
Abstract
Purpose:
The treatment for young patients with advanced knee arthritis by Oxford unicompartmental knee arthroplasty (Oxford-UKA) is still controversial. A relative few studies were published about Asian patients. We evaluated midterm results of Oxford-UKA in young patients aged less than or equal to 60 years.
Methods:
Between December 2009 and December 2018, 95 patients (109 knees) (mean age 57.48 years; range: 33–60 years) were included. The mean follow-up period was 3.0 years (range: 1.0–9.5 years). The functional outcomes and pain score of the knee before and after surgery were examined.
Results:
To the last follow-up, no patient died, six patients (nine knees) were lost and one patient underwent total knee revision in case of unexplained postoperative pain. The patients demonstrated significant improvement in range of knee motion (103.65 vs. 115.96, p < 0.05), Oxford Knee Score (40.0 vs. 14.4, p < 0.05), Hospital for Special Surgery Score (56.0 vs. 85.7, p < 0.05), and Visual Analogue Score (VAS) (5.23 vs. 1.08, p < 0.05) before and after surgery.
Conclusion:
Our midterm results showed that the Oxford-UKA was a reliable and effective treatment option for young patients aged less than or equal to 60 years with anterior medial osteoarthritis. The knee pain can be effectively relieved and excellent functional activities of the knee joint can be obtained after surgery.
Introduction
Unicompartmental knee arthroplasty (UKA) was widely performed for the treatment of isolated compartmental osteoarthritis (OA) of the knee. A number of studies showed satisfactory clinical results, with a 10-year survival rate of 94% in Korean patients 1 and 95% in Japanese patients. 2 However, UKA in active young patients is still controversial due to concern regarding higher risk of revision. 3 –5
In addition to UKA, current treatment options for advanced OA include high tibial osteotomy (HTO) 6,7 and total knee arthroplasty (TKA). 8 The follow-up results of TKA demonstrated that the overall risk of complications was higher for patients undergoing TKA than UKA (11% vs. 4.3%). 9 What’s more, it was reported that TKA has a less successful outcome in younger patients than in elderly patients. 10 For HTO, the survivorship is reported approximately 70–80% by 10 years followed up. 11 –13 UKA’s less invasive approach has many theoretical advantages over TKA and HTO, which are the greater preservation of bone, a more rapid recovery, and a lower risk of infection and morbidity. 9,14,15 Thus, UKA is considered as a procedure with satisfactory medium- and long-terms results. 16 Even so, the performance of UKA in young patients has not been completely consistent. 4,17 –19 The study from Parratte et al., proposed that polyethylene wear is one of the most important contributors affecting the survival of UKA in young patients. 20 With the development of surgical techniques and prosthetic designs, a number of studies have been published on the good medium- and long-term outcomes of UKA in young patients. 21 –23 Although the efficacy of UKA in patients over 60 years of age is definite and the survival rate is satisfactory, there are still different reports on the efficacy of young patients. In particular, a relatively small number of studies have been published on the Asian population.
In this study, we evaluated the midterm results of young Asian patients (≤60 years) who underwent Oxford-UKA with the cemented meniscal-bearing prosthesis. This study aimed to determine whether the Oxford-UKA can be reliable and safe in young Asian patients according to the assessment of clinical outcomes and complications.
Materials and methods
Patient characteristics
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee (Yangpu Hospital, Tongji University). Patients’ informed consent was also obtained.
Since December 2009, 101 patients (118 knees) were enrolled. None died, six patients (nine knees) were lost to follow-up. The remaining 95 patients (109 knees) were followed up for 3.0 years (range: 1.0–9.5 years). All operations were performed by one senior joint surgeon. The details can be seen in Table 1. All patients satisfied the recommended indications as described by Goodfellow et al. 24 including anteromedial OA with functionally intact of the medial collateral ligament (MCL) and anterior cruciate ligaments; there was full-thickness cartilage in the lateral compartment; correctable varus deformation less than 15°. The weight, level of activity, and degeneration of the patellofemoral joint (PFJ) were not considered as contraindications.
Demographic data for study population.

