
Abstract
Introduction
Although better surgical exposure is encountered with the excision of infrapatellar pad of fat (IPPF) during total knee replacement (TKR), some studies showed an increase in anterior knee pain and other specific complications associated with such a step. The purpose of this study was to add in literature a new comparison between IPPF excision and preservation during TKR, focusing on the anterior knee pain, functional range, oxford knee score and patellar height through a randomized clinical trial
Methods
This prospective randomized study was conducted from 2016 to 2019 on 90 patients with knee osteoarthritis treated with elective primary TKA by same surgeons at one hospital with the same implant design with a mean follow up of 18 month. Patients were randomized into two groups: one group including patients with IPPF complete excision and the other group include patients with IPPF preservation. No patella resurfacing was done. Pre and postoperative anterior knee pain was recorded and compared using VAS score in addition to Oxford knee score.
Results
At 6 months follow-up, 10 knees and 14 knees (27%) had anterior aching discomfort with a mean postoperative extension were −5.3 and −5.2 in IPPF preservation and excision group patients, respectively. There was no statistically significant differences between both groups regarding anterior knee pain, range of motion, oxford knee score or patellar height measurement through the follow up period. No patellar complications were recorded in all cases.
Conclusion
Although Infrapatellar fat pad excision in TKA resulted in a minor increase in number of patients with postoperative anterior knee pain, it was of no statistically significant difference. Hence, whenever a better surgical exposure is needed, IPPF excision should be considered. Additional large scale randomized studies should be added to the calling literature for more result validation and guidelines formulation.
Introduction
The functional results after total knee arthroplasty (TKA) is a multifactorial subject that need to be addressed individually. Starting from patient education to the rehabilitation program, all these factors must be optimized. One of the important steps during the surgical technique is dealing with infrapatellar pad of fat (IPFP) whether to resect or to preserve.1,2
Infrapatellar fat pad is mass of adipose tissue two-faced between the patellar ligament, the lower end of the patellar and proximal tibia. Anatomically, it is considered an intraarticular extra synovial compartment that might support effective joint lubrication.3
The IPFP containing nerve fibers that might play an important role in pain sensation and contribute to the inflammatory processes in anterior knee pain. In addition some studies suggest a significant role for the IPFP in the blood supply of the patella and the anterior part of the knee.4
Although removal of the fat pad is not uncommon in TKA owing to the gained favorable effect (enhancing surgical exposure, tibia bone cut, polyethylene implantation), it may be associated with some adverse effects (Scarring of the infrapatellar tendon, patella baja, range of motion reduction, stiffness and persistent anterior knee pain).5–7 The sufficient operative exposure tends to motivate a lot of surgeons to remove it during surgery as there is a debate regarding the effect of its resection with no complete agreement.5,6
This choice remains debatable, and practice forms differ extensively. The literature data contain only two meta-analysis that tried to grasp evidenced based decision criteria.7
Although biomechanical data embrace this argument, the clinical impact of the fat pad removal has not been obviously recognized up till now.8
The aim of this study is to investigate and compare resection versus preservation of the infrapatellar pad of fat during total knee arthroplasty regarding anterior knee pain, oxford knee score, range of motion, functional outcome and patellar height.
Materials and methods
Patient recruitment
This prospective randomized controlled study was conducted in our university and insurance hospital between April 2016 and April 2019 including patients with primary knee osteoarthritis [OA] (50 years old or older) treated with elective primary TKA after the approval of the scientific board and the ethical committee of our department (IRB approval #MS-622-2016). Patients with secondary cause for osteoarthritis (rheumatoid arthritis, posttraumatic), history of previous knee surgery, severe varus or valgus (more than 15 degrees) or fixed flexion deformity (more than 15 degrees) were excluded from this study.
The study sample size was calculated based on expecting a mean difference in the knee range of motion (flexion / extension) equal to 25 degree between the two-study groups after TKR. Assuming a standard deviation of 5 degree, an alpha error of 0.05, and 90% statistical power, 40 patients were required in each group. To compensate for the dropout, 90 patient were enrolled.
