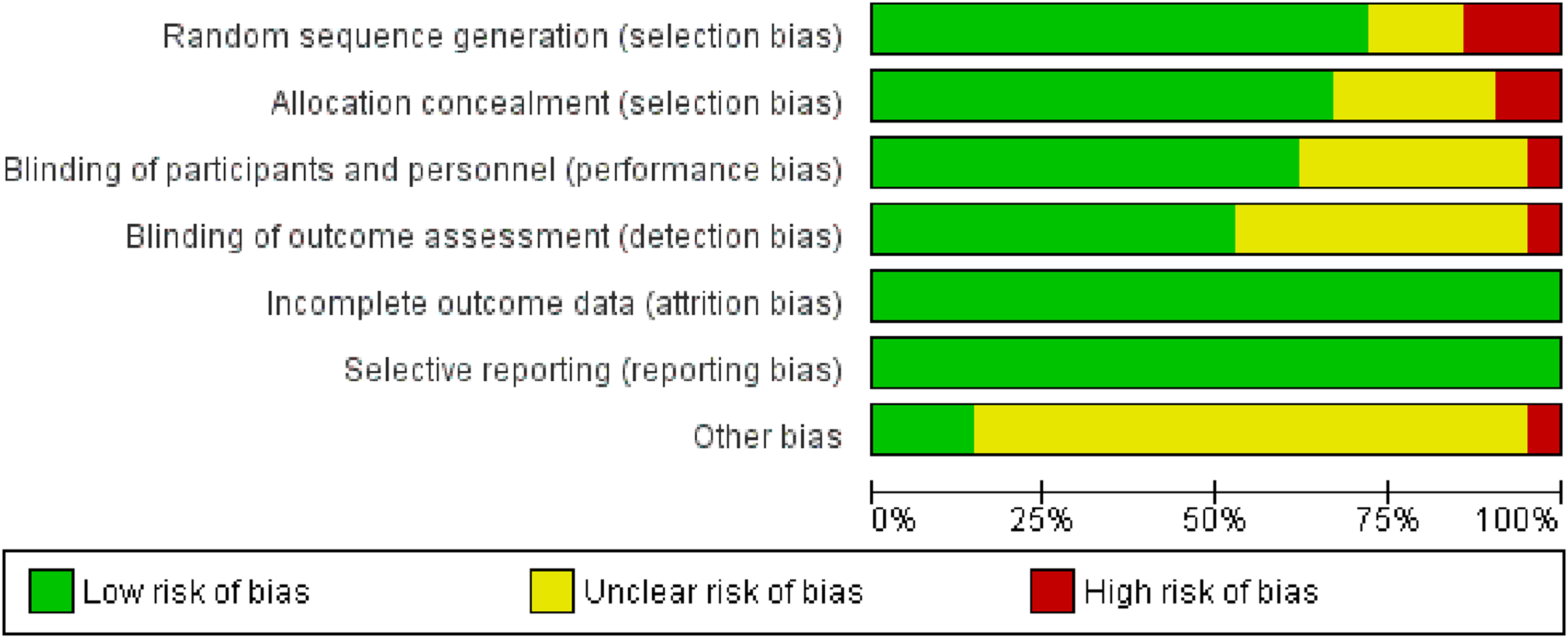
Summary of quality assessment of included studies.
Characteristics of included studies.
Study outcomes
Incidence of AKP
Eleven studies were included for the analysis of incidence of AKP. Only two studies recorded the incidence of AKP at ≤3 months and six studies for incidence at >3–12 months and resulted in fewer incidence of AKP (p = 0.001 and p = 0.0004, respectively) in PD group. For >12 months subanalysis, the analysis of seven articles also showed better performance in PD group. Originally, Thiengwittayaporn et al. 30 reported no AKP in both groups at this period. The overall incidence of AKP was significantly lower in PD group (p < 0.00001), as well as at every follow-up period (Figure 3).
