
Abstract
Patellar management in primary total knee arthroplasty (TKA) remains one of the most debated and variable aspects of contemporary arthroplasty practice. Patellar resurfacing, non-resurfacing, and selective resurfacing each offer distinct advantages, but no universally superior strategy has emerged. Although global functional outcomes are generally comparable across techniques, differences persist in anterior knee pain, survivorship, patellofemoral degeneration, and the likelihood of secondary patellar procedures. This narrative review synthesizes current clinical, radiographic, biomechanical, and registry-based evidence to provide a comprehensive understanding of these differences. Patellar resurfacing tends to offer clearer benefits in patients with advanced patellofemoral osteoarthritis, significant preoperative symptoms, unfavorable patellar morphology, or implant designs that increase patellofemoral loading. Conversely, non-resurfacing remains a safe and effective option in patients with minimal patellofemoral disease and favorable anatomical characteristics. Selective resurfacing represents a patient-tailored compromise, though its effectiveness is currently limited by the absence of standardized selection criteria. The integration of evidence across multiple studies reinforces that patellar resurfacing should follow an individualized, indication-guided approach instead of routine application. It also proposes a structured framework that incorporates anatomical, radiographic, and implant-related factors to guide patellar management during primary TKA.
Keywords
Introduction
Total knee arthroplasty (TKA) is widely regarded as one of the most successful surgical treatments for advanced knee osteoarthritis, rheumatoid arthritis, and other degenerative conditions of the tibiofemoral and patellofemoral joints. Despite ongoing advancements in implant design, biomaterials, surgical technique, and perioperative protocols, anterior knee pain (AKP) continues to be a leading cause of postoperative dissatisfaction, affecting up to 47% of patients even when component alignment and mechanical stability are adequate.1,2 Within this context, the optimal management of the patella remains one of the most debated aspects of primary TKA. Whether to perform routine resurfacing, selective resurfacing (SR), or retain the native patella is still controversial, with practice patterns varying significantly worldwide.2,3
Patellar resurfacing (PR) was originally introduced to reduce patellofemoral pain, improve functional outcomes, and limit secondary interventions. Early implant designs, however, were associated with complications such as polyethylene wear, fracture, osteonecrosis, maltracking, loosening, and patellar clunk syndrome. 4 As implant designs evolved, many surgeons adopted routine resurfacing, whereas others preferred selective or no resurfacing, raising concerns about implant-related complications, additional cost, and increased operative time.2,3
High-volume clinical studies have further intensified this debate. The Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) demonstrated improved long-term survivorship in resurfaced patellae, particularly in minimally stabilized designs, without an associated increase in mechanical failure.5,6 In line with these findings, Fleaca et al. similarly reported that non-resurfaced (NR) patellae showed higher rates of secondary revision, most commonly for persistent anterior knee pain (AKP), whereas primary PR was associated with lower reoperation rates and a reduced need for secondary procedures. 2 Moreover, multiple studies have consistently documented higher incidences of AKP and secondary interventions when the patella is not resurfaced.2,3,6,7
However, these findings are contrasted by contemporary RCTs and systematic reviews that report no significant differences in clinical outcomes [Knee Society Score (KSS), Oxford Knee Score (OKS), Forgotten Joint Score (FJS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)] or patient satisfaction between resurfaced and non-resurfaced patellae, especially with modern “patella-friendly” femoral components.8–10 Some observations even suggest slightly better postoperative range of motion (ROM) in NR patients. 11 These inconsistencies further emphasize the influence of prosthesis geometry, surgical technique, and individual anatomy on patellofemoral outcomes.