Surgical technique and postoperative management
All surgeries were performed by the same senior surgeon with the Oxford phase Ⅲ (Biomet, Warsaw, Indiana, USA) prosthesis. The operation was performed through a minimally invasive, medial parapatellar incision (about 8–10 cm long). The tibial saw guide is aligned with the long axis of the tibia and fixed on the extramedullary rod. A reciprocating saw was used to make the horizontal osteotomy and vertical cut. Then, we insert the intramedullary guide into the drill hole located in the anterior to the anteromedial aspect of the intercondylar notch. Next, we place the second femoral drill guide parallel to the intramedullary guide in the anteroposterior and lateral planes. The posterior facet of the femoral condyle was resected using a femoral saw block, using the ligament balancing technique and a spherical cutter to require a number of spigots, the femoral condyle was milled. The prostheses were cemented when a test was satisfactory. Details of the operative technique are described in the operation manual of Oxford phase Ⅲ-UKA. 24,25 Taking care of ligament accurate balance and the bearing did not impinge on cement or retained bone. Wound drains were not applied in both groups. Perioperative intravenous antibiotics were given for 24 h. Thromboprophylaxis was routinely prescribed consisted of low-molecular-weight heparin administered subcutaneously or rivaroxaban was given orally day after surgery and was continued for at least 4 weeks postoperatively. The patient began to receive fully tolerated physiotherapy gradually after surgery.
Clinical evaluation
Clinical assessment was performed preoperative, 3, 6, and 12 months and thereafter once a year after surgery. The assessment using the range of knee motion (ROM), Oxford Knee Score (OKS), Hospital for Special Surgery Score (HSS), and visual analogue scale (VAS) scores for pain. The VAS is a 10-cm long line, where patients indicated the degree of pain, being informed that the 0 points refer to no pain and the 10 points mean most severe pain. 26 Complications such as intraoperative patellar ligament injury, patellar snapping or impingement, wound problems, deep venous thrombosis, pulmonary embolus, knee stiffness, progressed arthritis of medial compartment, implant loosening with or without polyethylene wear, and mechanical failure requiring revision were recorded.
Statistical analysis
The statistical analysis performed with SPSS 20.0 (Statistical Package for Social Sciences, IBM, USA) software. The difference between the mean preoperative and postoperative was analyzed by the paired student’s t-test. The data are presented as mean ± standard deviation. The differences were considered significant at p < 0.05.
Results
Clinical Outcome
The primary indication in 109 knees was medial compartment OA; one knee was treated for traumatic OA. By the end of the last follow-up, a total of 95 young patients who met the inclusion criteria and received medial Oxford-UKA were followed up. The average follow-up time was 3.0 years (range: 1.0–9.5 years), and average age was 57.48 years (range: 33–60 years). Detailed information are presented in Table 1.
By the last follow-up, the mean of OKS decreased from 40.0 (range: 35–59) preoperative to 14.4 (range: 12–29) postoperative (p = 0.00); the HSS increased from 56.0 (range: 42–67) preoperative to 85.8 (60–93) postoperative (p = 0.00). The mean of VAS decreased from 5.23 (range: 4.0–6.0) preoperative to 1.08 (range: 0–4.0) postoperative (p = 0.00); the mean ROM increased from 103.65 (range: 80–130) preoperative to 115.96 (range: 88–125) postoperative (p = 0.00) in Table 2 and Figure 1. All scores showed a significant improvement (p < 0.01). No case to be found with radiographic evidence of pathological radiolucency around the femoral/tibial component or osteolysis. A typical case is from a 44-year-old man presented excellent postoperative results (Figure 2)
Outcome scores, OKS (39.78 vs. 14.38), HSS (55.54 vs. 85.79), ROM (103.65 vs. 115.96), and VAS (5.23 vs. 1.08).a

ROM: range of knee motion; OKS: Oxford Knee Score; HSS: Hospital for Special Surgery Score; VAS: Visual Analogue Score.
a Measurement data are expressed as mean ± standard deviation.