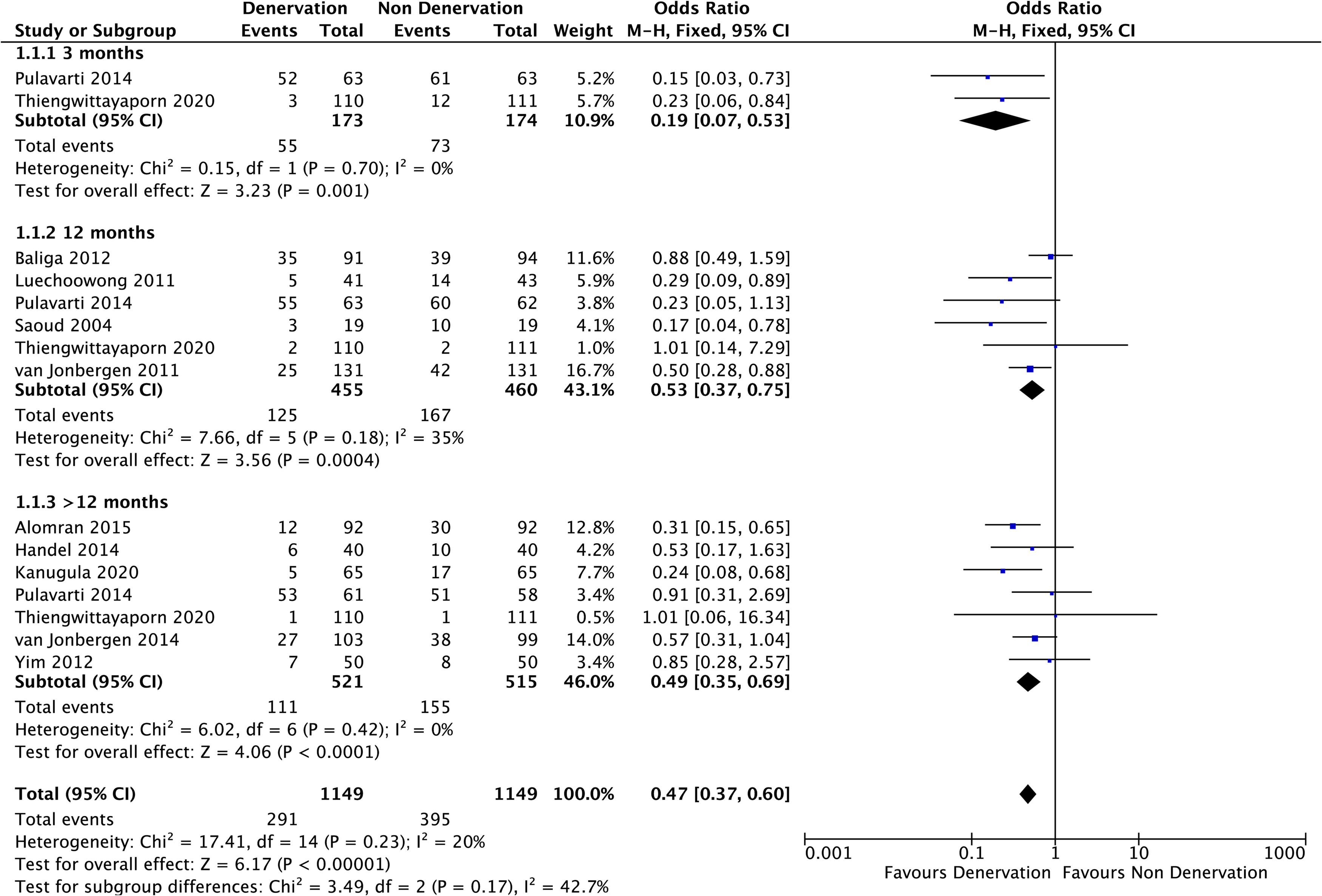
Incidence of anterior knee pain.
Visual analog scale
Figure 4 showed the result of VAS. A total of seven studies were included for VAS. Five studies were involved for <3 months subanalysis, and four studies were included in >3–12 months and >12 months analyses. Al-Shamari et al. also reported VAS during >3–12 months follow-up; however, the data appeared to be an outlier and was precluded from the analysis. Change in VAS was statistically better (p < 0.00001) at ≤3 months, but not significant at 3–12 months and >12 months post arthroplasty (p = 0.26 and p = 0.59, respectively). Pooled analysis showed better alleviation of VAS in PD with significant difference (p = 0.009).
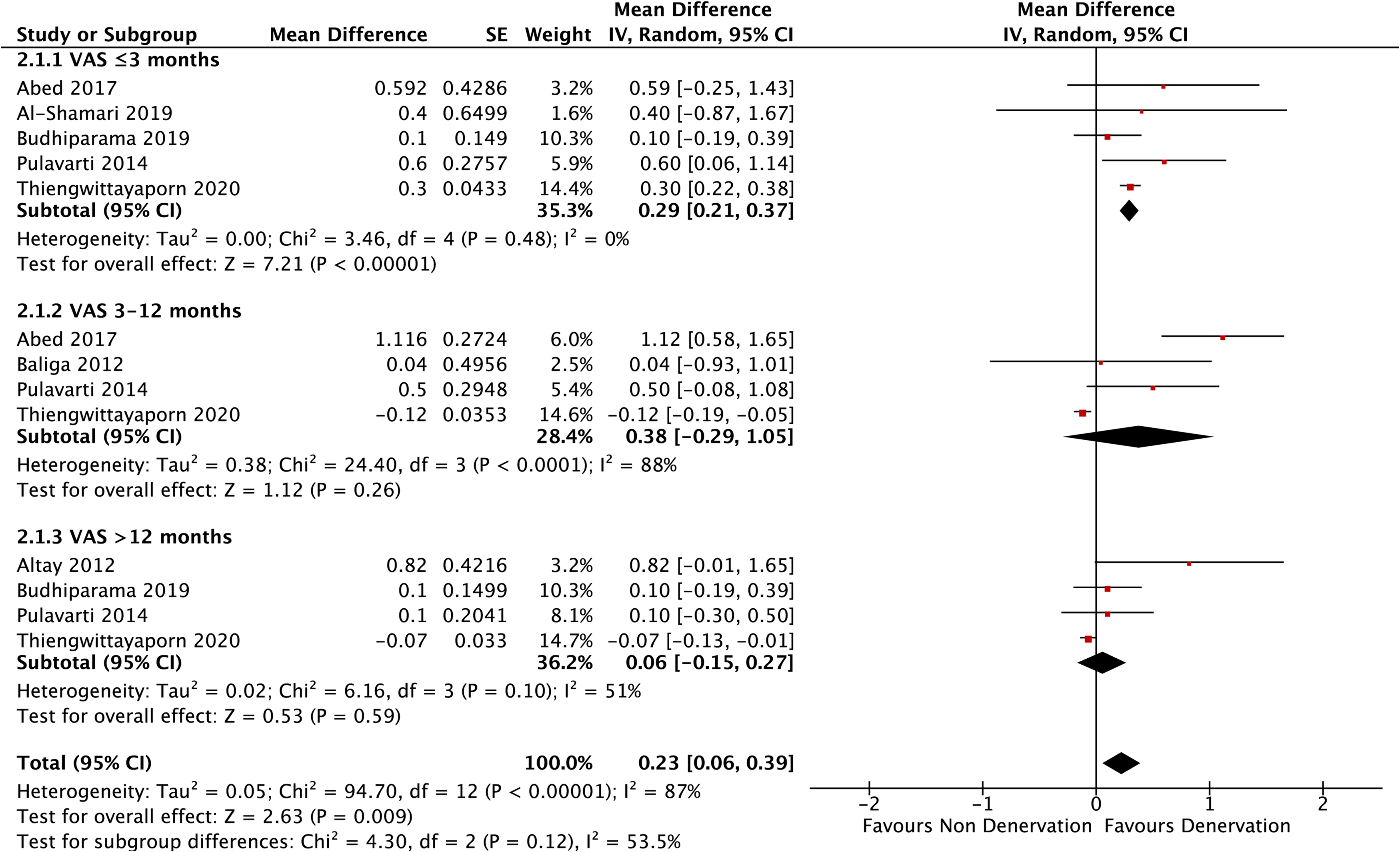
Visual analog scale.