Given these conflicting results, growing attention has turned toward patient-specific and radiographic predictors. Several studies highlight the potential significance of preoperative patellofemoral osteoarthritis (PFOA). Nardelli et al. reported inferior implant survivorship in non-resurfaced TKAs among patients with Iwano stage 3-4 PFOA, 12 and Shon et al. demonstrated poorer outcomes when moderate to severe intraoperative cartilage loss was present in retained patellae. 13 In contrast, Feng et al. found that patient-reported outcomes (PROMs) did not differ according to PFOA severity, indicating that some patients tolerate non-resurfacing even with substantial degeneration. 14 Additional imaging and biomechanical analyses showed progressive postoperative cartilage thinning in unresurfaced patellae 15 and underscored the complex interplay between anatomy, implant geometry, and lower limb alignment in patellofemoral loading, irrespective of resurfacing technique. 16
In response to these contradicting findings, SR has been described as an individualized patellar management strategy, defined as a non-routine intraoperative approach in which the decision to resurface the patella during the index TKA is tailored to patient-specific and patellofemoral characteristics rather than applied systematically. This approach is typically applied in patients considered more likely to benefit, including those with severe patellofemoral osteoarthritis (PFOA), inflammatory arthritis, or preoperative anterior knee pain (AKP). Grela et al. demonstrated comparable functional outcomes between routine PR, SR, and NR approaches, supporting its potential utility. 17 Until now, without a staged and standardized approach, selective resurfacing remains highly surgeon-dependent, often relying on subjective intraoperative evaluations of cartilage quality and patellar morphology.18,19
Despite selective patellar resurfacing being an established option, many surgeons continue to adopt a non-resurfacing approach at the index procedure, performing resurfacing only when distinct clinical or radiographic signs are present. However, this practice introduces a major challenge, specifically the need for secondary patellar resurfacing (SPR). SPR is defined as a subsequent surgical procedure in which a patellar component is implanted after primary total knee arthroplasty in cases where the patella was initially left unresurfaced. Although most commonly performed for persistent AKP after primary non-resurfacing, SPR continues to be a subject of debate. While some studies report improved patient satisfaction after SPR, others note only modest or inconsistent clinical improvement, reinforcing the importance of appropriate initial patellar management.1,3 Predictive models have identified radiographic features such as patellar tilt, width, height, and thickness as risk factors for SPR. 20 Moreover, implant selection may also influence outcomes, as Øhrn observed decreased survivorship of medial-pivot designs compared with cruciate-retaining (CR) prostheses in non-resurfaced patellae. 21 Taking all the above into consideration, it is clear that there is substantial variability and complexity in the outcomes associated with differing patellar management strategies.
Considering the persistent variability, some expert reviews recommend routine patellar resurfacing whenever technically feasible, aiming to minimize postoperative AKP, reduce the need for reoperation, and improve overall patient satisfaction.2,3,6,22 However, despite these recommendations, international practice patterns remain highly heterogeneous. Resurfacing is widely performed in the United States, yet it is adopted far less frequently across many European and Asian countries, reflecting divergent philosophies and training backgrounds.3,18 In view of the inconsistent evidence and considerable international variation in practice, a systematic consolidation of current knowledge is warranted.
This narrative review aims to synthesize the most recent literature addressing the indications, contraindications, and clinical outcomes associated with PR, SR, and NR in the context of primary TKA. Its objective is to comprehensively evaluate and integrate the available evidence, providing a clear and coherent representation of current knowledge in this domain. Building upon these insights and contemporary practice patterns, the review further aims to propose a structured framework for patellar management during primary TKA. To the best of our knowledge, this represents one of the few attempts to develop such a formalized management algorithm, thereby contributing meaningfully to a field characterized by long-standing debate and heterogeneous practice.
Materials and methods
This narrative review was conducted to integrate up-to-date evidence regarding PR, NR, and selective resurfacing strategies in primary total knee arthroplasty (TKA). A narrative review approach was adopted to integrate the diverse body of evidence encompassing randomized controlled trials (RCTs), meta-analyses, observational studies, major registry reports, and biomechanical or imaging investigations. This design was deemed most appropriate given the substantial variability in prostheses design, surgical techniques, patient selection, and outcome reporting across studies.
A structured literature search was performed in PubMed/MEDLINE. The search focused on studies published within the last decade (January 2015 to October 2025), with the final literature search conducted in October 2025. Search terms included patellar resurfacing, non-resurfacing, selective resurfacing, total knee arthroplasty, anterior knee pain, patellofemoral osteoarthritis, and secondary patellar resurfacing. Reference lists of retrieved studies and relevant systematic reviews were manually screened to identify additional eligible publications.
Studies were included if they met the following criteria 1 : adult patients undergoing primary TKA, 2 interventions involving PR, NR, or selective resurfacing, and 3 reporting outcomes such as Knee Society Score (KSS), Oxford Knee Score (OKS), Forgotten Joint Score (FJS), anterior knee pain, revision or reoperation rates, patellofemoral complications, radiographic progression, survivorship, or predictors of outcome. Eligible study designs included randomized controlled trials, prospective or retrospective cohort studies, registry analyses, biomechanical or imaging studies, and systematic reviews. Exclusion criteria were revision TKA, unicompartmental knee arthroplasty, case reports, non-English publications, preclinical studies, and studies lacking extractable data relevant to patellar management. Overall, approximately 35 studies were included in the narrative synthesis.
Results
This narrative review integrates the most up-to-date evidence on patellar management in primary TKA, focusing on comparative clinical outcomes, anterior knee pain, revision rates, complication profiles, degenerative progression, and predictors of success or failure across resurfacing (PR), non-resurfacing (NR), and selective resurfacing strategies. The results presented below provide a detailed assessment of the clinical performance, risks, and indications associated with the various patellar management strategies.