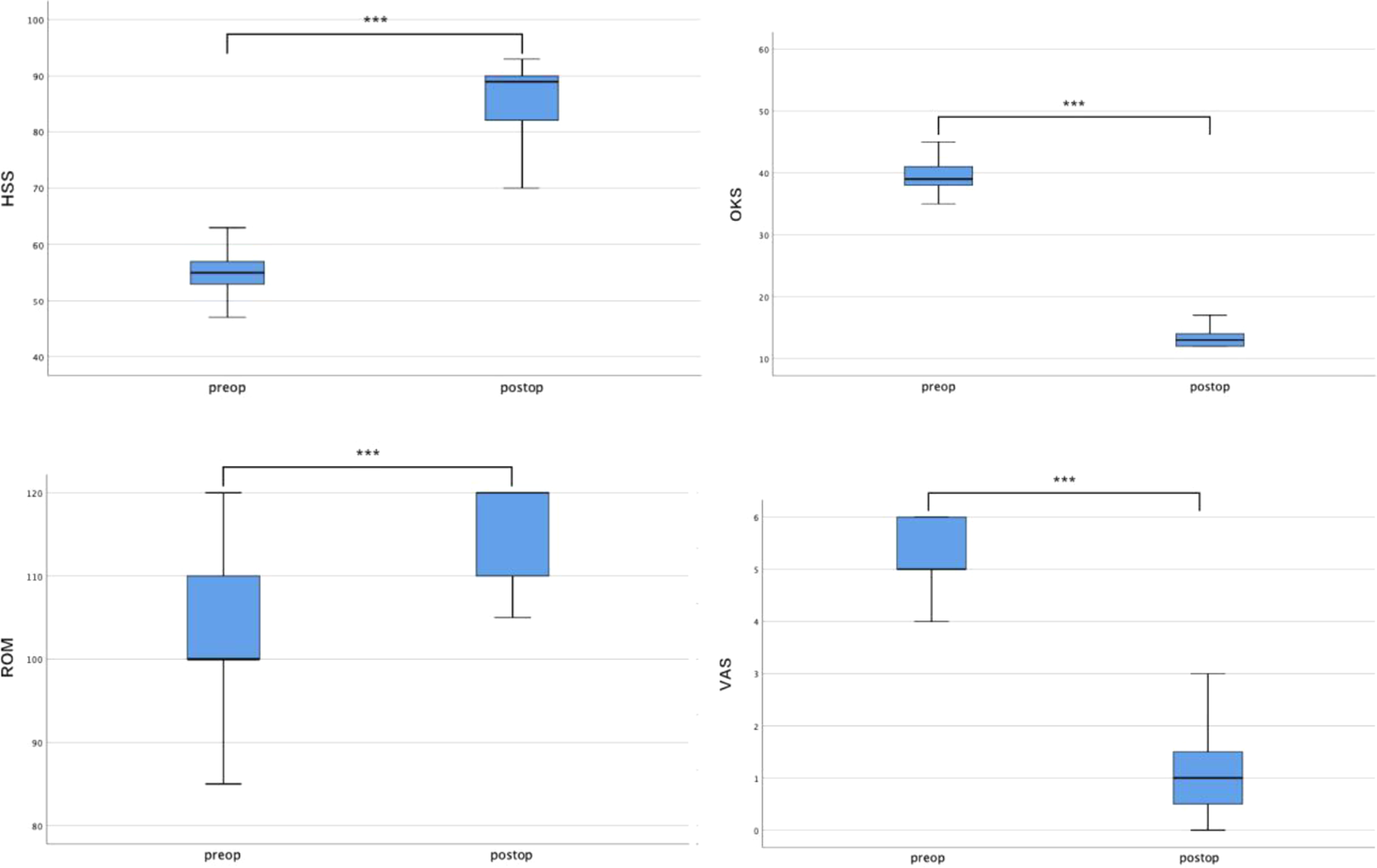
Box and whisker plots showing the outcome scores, HSS, OKS, ROM, and VAS for preoperatively (preop) and at final follow-up (postop). ***p < 0.01. HSS: Hospital for Special Surgery Score; OKS: Oxford Knee Score; ROM: range of knee motion; VAS: Visual Analogue Score.
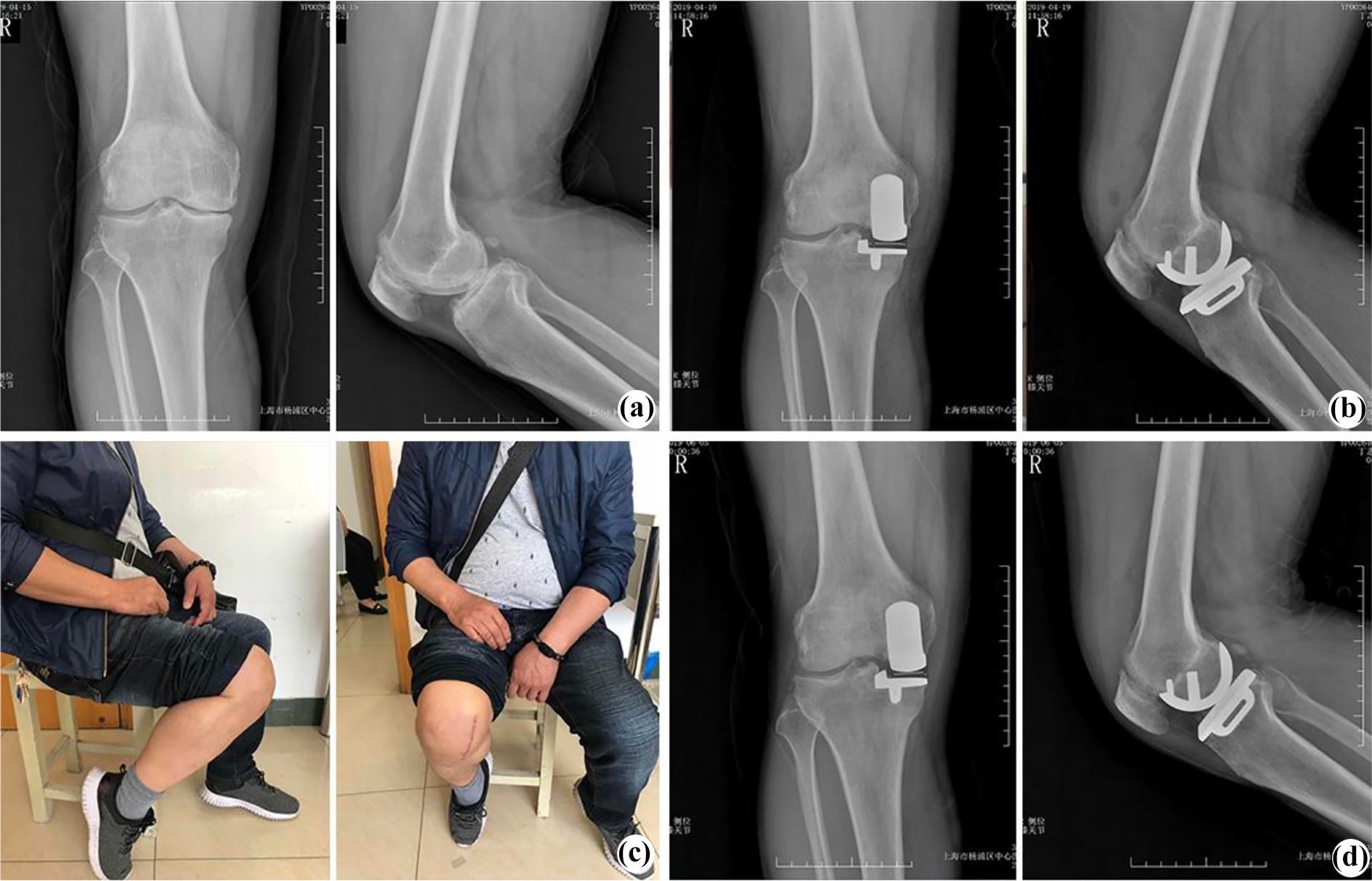
(a) The preoperative radiographs from a 44-year-old man showed that the right side of the knee with medial compartmental OA. (b) The postoperative radiographs after Oxford-UKA with the Oxford phase Ⅲ (Biomet, Warsaw, Indiana, USA). (c) and (d) The imaging and radiographs after surgery for 2 months. OA: osteoarthritis.
Complication
Only one case was treated with TKA because of unexplained pain. Revision knee arthroplasty (Vanguard, Zimmer Biomet, Warsaw, Indiana, USA) was performed 3.0 years after surgery. The unexplained pain was effectively relieved after TKA. Other possible complications of UKA including infection, periprosthetic fracture, MCL injury, and lateral compartment progressive OA were not observed.
Discussion
We followed 109 knees in 95 young Asian patients (≤60 years) after Oxford-UKA for an average of 3.0 (range: 1.0–9.5) years. Our results of the study indicated that medial Oxford-UKA is safe and reliable for the treatment of patients with anterior medial osteoarthritis (AMOA) aged less than or equal to 60 years. Our finding is not in agreement with Kozinn and Scott 27 who suggested that the young (<60 years) and active patients were considered as a contraindication of Oxford-UKA. There is still controversy about the Oxford-UKA that is appropriate for young and active patients. The report from Thompson et al. 28 and Pandit et al. 29 was consistent with our result. They suggested that the contraindication about young patients should be