Range of motion
Analysis of ROM is presented in Figure 5. Ten studies involved in the analysis for ROM, which four were used in ≤3 months analysis, four others in >3–12 months, and seven in >12 months. Only ≤3-month follow-up showed a significant improvement of ROM in PD group (p = 0.03). The >3–12-month, and >12-month, as well as overall analyses showed no statistical differences (p = 0.96, p = 0.10, and p = 0.13, respectively).
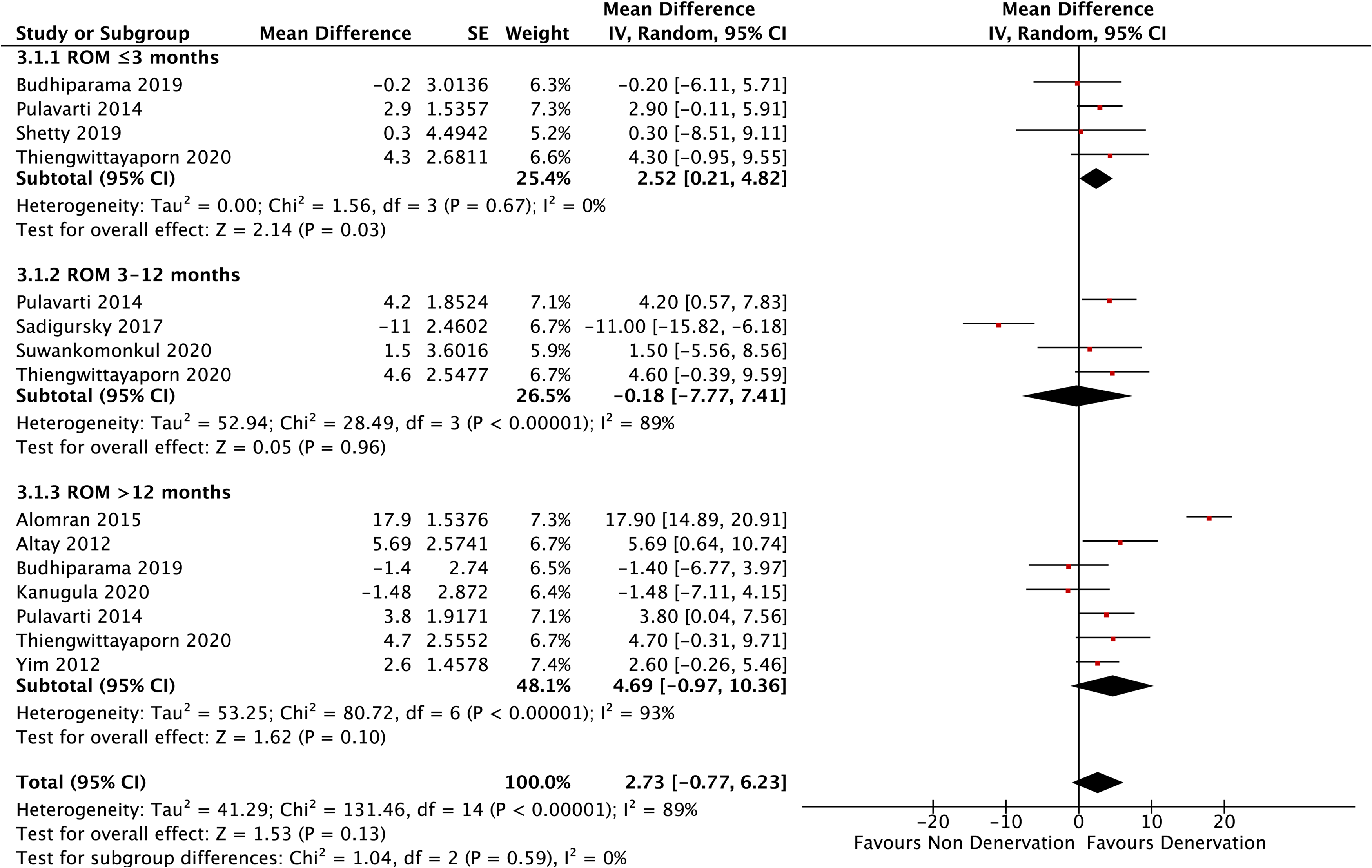
Range of motion.