Comparative clinical outcomes of resurfacing and non-resurfacing
Functional scores and clinical outcomes
Evidence from RCTs, meta-analyses, and cohort studies did not reveal statistically significant differences in clinical outcomes (KSS, OKS, FJS) or knee ROM between PR and NR.4,8,10,17,23 In line with these findings, Deroche et al. observed similar AKP and FJS outcomes with a modern patella-friendly design; however, the NR group experienced a twofold increase in stair-climbing pain, and 3.6% later required SPR. 8 These observations contrast with findings from the RCT by Ha et al., which showed significantly better outcomes with PR, including higher KSS and Feller scores. 6 Providing further support from mid-term follow-up data, a recent retrospective cohort study by Sağlam et al. with a minimum 5-year follow-up reported significantly lower pain levels and superior WOMAC scores in patients who underwent PR compared with those managed with NR, independent of tibial insert type. 24
Meta-analyses offer a more detailed understanding of these outcomes. In their respective studies, Fu et al., Longo et al., and Migliorini et al. reported small but statistically significant advantages for PR in pain-specific outcomes and patient satisfaction, though differences in global functional scores remained limited.25–27 However, several studies demonstrate clear exceptions to this general pattern. In the study by Upadhyay, transient early improvements in OKS were reported among patients who underwent PR. 4 Tang’s meta-analysis also demonstrated superior patellar-specific scores in the PR group (MD 1.24; p < 0.001). 11 Similarly, Thilak and Palan reported improved patellofemoral-specific outcomes with PR, despite overall functional results being comparable between PR and NR groups.7,28 Importantly, the RCT by Ha et al. provided strong mid-term evidence supporting PR, showing significantly lower AKP, reduced patellar crepitus, and a markedly higher patient preference (47% for PR vs. 7% for NR), further reinforcing the patellofemoral advantages of resurfacing. 6
Range of motion (ROM)
ROM outcomes demonstrate a slight preference toward NR. Migliorini et al. reported slightly greater ROM in the NR group of patients, although the difference was clinically negligible and unlikely to affect decision-making independently. 27 Further clarifying the determinants of postoperative ROM, Sağlam et al. demonstrated that improvements in flexion and reduced extension limitation were primarily associated with the use of mobile-bearing (MB) tibial inserts rather than with PR status itself, reinforcing the concept that implant design exerts a greater influence on postoperative ROM than patellar management alone. 24 Overall, PR and NR yield similar global functional results, with occasional differences favoring patella-specific outcome measures.
Anterior knee pain (AKP)
AKP reduction with resurfacing
Patellar resurfacing (PR) consistently demonstrates lower rates of anterior knee pain (AKP) across high-level evidence. Tang reported a 28% relative risk reduction in AKP with PR (RR 0.72; p = 0.006), and a similar pattern is evident in the RCT by Ha et al., the meta-analyses summarized by Samih et al., and the findings of Fleaca et al. and Sağlam et al., who also observed reduced AKP with PR.2,6,10,24 Earlier systematic evaluations by Longo, Migliorini, and Fu likewise favored PR, showing reduced AKP and improved pain-related outcomes.25–27 Registry and cohort data further support these findings; Woelfle et al. observed that NR patellae more commonly develop progressive PFOA, often necessitating SPR. 18
AKP can persist despite resurfacing
PR decreases but does not eliminate AKP. Multifactorial contributors such as maltracking, extensor mechanism imbalance, and soft-tissue pathology may play a more dominant role than cartilage-related pain in many cases. 10 Moreover, SPR seldom results in complete symptom resolution.10,18 Therefore, despite the overall reduction in AKP with PR, residual symptoms could be attributed to mechanical issues rather than chondral pathology.