Randomization
The patients in this single-blinded study were allocated randomly into one of two groups; the first group included replacement with complete excision of IPFP and second group included replacement with preservation of IPFP. The randomization agenda was engendered earlier to the launch of enrollment for the study and was done using sealed opaque. The randomization list provided to the author who was not blinded to the patients’ groups and the patient was blinded to the randomization pool. The patients in this single-blinded study were allocated randomly into one of two groups; the first group included replacement with complete excision of IPFP and second group included replacement with preservation of IPFP. The randomization agenda was engendered earlier to the launch of enrollment for the study and was done using sealed opaque. The randomization list provided to the author who was not blinded to the patients’ groups and the patient was blinded to the randomization pool.
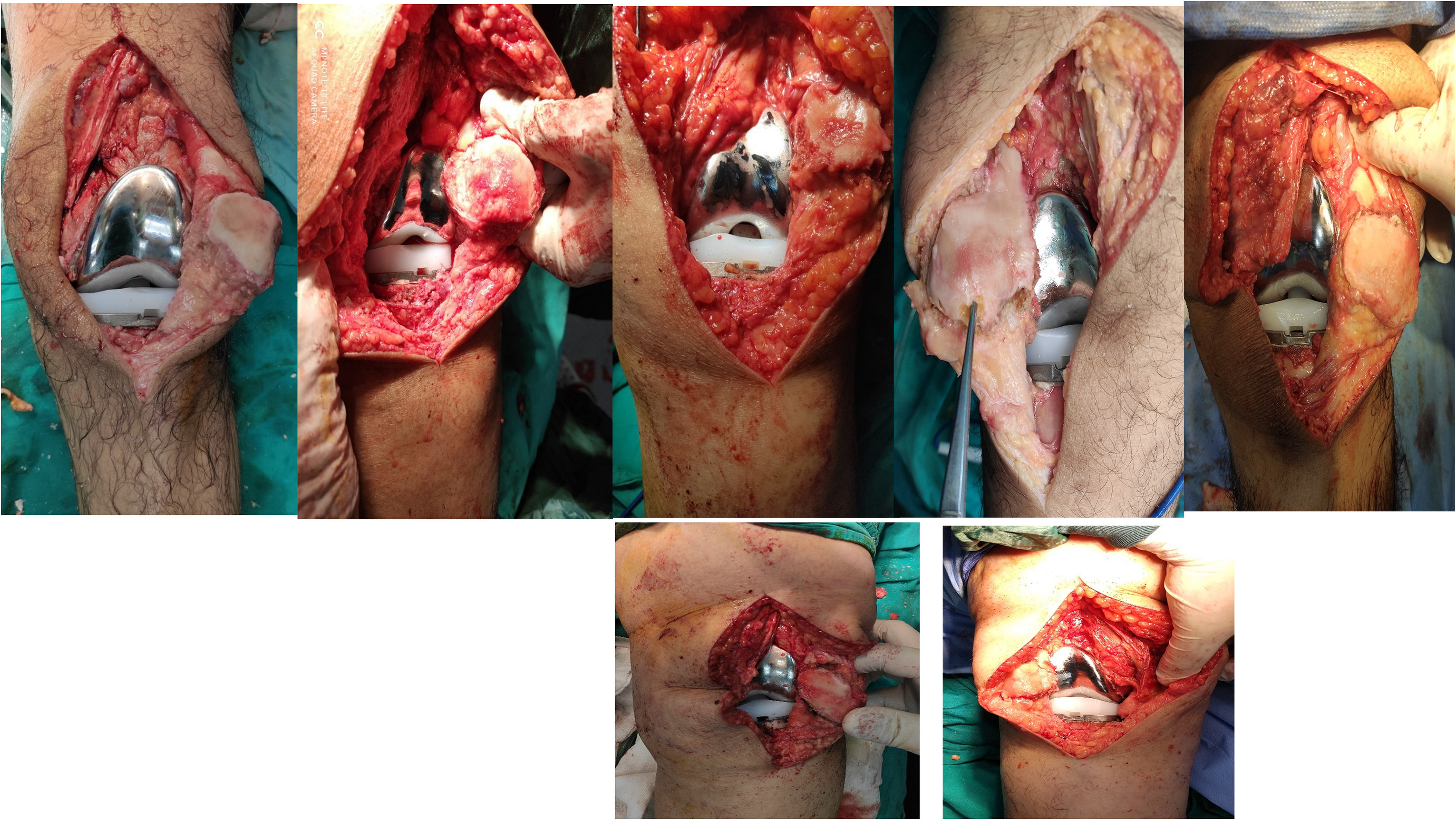
Patients with complete excision of infrapatellar pad of fat.