Patellar score
Subanalyses at ≤3 months and 3–12 months both consisted of four studies, and subanalysis of >12 months consisted of six studies. These subanalyses showed no significant different between PD and NPD (p = 0.42, p = 0.90, p = 0.64, respectively). Pooled analysis also resulted in insignificant difference (p = 0.67) (Figure 6).
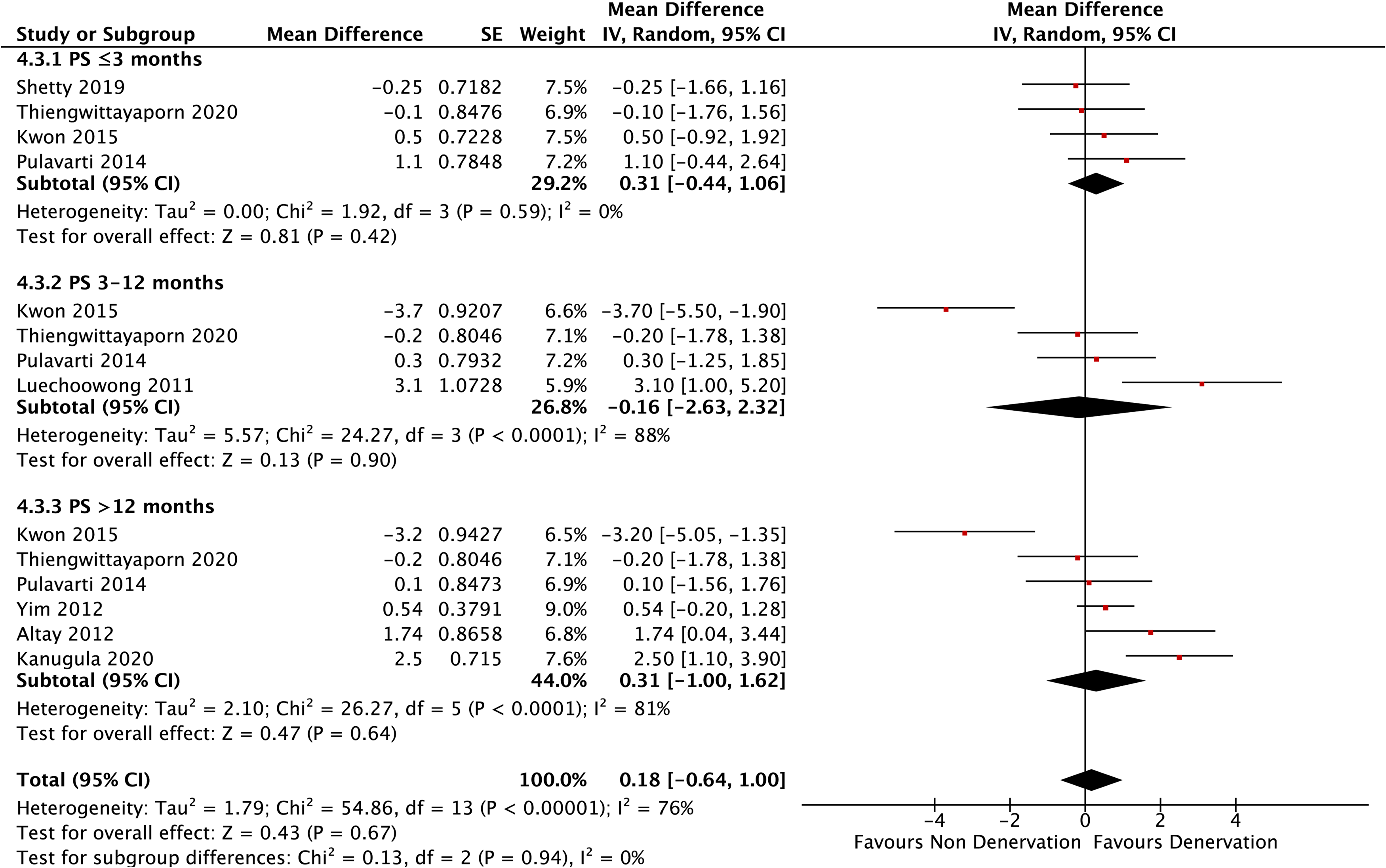
Patellar score.
Knee society score
Twelve studies reported the result of KSS. At any interval of follow-up, KSS did not show any significant differences (p = 0.52 at ≤3 months, p = 0.24 at >3–12 months, and p = 0.10 at >12 months). Meanwhile, the pooled analysis resulted in significantly higher improvement of KSS in PD group (p = 0.03) (Figure 7).