Revision rates and survivorship
Patella resurfacing (PR) reduces need for secondary surgery
A consistent finding across studies is the lower incidence of SPR and patellofemoral revision with PR. Tang (2024) reported significantly reduced patellar (RR 0.41) and non-patellar (RR 0.64) revision rates in the PR cohort. 11 Similarly, Woelfle et al. observed substantially higher patellofemoral reoperation rates in NR (7.6%) compared with PR (0.3%), with 6.8% of NR patients ultimately requiring SPR. 18 Deroche et al. likewise documented a 3.6% early SPR rate among NR patients. 8 Large registry analyses further corroborate these findings. Data from the AOANJRR demonstrated significantly lower cumulative revision rates with PR across implant categories, 5 and Øhrn et al. reported reduced survivorship in NR knees, particularly when medial pivot designs were used. 21
Outcomes of secondary patellar resurfacing (SPR)
SPR provides limited and inconsistent clinical benefit, as demonstrated across contemporary literature. Fleaca et al. reported that only 44% of patients experience meaningful improvement following SPR, while more than 50% continue to suffer from persistent AKP. In addition, SPR carries substantial risks, including infection, instability, patellar fracture, and wound complications – factors that contribute to its overall unpredictability. 2
Recent clinical data further reinforce these concerns. Vermue et al. reported that although SPR improved KSS function score, it did not produce corresponding improvements in KSS knee score, with overall patient satisfaction limited to 81% and a complication rate of 10%. 1 Earlier evidence from Woelfle et al. similarly demonstrated that merely 64% of patients achieved clinically meaningful improvement after undergoing SPR. 18
Taken together, the cumulative evidence from Fleaca et al., Vermue et al., and Woelfle et al. underscores the relative unreliability and inferior effectiveness of SPR when compared to primary resurfacing. These findings provide strong support for primary patellar resurfacing in patients at higher risk of patellofemoral symptoms, as early intervention may help prevent persistent AKP and decrease the likelihood of secondary procedures.
Complications associated with resurfacing (fracture, loosening, maltracking, and instability)
Although uncommon, patellar fractures occur more commonly following PR. In the study by Woelfle et al., with a mean follow-up of 23.6 months (range 12.0-66.9 months), fractures were observed in 1.3% of PR (5/386) compared with 0.8% of NR patellae (1/118). Notably, no cases of patellar component loosening were identified in the PR cohort, whereas patellar instability was documented exclusively in the NR group (0.8%). 18 Additional PR-specific complications such as component loosening, button malposition, patellar maltracking and instability (early or late), have been highlighted in narrative and systematic reviews. In conjunction with these issues, other factors such as overstuffing and compromised patellar vascularity, especially following lateral release, further contribute to the risk of fracture and instability in PR.4,7,22 Taken together, these data underline that although the overall incidence of complications after PR remains low, PR carries distinct risks that necessitate meticulous surgical technique and careful patient selection.
Degenerative progression in non-resurfaced patellae
Structural deterioration of the patellar is reported more frequently in NR. Sato et al. reported substantial progression of patellofemoral degeneration, including more than 50% cartilage loss within 5 years, progressive lateral facet thinning, and increasing tilt and shift. 15 Consistent with these observations, Woelfle et al. documented several cases in which NR knees progressed to severe patellofemoral osteoarthritis necessitating SPR. 18 Moreover, evidence by Fu et al. indicated a greater propensity for degenerative progression in NR patellae. 25 Collectively, these findings suggest that NR may predispose patients to accelerated patellofemoral structural deterioration, particularly in the presence of patellar dysplasia or maltracking.
Summary of comparative outcomes across various patellar management strategies in primary TKA.

Abbreviations: PR: Patellar Resurfacing, NR: Non-Resurfacing of the patellar, KSS: Knee Society Score, OKS: Oxford Knee Score, FJS: Forgotten Joint Score, ROM: Range of motion, AKP: Anterior Knee Pain, SPR: Secondary Patellar Resurfacing, PF: Patellofemoral, PFOA: Patellofemoral Osteoarthritis, MP: Medial-Pivot.
Influence of implant design and surgical technique
Modern implant designs appear to narrow the performance gap between PR and NR. Patella-friendly trochlear geometries and refined femoral component designs have improved patellofemoral kinematics, reduced contact stresses, and minimized complications traditionally associated with leaving the patella unresurfaced. Deroche et al. demonstrated that such modern trochlear designs mitigate patellofemoral complications, making NR a safe and reliable option when alignment is appropriate. 8 Similarly, McConaghy et al. emphasized that technical factors such as accurate femoral component rotation, restoration of limb alignment, preservation of patellar thickness, optimal trochlear geometry, and extensor mechanism balance, often exert greater influence on postoperative patellofemoral mechanics than the resurfacing decision itself. 16 When these parameters are optimized, patellar tracking, retropatellar contact forces, and overall joint mechanics improve, reducing the risk of AKP, maltracking, and instability regardless of resurfacing.