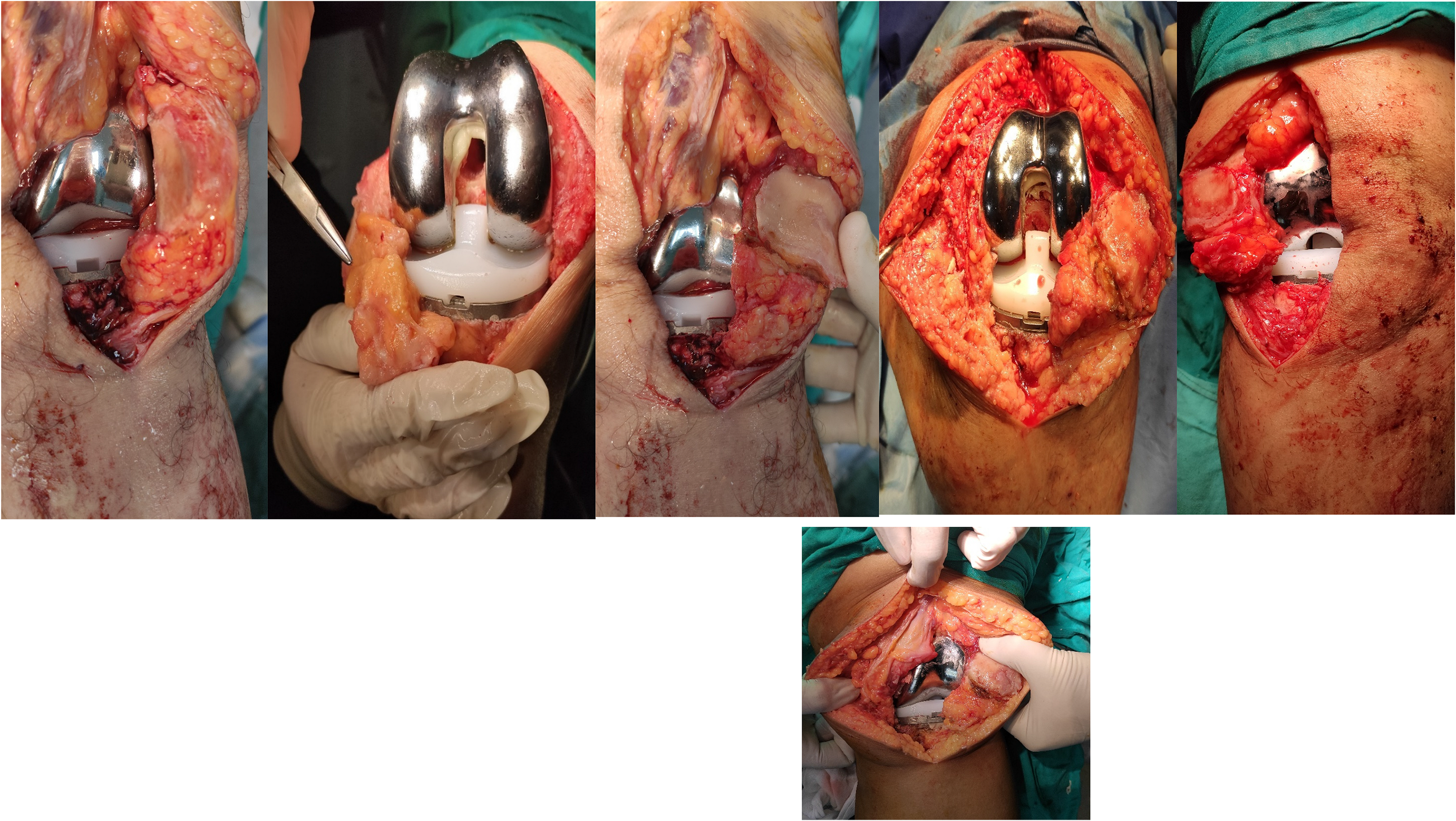
Patients with preservation of infrapatellar pad of fat.