amended. Compared with elderly patients, young patients have special characteristics in social life, including longer prosthesis life and the higher requirement for postoperative knee joint function. A report showed that young people use their knees frequently and have about five times as much daily activity as older people. 30
The current treatment of young patients with symptomatic AMOA is still a challenge. Surgical options for young patients with advanced OA include TKA, HTO, and UKA. Traditionally, HTO has been considered as an effective surgical method for the treatment of young patients with OA and able to return to the higher level of function after surgery. Spahn et al. 31 reviewed 5- to 8-year follow-up studies on HTO and UKA in a meta-analysis. They found that both surgical methods were reliable in their postoperative efficacy, however, clinical outcomes of UKA were superior to those of HTO. Another study showed that both open wedge high tibial osteotomy (OW-HTO) and UKA are treatment options for the patients aged between 55 years and 65 years, patients should be informed that more residual pain and symptoms will happen after OW-HTO. 32 Furthermore, there are many difficulties to revise TKA after HTO, such as old skin scar affecting the revision incision, ectropion of patella caused by cicatricial adhesion contracture is difficult, need to remove internal fixation, and the local bone foundation is poor. A study from Nwachukwu et al. 33 reported that both UKA and HTO produce satisfactory outcomes if appropriate patients are selected. However, according to their finding, UKA is preferable for patients with unicompartmental OA. One reason is that HTO requires longer rehabilitation and restrictions on weight-bearing. This process may be difficult for patients, especially for older women.