Beyond general design principles, specific implant categories interact differently with the patellofemoral joint and therefore influence the appropriateness of resurfacing. Medial pivot (MP) designs have demonstrated variable outcomes depending on implant generation and biomechanical characteristics. Earlier registry data indicated that MP systems, which impose greater patellofemoral contact forces, were associated with poorer outcomes when the patella was not resurfaced. 21 However, more recent analyses of newer MP designs engineered to optimize load distribution and replicate native knee kinematics have shown favorable early postoperative results even without resurfacing, suggesting that contemporary pivoting systems may reduce the necessity for PR in select patients. 30 In contrast, posterior-stabilized (PS) prostheses impose greater mechanical interaction on the patellofemoral joint. PS implants may increase the risk of patellar clunk or crepitus when the patella is not resurfaced, and registry evidence indicates higher rates of secondary resurfacing in PS knees treated without PR. 31 Accordingly, PR may be more advantageous when using PS systems, especially in patients predisposed to AKP. Cruciate-retaining (CR) implants generally exert less constraint on patellar tracking, though resurfacing may still be advisable in cases of patellofemoral incongruence or preexisting cartilage damage. 32
Large registry data further show that both younger patients and those receiving PS implants have higher SPR rates when initially left unresurfaced, demonstrating that implant design can independently influence long-term patellofemoral outcomes. 33 In this context, recent clinical evidence from the study of Sağlam et al. demonstrated that the effectiveness of PR is closely linked to implant characteristics, particularly tibial insert design. Specifically, the most favorable pain relief, functional outcomes (WOMAC), mobility (TUG), and knee range of motion were observed in patients receiving MB inserts combined with PR, whereas fixed-bearing implants without resurfacing were associated with the poorest overall outcomes. 24 Nevertheless, advances in trochlear geometry and polyethylene formulations have reduced these disparities, with modern designs improving outcomes for both PR and NR across patient age groups.
Overall, implant design remains a central determinant of patellar management strategy in primary TKA. Older or less patella-friendly systems as well as PS implants with greater patellofemoral interaction often justify routine PR to reduce the risk of postoperative complications. In contrast, contemporary MP and modern trochlear-optimized designs increasingly support a selective, individualized approach in which PR is guided by patient anatomy, preoperative symptoms, and patellofemoral risk profile rather than by implant choice alone. As implant technology continues to evolve, the emphasis is shifting toward matching prosthesis-specific biomechanics with patient-specific characteristics, enabling more precise and reliable optimization of patellofemoral outcomes.
Age-related considerations
Age alone should not dictate patellar management in primary total knee arthroplasty (TKA), but it meaningfully interacts with patient comorbidity, functional status, implant design, and expected postoperative activity. Evidence suggests that older patients may derive greater benefit from patellar resurfacing, largely due to lower activity levels and reduced mechanical stresses. Studies have shown that resurfacing may decrease anterior knee pain in older individuals and may be relatively indicated when preexisting patellofemoral arthritis or advanced age is present. 34 Additionally, patients over 80 years demonstrate excellent survivorship with either resurfaced or non-resurfaced patellae, although functional outcomes naturally decline with age. 8
A significant age threshold appears at 65 years. Patients younger than 65 have higher rates of aseptic patellar complications following resurfacing, whereas older patients experience fewer resurfacing-related problems, suggesting a paradoxical age-related protective effect. 31 Furthermore, frailty, comorbidity burden, and functional dependence become powerful modifiers of outcome beyond chronological age alone. For patients over 75, particularly those with multimorbidity or limited mobility, resurfacing may help avoid secondary surgeries – an important consideration in populations with higher surgical risk profiles.
Interestingly, registry data indicate that younger patients (50-59 years) are more likely to undergo primary resurfacing or later require secondary resurfacing when initially untreated, highlighting an age-related trend toward proactive patellar management in this group as well.2,6,33 However, modern “patella-friendly” prosthesis designs may reduce age-related differences altogether, as comparable early outcomes have been reported regardless of resurfacing status across age groups. 30
Overall, patient age should be integrated into a broader individualized decision-making framework that considers comorbidities, frailty, functional expectations, anterior knee pain history, and implant design features. No single age cutoff universally determines the need for resurfacing, and both selective and routine strategies may be appropriate when applied based on patient-specific factors. 35
Comorbidities
Patient comorbidities have a major influence on patellar management in primary TKA and often provide more substantial guidance than age alone. A higher overall comorbidity load (such as a Charlson Comorbidity Index ≥4) and increased frailty are consistently linked to poorer surgical outcomes and recovery. As a result, minimizing the likelihood of future reoperations becomes a priority, which frequently favors primary patellar resurfacing in older patients with multiple health conditions.36–38
Patterns associated with elevated risk: Cardio-renal-metabolic clusters (diabetes, cardiovascular disease, chronic kidney disease, anemia), which increase complications, infections, readmissions, and mortality.37,38 Frailty + cognitive impairment + functional dependence, which predict delirium, prolonged stay, and higher mortality; these patients are poor candidates for secondary procedures and generally benefit from “one-stage” solutions including resurfacing.39–41 Diabetes + obesity ± depression, which increase PJI risk, particularly with additional surgery; in such profiles, resurfacing at the index TKA may be preferred to avoid secondary patellar operations.