Surgical technique: The authors did all arthroplasties under spinal anesthesia using the medial Para patellar approach with patellar eversion in all cases while the patient was in the supine position and using the standard gap balancing technique in femur/tibia preparation. In the fat pad removal group, all the fatty tissue was removed completely from the under surface of the patellar tendon after patellar eversion (Figure 1). In the fat pad preservation group, the whole fatty tissue is preserved and retracted away from the surgical field by a double–angled homman applied carefully to the edge of the lateral tibial plateau through the whole surgery (Figure 2). All the primary cemented arthroplasty implants were provided from one company with the same implant design (posterior stabilized PS design with no ultracongruent inlays). No patellar resurfacing was done for all patients. Standard Postoperative care program was conducted to all cases highlighting the rehabilitation therapy starting from the first postoperative day. Radiological and functional assessment was done every 3 month at the outpatient clinic.
Outcome measurement: Definition of anterior knee pain in our study was anterior aching distress while ascending or descending stairs in addition to any distressing kneeling pain at the anterior part of the knee with flexing or extending that disturbs daily life activity and was graded according to VAS score. In addition, Functional evaluation was done using oxford knee score [3] every 3 month until the final follow up visit, recording the outcome improvement with a mean follow up 18 month (range:16-22 month). Patellar height was measured and recorded using