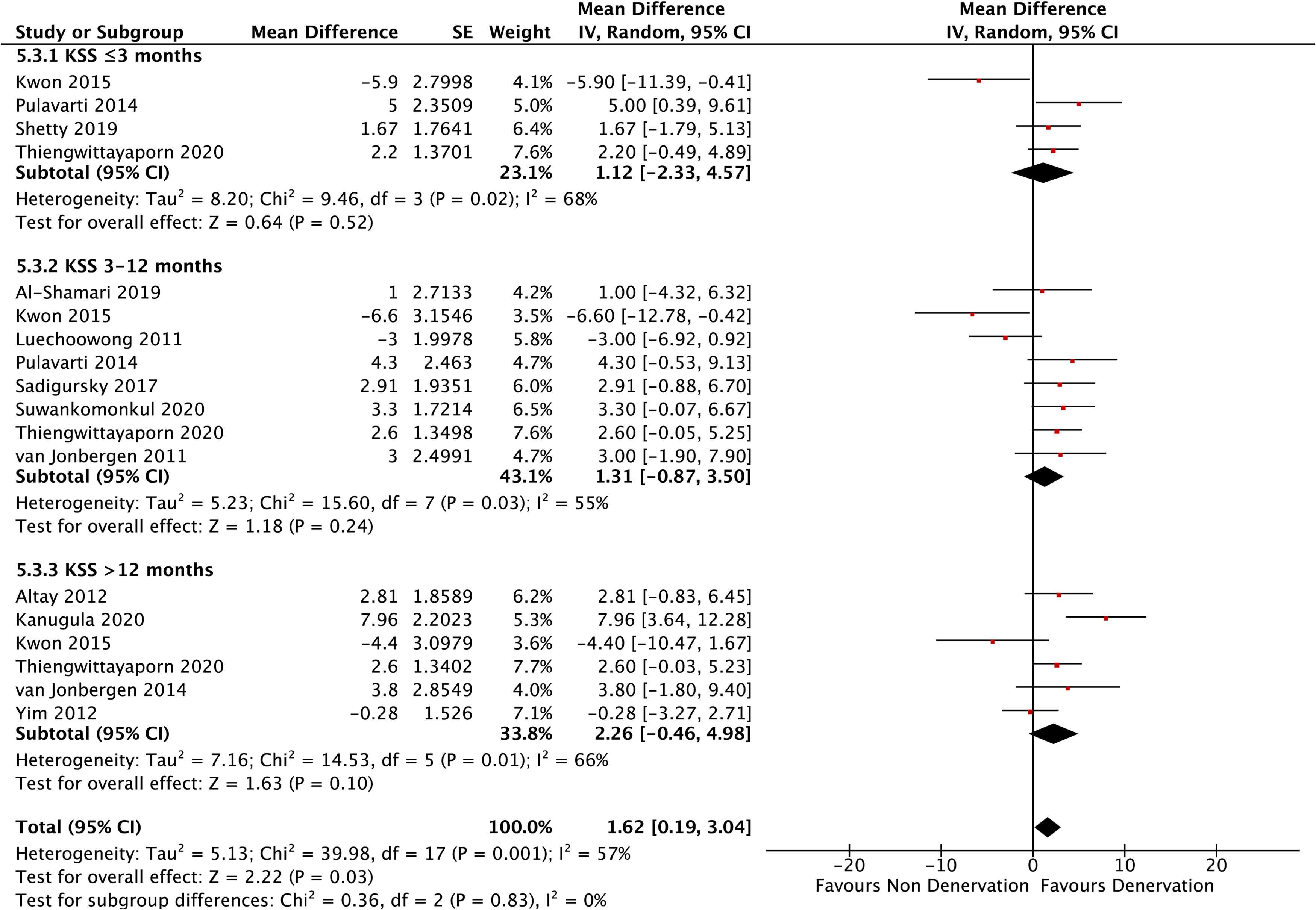
Knee society score.
Knee society score function
As for KSSF, eight studies comprised in the analyses. No significant differences were shown at every follow-up period (p = 0.11 at ≤3 months, p = 0.24 at >3–12 months, and p = 0.97 at >12 months) as well as in pooled analysis (p = 0.19) (Figure 8).