In the past, TKA is most commonly performed in patients with OA. However, in the early postoperative complications, the research showed that the risk of complications was higher in the TKA. 34 Not only that, but the revision of TKA is also a more complicated, more invasive, and longer recovery period. In contrast, UKA, as a minimum invasive surgery, has a main advantage with the preservation of bone stock. According to the study from Cross et al., 35 the functional outcomes of revising a UKA to a TKA are similar to a primary TKA. UKA has provided sufficient anatomical preparation for the risk of revision after UKA in the future. Thus, UKA has been widely used as an alternative to TKA for the treatment of isolated compartmental knee pathologies with minimally invasive surgery techniques and satisfactory longer-term survivorship. 36 UKA has more further advantages in the treatment of AMOA including retention of the cruciate ligaments, higher range of movement, lower morbidity and mortality, and lower rates of infection. 37 –39 In 1989, the research published by Kozinn and Scott detailed contraindications to UKA selection criteria. They reported that young patients (age < 60), obese patients (weigh > 180 pounds), and active patients were contraindicated because of increased risk for prosthesis loosening. Considering that repeated high impact load increases the risk of component failure. 27 However, the polymer polyethylene bearing reduces wear significantly with the improvement of the knee prosthesis, tibial anatomical model covering a better platform to achieve uniform distribution of the stress. 40 The results from 10 years in vitro wear measurement of mobile-bearing UKA showed that the mean linear wear rate was 0.02 mm/year, 41 it’s no doubt that a very low wear rate of bearing offers the device a survival advantage for younger patients. In addition, careful implantation of fully congruous bearings can avoid failure due to polyethylene wear for medial Oxford-UKA. 42 This might be a particular advantage in young and active patients and could be obtained longer postoperative efficacy.
At the last follow-up, one patient underwent total knee revision in case of unexplained knee pain after surgery. A number of studies have shown that unexplained persistent pain is one of the common causes of revision after Oxford-UKA. The pain is mainly near the anterior center of the joint and often occurs weeks or months after surgery. Kim et al. 43 analyzed 89 patients with complications of various reasons after UKA showed that two cases caused by unexplained pain. Hun et al. 44 followed up 246 patients who received UKA for more than 1 year, and the incidence of postoperative complications was 9.8%, a case was revised to TKA for unexplained pain. Bhattacharya et al. 45 explained that the reasons of the unexplained pain after Oxford-UKA may be related with the position of prosthesis or soft tissue stimulation, yet there are still a large number of unexplained causes is difficult to find exact reasons. The conservative treatments for unexplained pain are injection of local anesthetics, glucocorticoids, using anti-inflammatory analgesics, or have a rest. For some patients with chronic intolerable pain, the TKA revision is the only way to treat.
However, the anterior knee pain and patellofemoral arthritis preoperatively should not be regarded as contraindications to UKA. 46,47 In recent years, many studies showed that medial Oxford-UKA can correct the lower limb alignment and remove osteophytes, which can not only effectively relieve the PFJ stress, 29,48,49 but also correct the patellofemoral fit angle, 50 which can effectively relieve anterior knee pain. Consistent with current research, there have been no cases of revision due to patella OA in our joint center so far.
Limitations of this study are a relatively short minimum follow-up, the lack of comparison with TKA, HTO, or >60-year-old UKA patients. However, the results of this study indicated that Oxford-UKA is a reliable choice for young Asian patients with a different lifestyle from Westerners.
Conclusion
Our midterm results showed that the Oxford-UKA was a reliable and effective treatment option for young patients aged less than or equal to 60 years with AMOA. The knee pain can be effectively relieved and excellent functional activities of the knee joint can be obtained after surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support for the research, authorship, and/or publication of this article: Shanghai Health System Advanced Suitable Technology Promotion Project Plan (NO. 2019SY060); Shanghai Municipal Commission of Health and Family Planning (NO. 201840187); Shanghai Municipal Science and Technology Commission (NO. 18411969800); Shanghai Municipal Health Commission (201940249).