both Insall-Salvati ratio and The Caton-Deschamps index on the lateral radiograph of fixed magnification with about 30º knee flexion (Figure 3). Other complications as recurrent effusion, patellar fracture and malt racking in addition to wound complication was assessed at the same follow up visit.
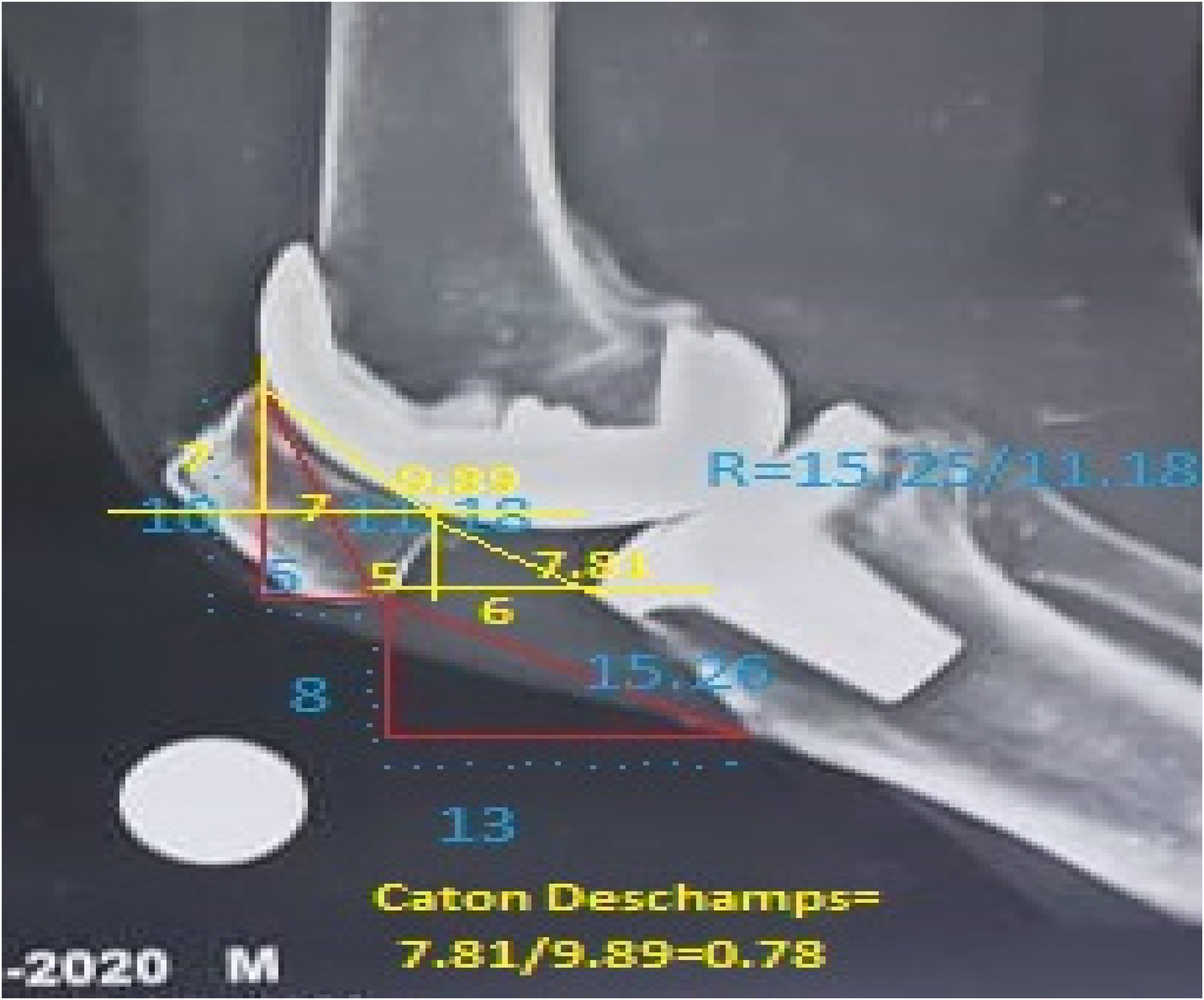
Patellar height measurement using Insall-Salvati ratio and the Caton-Deschamps index.
Statistical analysis
Information was entered using Statistical Package for the Social Sciences version 23 and concise using mean and standard deviation. Assessments between quantitative variables were completed by means of the non-parametric Kruskal-Wallis and Mann-Whitney tests while for evaluation of serial measurements the non-parametric Friedman test and Wilcoxon signed rank test were utilized. For matching categorical data, Chi square test was accomplished. Associations among quantitative variables were finished by Spearman correlation coefficient. Values fewer than 0.05 were reflected as statistically substantial.
Results
120 patients listed for primary total knee arthroplasty were selected for participation in our study. 24 were ineligible based on our exclusion criteria and were excluded, while eight refused to participate.
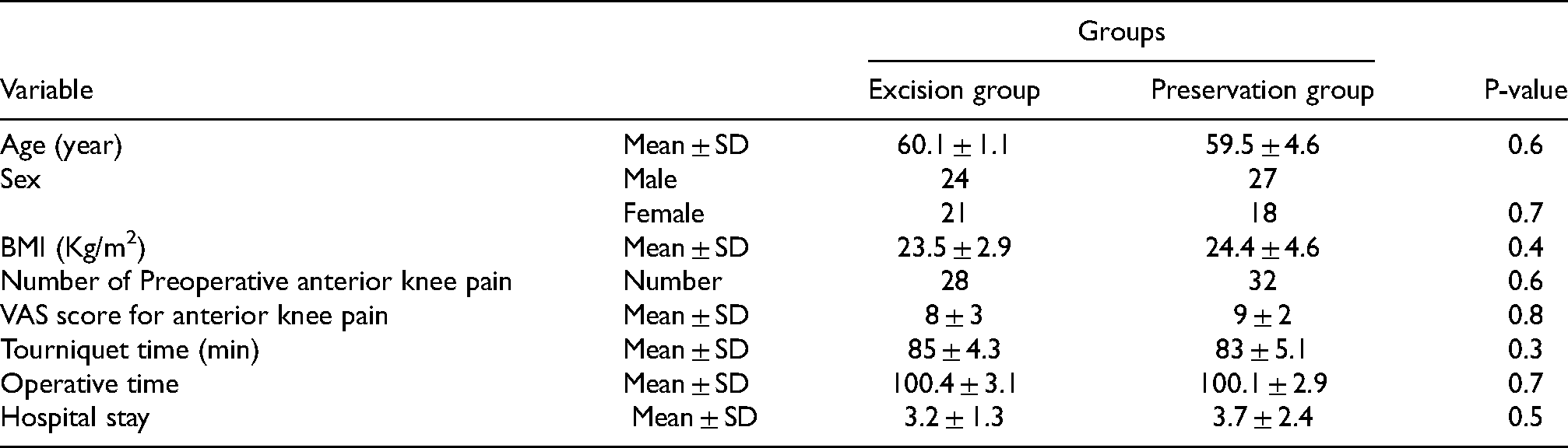
There were no statistically substantial variances between the two groups concerning demographic data, perioperative surgical characteristics, preoperative flexion, preoperative oxford knee score, or preoperative laboratory values. Preoperative anterior knee aching or discomfort was graded using VAS score in the two groups, with no statistically difference value (Table 1).