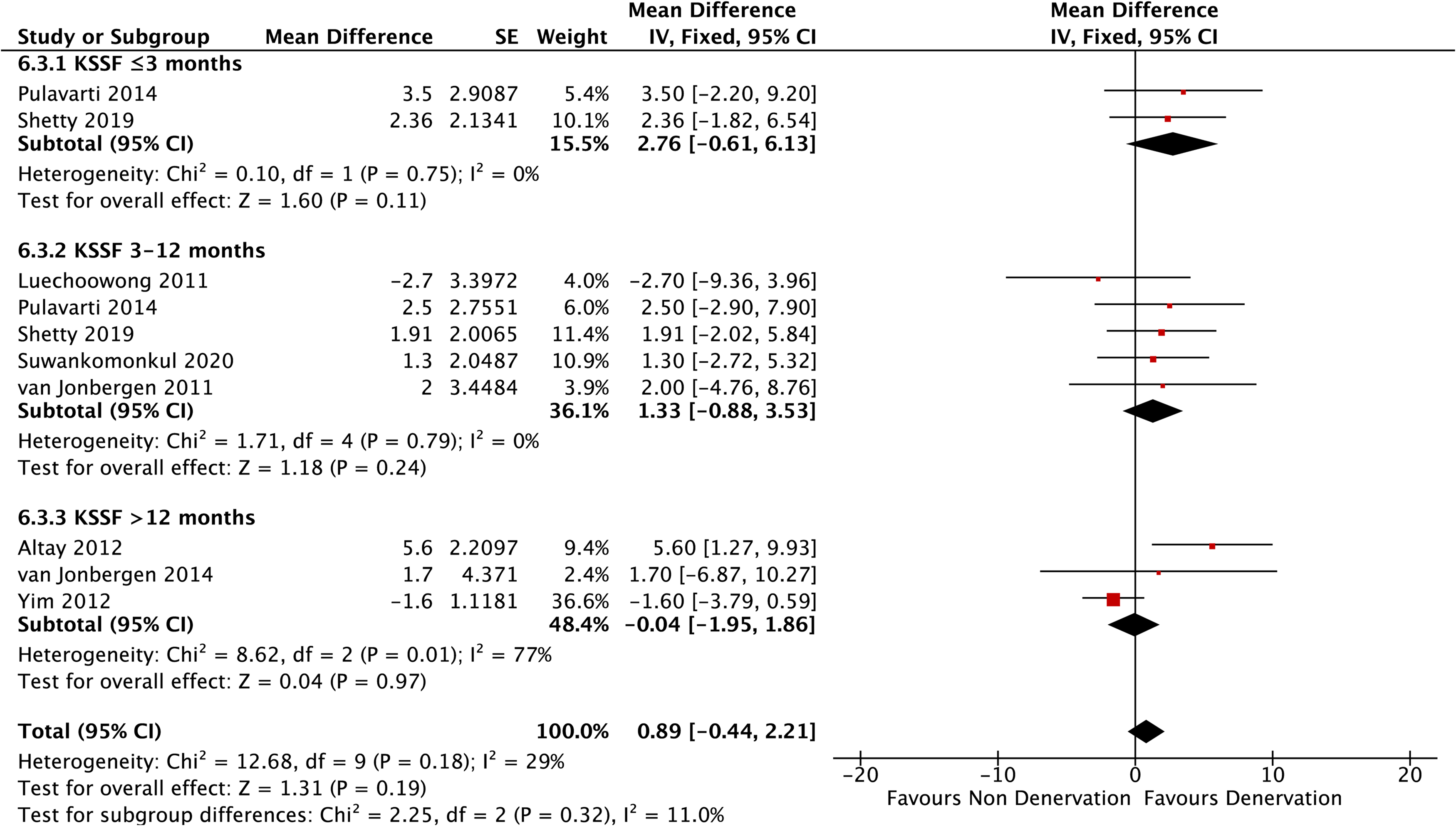
Knee society function subscale.
Complications
Figure 9 presented the comparison of complications between PD and NPD. Eight studies observed no complications throughout the follow-up intervals. The numbers of complication in both groups were equal, 17 events each. Reported cases of complications were as follows: 15 limited ROM that needed manipulation (9 in PD and 6 in NPD), 8 deep vein thrombosis (3 in PD and 5 in NPD), 7 delayed wound healing (3 in PD and 4 in NPD), 3 deep infection (2 in PD and 1 in NPD), and 1 patellar lateralization (0 in PD and 1 in NPD). No significant difference between PD and NPD groups (p = 1.00).
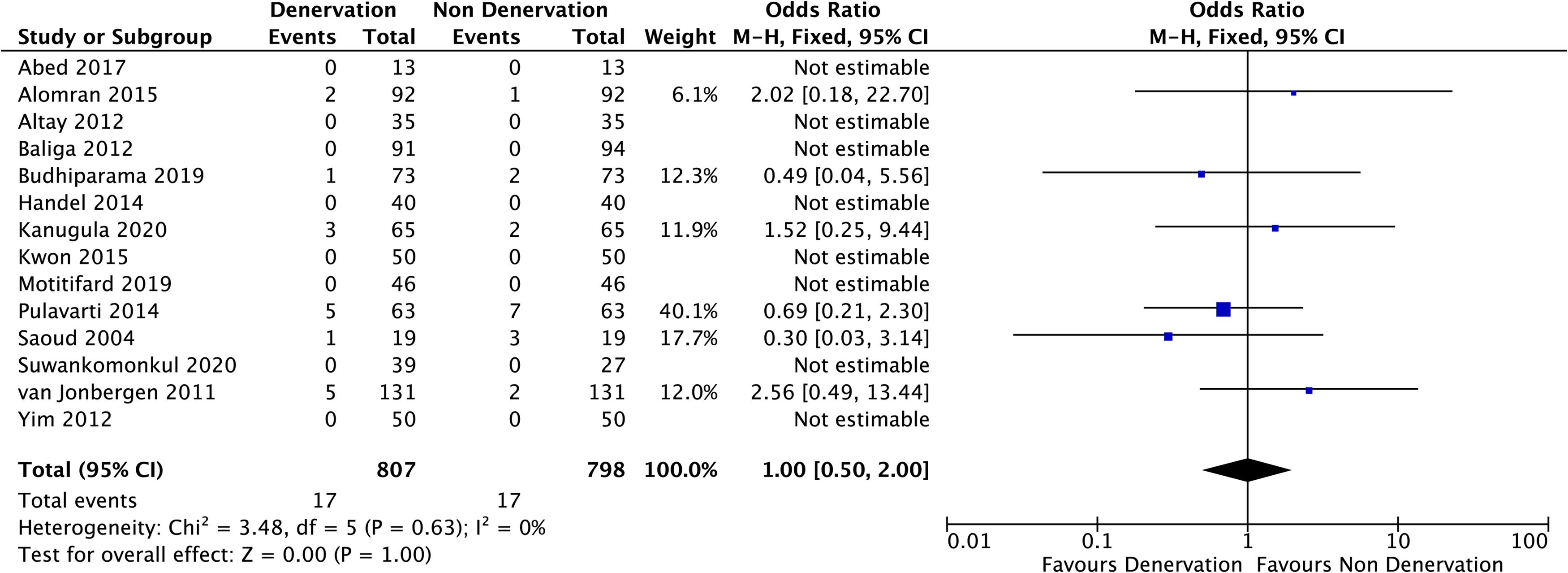
Complications.