42
Modern risk tools such as the Charlson Comorbidity Index (CCI), Hospital Frailty Risk Score (HFRS), 5-Item Modified Frailty Index (mFI-5) can help stratify these comorbidities and support a personalized, comorbidity-driven approach: low-risk patients can safely follow selective resurfacing strategies, whereas high-risk, frail, multimorbid patients are often managed with primary resurfacing to minimize later surgical burden.36,38,40,43–46
Predictors of success or failure
Predictors favoring resurfacing
Within the current literature, a substantial body of studies outlines several criteria favoring PR. Severe patellofemoral osteoarthritis, particularly Iwano grades 3 and 4, has repeatedly been associated with reduced survivorship when managed with NR.3,12 Preoperative anterior knee pain is another consistent indicator supporting resurfacing, as emphasized in the reviews by Migliorini, Longo, and Palan.2,3,6,7,26,27 Implant design also plays an important role; medial pivot systems, which place greater biomechanical demands on the patellofemoral articulation, have demonstrated poorer outcomes when the patella is left unresurfaced. 21 Intraoperative identification of severe articular cartilage loss provides an additional rationale for performing PR.2,3,13 Patellar maltracking or dysplasia further supports resurfacing, as documented by Sato et al., Usman et al. and Molfetta et al.3,15,29 Finally, anatomical features such as lateral facet overload or abnormal patellofemoral morphology are recognized indications for PR.3,16
Predictors favoring non-resurfacing
Patients who are likely to perform well without PR generally exhibit favorable patellofemoral characteristics. These include normal patellar morphology, height, tilt, and thickness, as well as mild or absent patellofemoral osteoarthritis.2,3,14,17,20 Outcomes also tend to be reliable when modern patella-friendly TKA designs are used, as demonstrated by Deroche et al. 8
Contraindications to resurfacing
Contraindications to PR have been consistently emphasized across the existing literature. A patella measuring less than 12 mm in thickness is widely regarded as a contraindication due to the increased risk of fracture.3,10,16 Vascular compromise, especially in the setting of a lateral release, represents a significant deterrent to resurfacing because of its association with higher postoperative complication rates. 18 In addition, complex patellar morphology that prevents safe component placement represents a further limitation. 19 Severe osteoporosis or poor bone stock has likewise been identified as a condition in which PR should be avoided.3,16
Predictors, indications, and contraindications for PR and NR in primary TKA.
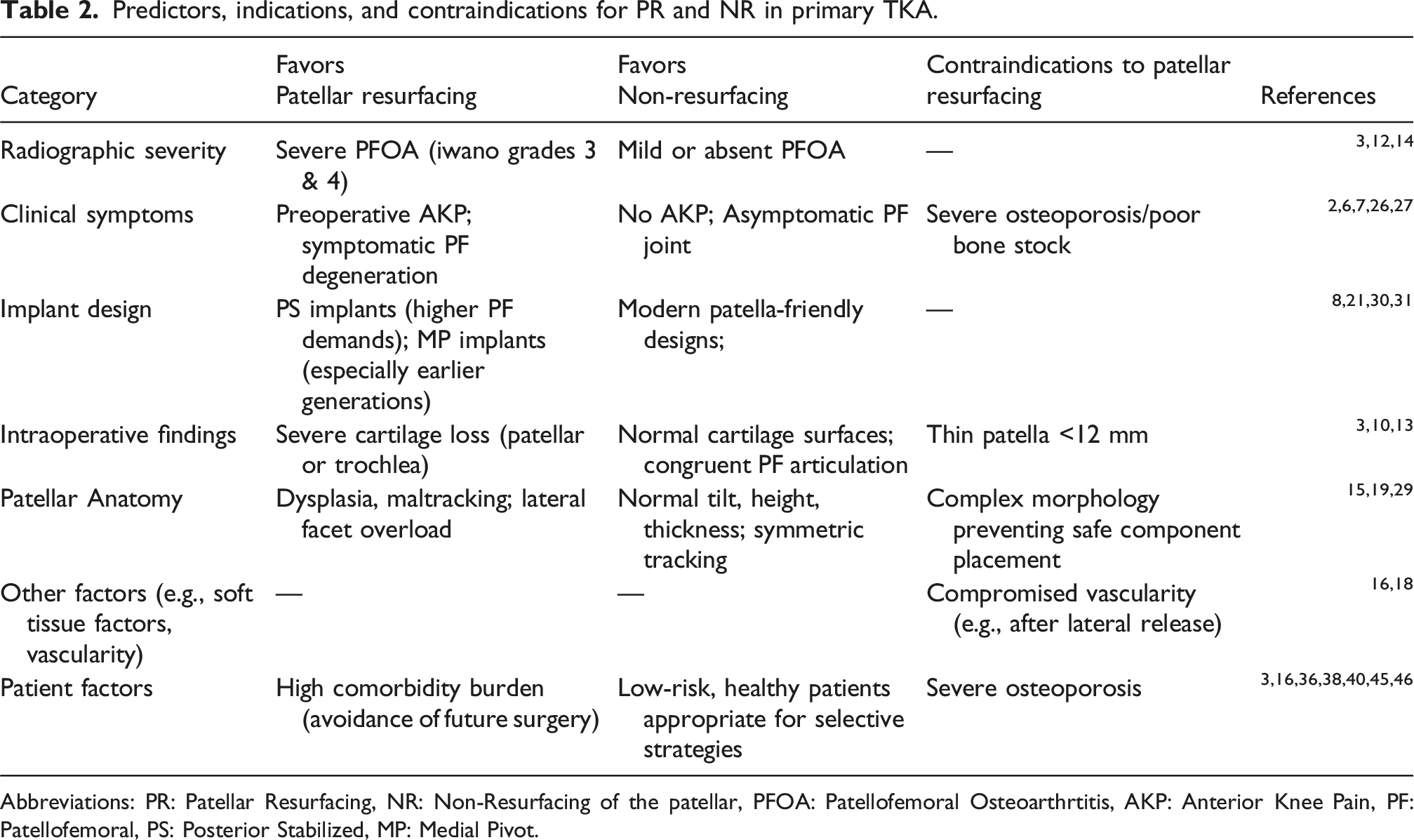