Patient demographics and characteristics in both groups.
In general, Excision of the fat pad was linked with superior postoperative anterior discomfort. Of the knees that underwent fat pad removal, 68.8% [31] were graded as painless knees compared to 77.7% [35] of the knees with preserved pad. At 6 months follow-up, 10 knees and 14 knees (27%) had anterior knee pain in IPFP preservation and excision group patients, respectively. This pain decreased through the follow up period until the final visit where the number of cases with anterior knee pain was nearly equal. This difference was not significantly difference (Table 2). The mean VAS pain scores in both groups were comparable through the recorded follow up period and this difference was not statistically significant (Table 3).
Anterior knee pain distribution in both groups through the follow up period.

VAS score measurement for anterior knee pain quantification in both groups through the follow up period.

The mean degrees of postoperative extension were −5.2 ± 3.7 in the IPFP excision group versus −5.3 ± 2.6 in the preserved IP groups at 6 month follow up, with gradual improvement through the follow up period in both groups; however the difference between both groups was not statistically significant (Table 4).
Range of motion (extension angle) in both groups through the follow up period.

Regarding the flexion range, at the first follow up visit the mean postoperative flexion was 100.9 ± 11.5 in the excision group IPS group versus 105.7 ± 13.4 in the non-IPS group, with no statistically significant difference at the final follow up visit (Table 5).
Range of motion (flexion angle) in both groups through the follow up period.

Oxford Knee Scores did not vary statistically between patients whose fat pad was excised and patients whose fat pad was preserved (Table 6).
Oxford knee score recording in both groups through the follow up period.

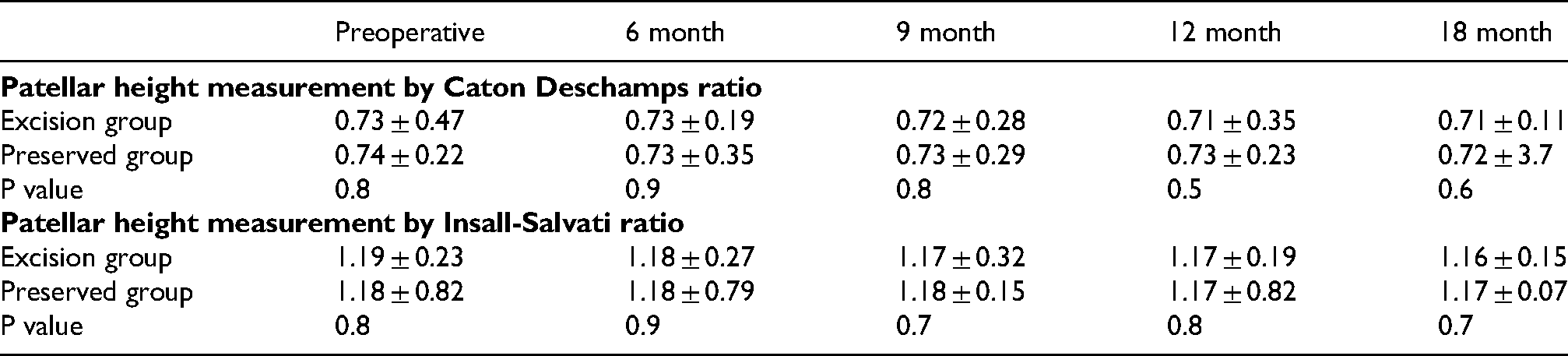
There was no statistical significant difference in the measurement of patellar height between the two groups. The serial lateral radiographs through the follow up period did not display any significant variation in the mean Insall-Salvati ratio and the Caton-Deschamps index in either group (Table 7).