Depth of electrocauterization
Comparisons of each parameter according to the depth of electrocauterization were shown in Figure 10. Not all studies reported the depth of diathermy and two studies reported with the value of 1–2 mm therefore were excluded from the analyses. Among 11 studies that recorded incidence of AKP, only four clearly stated the depth of cauterization and all of them were within 1 mm. In addition, incidence of AKP remained favorable in PD group compared to NPD group (p < 0.0001).
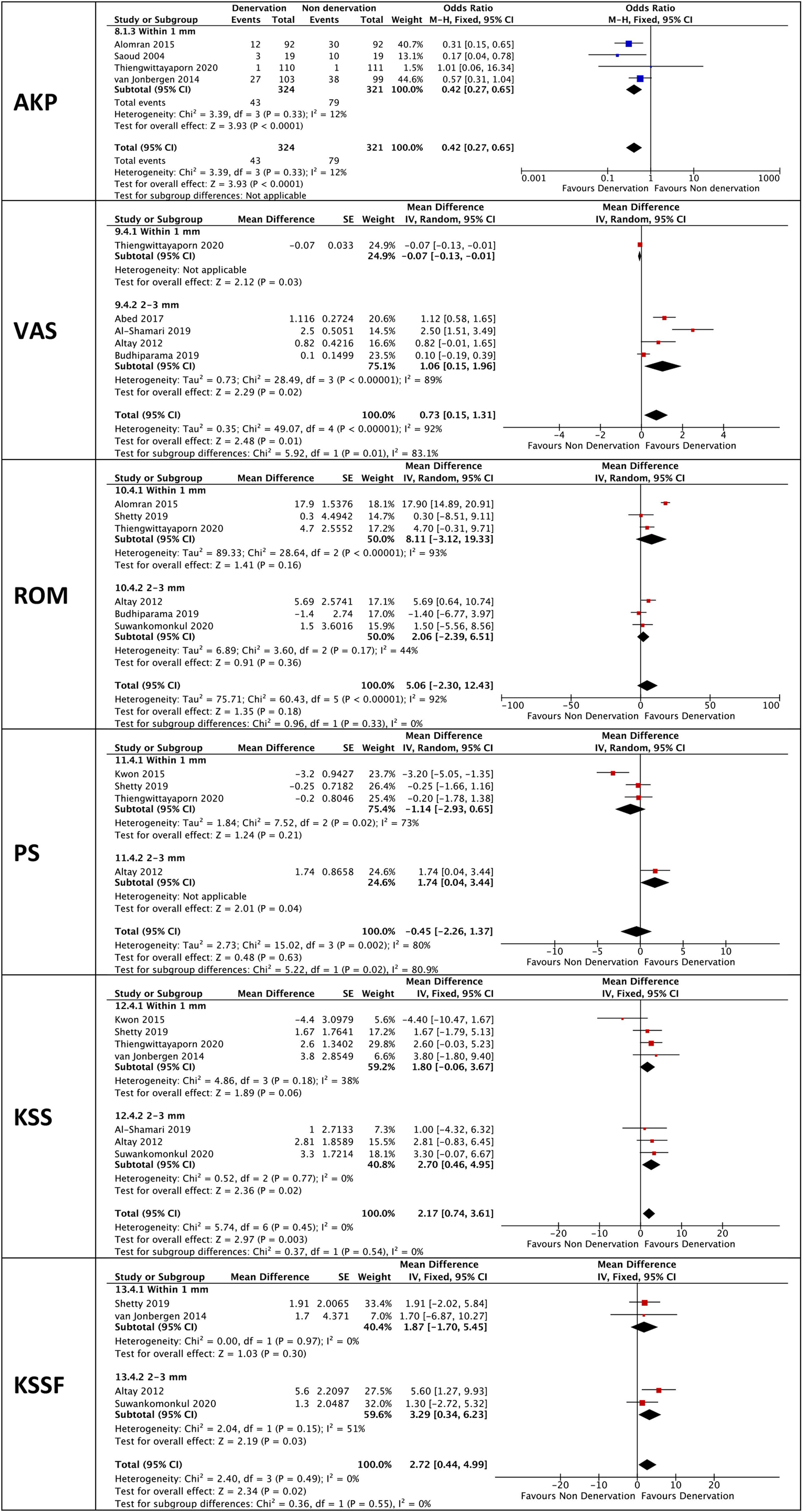
Subanalyses based on depth of cauterization.