Abbreviations: PR: Patellar Resurfacing, NR: Non-Resurfacing of the patellar, PFOA: Patellofemoral Osteoarthrtitis, AKP: Anterior Knee Pain, PF: Patellofemoral, PS: Posterior Stabilized, MP: Medial Pivot.
Selective resurfacing strategies
Selective resurfacing demonstrated comparable outcomes between the PR and NR groups in the study by Grela et al. 17 However, an important limitation of this analysis is that the treatment groups were not stratified according to PFOA severity. Consequently, patients with moderate-to-severe PFOA, conditions for which contemporary evidence increasingly favors resurfacing, may not have been consistently allocated to PR cohorts. This lack of severity-based allocation introduces clinical heterogeneity and may attenuate true differences between treatment strategies. Moreover, as emphasized by Iordache et al., selective resurfacing continues to lack standardized selection criteria and remains heavily dependent on surgeon judgment, thereby contributing to variability in its application and reported outcomes. 19
Discussion
The management of the patella in primary TKA remains controversial. While numerous RCTs, meta-analyses, registry studies, and biomechanical investigations demonstrate broadly comparable global
High-quality trials using modern patella-friendly femoral designs report equivalent
One of the most consistent advantages of PR is its association with lower rates of
However, AKP is multifactorial and may persist after PR due to maltracking, malrotation, soft-tissue imbalance, or extensor mechanism dysfunction – factors not addressed by resurfacing alone.10,16 Importantly, SPR after NR is unpredictable, with symptom improvement reported in only 44-64% of cases.2,18 Advanced imaging supports these findings; SPECT/CT analysis by Wu et al. demonstrated metabolically active patellofemoral pathology in symptomatic NR knees, highlighting the role of the pre-existing anatomy and joint loading patterns to postoperative pain 47 . These data underscore that AKP reflects a complex interaction of cartilage status, morphology, alignment, implant geometry, and soft tissues rather than resurfacing status alone.
Among all clinical outcomes,
In addition to clinical and revision data, imaging and biomechanical studies offer crucial insights into the structural consequences of retaining the native patella, consistently demonstrating progressive
The
Although implant design and surgical technique shape patellofemoral mechanics,
Decision Framework for Patellar Management in primary TKA.

Abbreviations: PFOA: Patellofemoral Osteoarthrtitis, AKP: Anterior Knee Pain, CR: Cruciate Retaining, MP: Medial Pivot, PS: Posterior Stabilized SPR: Selective Patellar Resurfacing, PF: Patellofemoral.