Patellar height measurement in both groups through the follow up period
No knee effusion or complications related to patella (patellar fracture, maltracking or wound complications) was recorded in both groups at the last follow up visit.
Discussion
Generally, in the presented literature there is absence of solid evidence towards benefits of preservation or resection of the infra-patellar fat pad during total knee arthroplasty. There are currently no guidelines regarding this issue with debatable material concerning removal of the fat pad that may cause patellar-related complications after TKA, which should be cautiously balanced with the benefit of the improved surgical exposure.
The present study compares the effects either preservation or the resection of the infrapatellar pad of fat during total knee replacement with no significant differences recorded between the two technique groups regarding anterior knee pain, functional outcome, oxford knee score and patellar related complications. We tried to reach an effective cost benefit technique with the least drawback outcome on the functional result.
Although we have replicated the findings in some studies, the literature still call for more high quality randomized, controlled trial over a longer period comparing both techniques in elective knee arthroplasty to confirm this finding.
Numerous trials display a synchronization in their outcomes where the shared feature was an increase in the incidence of anterior knee pain with IPFP resection compared to preservation after long follow up period.
White et al. conducted a systematic review revealed an increased incidence of anterior knee pain with IPFP resection beyond six-months post-operatively.10 Pinsornsak et al. conclude that the patients in excision group had more anterior aching on the short follow up visits compared with preservation group.11 Retrospective study conducted by Meneghini et al.12 showed that the anterior knee pain has been doubled at the final follow up in the excision group patients compared to the reserved (mean follow-up of 5.1 years).12 Comparable conclusions was released Moreland et al.13 and Tanaka et al.14 reported that infrapatellar fat pad excision in rheumatoid patients had more anterior pain at the last follow up. Baker et al. reported in another retrospective study there is no variance in satisfaction for both resection and preservation.15
However, a recent systematic review done by Van Beeck et al. found contradictory results with conflicting evidence where he found no difference in anterior knee pain, ROM, or function in the patient with osteoarthritis.16
The limitation of the current study include the single blindness investigation, the small sample size allocated in addition to the subjective nature for the anterior knee pain that has difficult analysis with complicated interpretation. Oxford knee score also may be not be very specific to the anterior knee pain. For that reason, a single surgeon perform all surgeries on osteoarthritic cases only with the same implant with no patellar resurfacing in a trial to decrease these confounding variables. Any degree of anterior knee pain was recorded through the VAS score.
Future large scale randomized multicenter studies on this topic should be conducted to validate these results and provide certified guidelines in the literature.
Conclusion
Resection of infrapatellar pad of fat versus its preservation during TKA is still a debatable area with no strong agreement in the literature with a variable effect on the clinical result. Nowadays, no evidence based guidelines found on the resection of the IPFP during TKA surgery. In the current study, the difference of the postoperative anterior knee pain, range of motion, oxford knee score and the clinical outcomes whether infrapatellar fat pad was excised or not were statistically insignificant. Therefore, we suggest that surgeons had better to save the fat pad if conventional exposure can be reached; otherwise, resection is preferred to improve exposure. However, there is insufficient proof to authorize surgical practice changes concerning the role of the IPFP.
It is important to promote further investigations and well-randomized controlled trials using the similar measurement structure to settle these conclusions and discovering the IPFP resection consequences. This may elaborate further details on this essential subject and formulate a background for basic management guidelines.
Footnotes
Authors’ contributions
both authors contributed in the study conduction, analysis and manuscript formulation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study has been approved by the appropriate ethics committee (the Scientific Board of the Department of Trauma & Orthopaedic Surgery, Cairo University Hospitals). Details that might disclose the identity of the subjects in the study have been omitted.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent for publication
applicable.