Regarding the depth of cauterization, superior outcomes in terms of VAS, PS, KSS, and KSSF were observed in 2–3 mm group, but test for subgroup differences only showed significant results in VAS and PS (p = 0.01, p = 0.02, p = 0.54, p = 0.55, respectively). Both subgroups showed better ROM improvement in PD compared to NPD but without significant differences. Test between subgroups also showed no statistical difference (p = 0.33).
Discussion
Although eliminating knee pain is one of knee arthroplasty goals, pain following this surgery is a frequent complaint. The mechanism of post arthroplasty knee pain is still a mystery. A systematic review has been done to evaluate the possible sources, but failed to point on a single factor as the underlying cause of this problem. 34
PD seems to be a plausible modification and stand a promising chance in overcoming patellofemoral pain after knee replacement. Few meta-analyses have been conducted in the past and produced various results hence conclusion could not be drawn. In this meta-analysis, we included more studies and we compared each numeric variable by the improvement at the time of follow-up from pre-operative values, expecting that these would result in a more reliable information than only comparing the post-operative values.
The procedure of denervation is not an unfamiliar concept and has been implemented for many other pain related disorders. Unlike others, the approach of PD is not a selective neurotomy. Substance-P, a nociceptive afferent nerve fiber, was reported distributed abundantly in the peripatellar soft tissue thus might play an important role in the event of AKP. This raised the premise that thermal injury produced by diathermy in this area might destruct the pain receptors and desensitize the anterior knee region, which consequently alleviate the pain.35–37
We observed that PD had significantly favorable outcomes on: number of AKP (overall and at all time points of follow-up), VAS (overall and ≤3 months), ROM at ≤3 months, and pooled analysis of KSS. This reflected that denervation may help in reducing the incidence of AKP. However, qualitatively, its superiority over NPD was short-term, that is, ≤ 3 months, as expressed in the VAS and ROM. Overall KSS showed better result in denervation, but not in subgroup analyses. This might be due to the diminished power on statistical analysis caused by reduced size effect in subgroups.
These findings differed from the recent meta-analyses conducted by Yuan et al. 38 and Wang et al. 39 Both studies observed significantly lower incidence of AKP in PD group in short-term follow-up (12 months), but the significance was no longer existed after 12 months. This difference might be due to the number of articles included in the studies.
Wang et al. 39 and Yuan et al. 38 found that post-operative VAS was significantly lower in PD group at ≤ 12-month follow-up. Like this study, Fan et al. 40 also evaluate ROM by the change of pre- and post-operative values. They reported better recovery of ROM in PD group but without taking into account the length of follow-up. We broke down the follow-up time frame and found that significant difference of VAS and ROM improvement between two groups was only observed at ≤3 months. Having a similar result in VAS, we assumed that greater ROM improvement might be due to better recovery in pain severity.
This study observed significant increase in overall KSS but not KSSF and PS. Knee society score consists of four subscales: objective and the patient reported subscales, satisfaction, expectation, and functional activity subscales (KSSF). On the other hand, patellar PS evaluates AKP, quadriceps strength, ability to rise from chair, and stair-climbing.
We assumed that the effect of better pain relief during the early period might lead to better patients’ satisfaction. A RCT by Pulavarti et al. 25 found significantly higher satisfaction in PD group compared to NPD group and Rudraraju et al. 41 also recorded better satisfaction in diathermy group in subjects who had patelloplasty with knee arthroplasty in their RCT. The non-significant results in KSSF and PS in this study seemed to confirm the effect of denervation is solely for pain management. This may also be explained by the fact that knee strength or knee function is influenced by many factors other than pain.42–45
Despite claimed to be safer than patellar resurfacing, there are probable adverse events that may be caused by denervation. Gupta et al. 46 suggested that there might be a probability of proprioceptive disturbance after PD that could lead to load bearing derangement. The electrocauterization was also suspected to be able to cause cartilage necrosis, either by direct thermal injury to the cartilage or indirect heat stress to the patellar tendon, which is the entrance of blood vessel, and therefore the interrupted blood supply can eventually lead to osteonecrosis. Nevertheless, this study showed no difference of complications between PD and NPD.19,47
Depth of electrocautery seemed to have an influence on PD. Aside from ROM, better improvement in terms of VAS, PS, KSS, and KSSF were obtained in cauterization with 2–3 mm depth compared to ≤1 mm depth, although significant impact was only observed in VAS and PS. This suggested that the lack of uniformity in denervation technique may play a role in inconsistent results existed in the literature. If PD would be included in future routine practice, we deemed it would be necessary to have this technical matter standardized.
We realized that this study has its own limitations. First, to acquire as much information as possible, we also included non-randomized studies. These non-randomized studies might carry biases that were not clearly stated in the literatures, even though studies showed that the benefits of including these studies would likely to outweigh the drawbacks.48,49 Second, we also included non-English studies that are not our native language and therefore might also cause language-related bias.
Conclusion
The role of circumpatellar denervation in knee arthroplasty is still in a gray area. Although some authors found no significant advantages of denervation in knee arthroplasty, we inferred that beside reducing the number of AKP incidence, denervation may still offer some benefits. We also believed that shorter length of pain recovery and being able to gain better movement faster may impact patients’ satisfaction. As denervation did not have more complications than non-denervation, therefore, we proposed that denervation is a safe technique that can be considered in the practice of knee arthroplasty, especially if its effects will be in the interest of the patient. Furthermore, cauterization with depth of 2–3 mm may have better outcomes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.