On the other hand, a number of situations support the choice of
Taken together, the evidence demonstrates that optimal patellar management in primary TKA cannot rely on a single uniform strategy but must instead be tailored to the interplay of anatomical, biomechanical, implant-specific, and patient-related factors. While PR consistently reduces AKP, lowers patellofemoral revision rates, and offers superior survivorship – particularly in the presence of advanced PFOA, inflammatory arthritis, patellar dysplasia, or high-stress implant designs – NR remains an appropriate option for patients with mild or asymptomatic PFOA, favorable patellar morphology, and poor bone quality. Imaging and biomechanical studies highlight the structural deterioration and increased risk of later SPR when diseased patellae are left unresurfaced, whereas registry findings emphasize the influence of implant choice, especially with designs such as PS system that impose greater patellofemoral loads. At the same time, age, comorbidity burden, and frailty further refine decision-making, as older or medically complex patients benefit from strategies that minimize the risk of secondary procedures. The integration of radiographic predictors, cartilage status, patellar shape, limb alignment, implant biomechanics, and patient-specific clinical factors provides the foundation for an evidence-based, indication-driven algorithm. Within this framework, PR and NR should be viewed not as opposing philosophies but as complementary strategies that, when selectively applied, optimize pain relief, function, and long-term survivorship in TKA.
Proposed treatment framework for patellar management in primary TKA
To support consistent and evidence-based decision-making, we developed a stepwise treatment framework for patellar management in primary TKA that integrates preoperative, implant-specific, and intraoperative determinants (Figure 1). This framework is presented as a hypothesis-generating, evidence-informed decision-making model rather than a validated clinical guideline and is intended to synthesize current knowledge rather than dictate practice. This multi-step algorithm integrates preoperative, implant-specific, and intraoperative determinants known to influence outcomes related to anterior knee pain, patellofemoral kinematics, and postoperative function. Although based on the current body of evidence, the proposed framework has not been prospectively validated and should therefore be interpreted as a conceptual tool that requires confirmation through future prospective, ideally multicenter, clinical studies before widespread adoption. Patellar management in primary total knee arthroplasty: A proposed stepwise treatment framework. Abbreviations: CR: Cruciate retaining, PS: Posterior Stabilized, MP: Medial pivot. A Proposed Comprehensive Algorithm for Patellar Management Decisions in Primary Total Knee Arthroplasty. Abbreviations: PR: Patellar Resurfacing, NR: Non-Resurfacing of the patellar, AKP: Anterior Knee Pain, SPR: Secondary Patellar Resurfacing, PF: Patellofemoral, PFOA: Patellofemoral Osteoarthritis, CR: Cruciate Retaining, PS: Posterior Stabilized, UC: Ultra-Congruent, MP/MC: Medial-Pivot/Medial Congruent, MLC: Midlevel Constraint, BCS: Bicruciate Stabilizing, LP: Lateral Pivot.


As part of this initial assessment, it is essential to establish whether the patient experiences AKP, since its presence strongly influences the suitability of PR. To standardize the assessment of AKP, a structured preoperative screening framework incorporating patient’s history, physical examination, PROMs, and imaging findings is applied (Figure 3). Preoperative screening for anterior knee pain: A structured clinical assessment framework. Abbreviations: Akp: Anterior knee pain, PROMs: Patient-reported outcome measures, PF: Patellofemoral, PFOA: Patellofemoral osteoarthritis.

Conclusion
The management of the patella in primary total knee arthroplasty (TKA) remains one of the most persistent and multifaceted challenges in contemporary arthroplasty, with evidence showing that no single approach is universally superior. Although overall functional outcomes are similar across strategies, resurfacing offers advantages in reducing anterior knee pain, limiting patellofemoral-related revisions, and avoiding secondary resurfacing in patients with advanced degeneration or biomechanical risk factors. Non-resurfacing remains appropriate when patellofemoral disease is minimal and anatomical and biomechanical conditions are favorable.
Optimal decision-making requires incorporating patient anatomy, cartilage quality, limb alignment, implant design, and surgical precision, as well as broader factors such as age, comorbidities, frailty, and expected activity levels. Thus, selective resurfacing can be effective when guided by clearly defined radiographic and clinical criteria, but its success depends on consistent application and adequate evaluation of patellofemoral pathology.
In this context, our effort to propose a conceptual framework for patellar management in primary TKA aims to provide clinicians with a structured, evidence-based approach that integrates patient-specific, implant-related, and intraoperative determinants. By synthesizing these elements into a reproducible algorithm, we seek to enhance decision-making consistency, reduce unnecessary variability in practice, and ultimately improve patellofemoral outcomes.
Future improvement in patellar management will rely on standardized assessment tools, patellofemoral-specific outcome measures, and refined selection algorithms. Ultimately, resurfacing and non-resurfacing should be viewed as complementary strategies that, when applied thoughtfully, can optimize long-term function, patient satisfaction, and implant durability in primary TKA.
Footnotes
Ethical considerations
Ethical approval was not required for this study.
Author contribution
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.