
Abstract
Introduction
Amputation is a very painful functional experience not only for a patient but also for their near and dear ones.1,2 Optimal rehabilitation of an amputee is a team effort and should start prior to amputation if feasible and be continued in the early post-operative period till functional restitution is achieved.3–5 Apart from various other reasons, functional restoration depends upon the type of prosthesis available to an amputee.3,6 It is often noticed that the affordable subjects are well rehabilitated with advanced functional prosthesis and the non-affordable ones adjust themselves with the suboptimal prosthesis barring few exceptions or even live without any rehabilitative prosthesis for various reasons.7–10 We report our experience of providing advanced artificial limbs at free of cost to the underprivileged through a state-sponsored pilot initiative.
Material and methods
This is a retrospective cohort study of 136 amputees who have been referred to the Department of Orthopaedics at Nizam's Institute of Medical Sciences, Punjagutta, Hyderabad, India from all over the state of Telangana between November 2017 and February 2021 for the provision of advanced artificial limbs (n = 142) through a pioneering state-sponsored pilot initiative to rehabilitate the amputees who cannot otherwise afford the same. Manuscript was submitted to the institutional ethical committee (IEC) of Nizam's Institute of Medical Sciences before submitting for publication. This being a retrospective analysis of available data, information to IEC was sufficient and ethical committee review exemption and approval was deemed granted.
Generic specifications for above elbow, above knee, below elbow and below knee prosthesis were prepared by studying and taking inputs from various suppliers of advanced artificial limbs in the market. Coding with approximate budget for each of the prosthesis was prepared including the K levels and 3 years warranty. A committee comprising of senior orthopaedic surgeons from various government hospitals was formed to finalize the formulated generic specifications. Global tender schedule was prepared by incorporating the finalized specifications. Technically sound pre-qualified vendors were selected by a technical evaluation committee comprising of experts from various institutes after taking a live demonstration of their quoted items. Price bids were opened for the technically qualified codes of various vendors and vendors with least price for a given code was finalized (Table 1).
List of some commonly used advanced artificial limbs in each category with specifications and price.
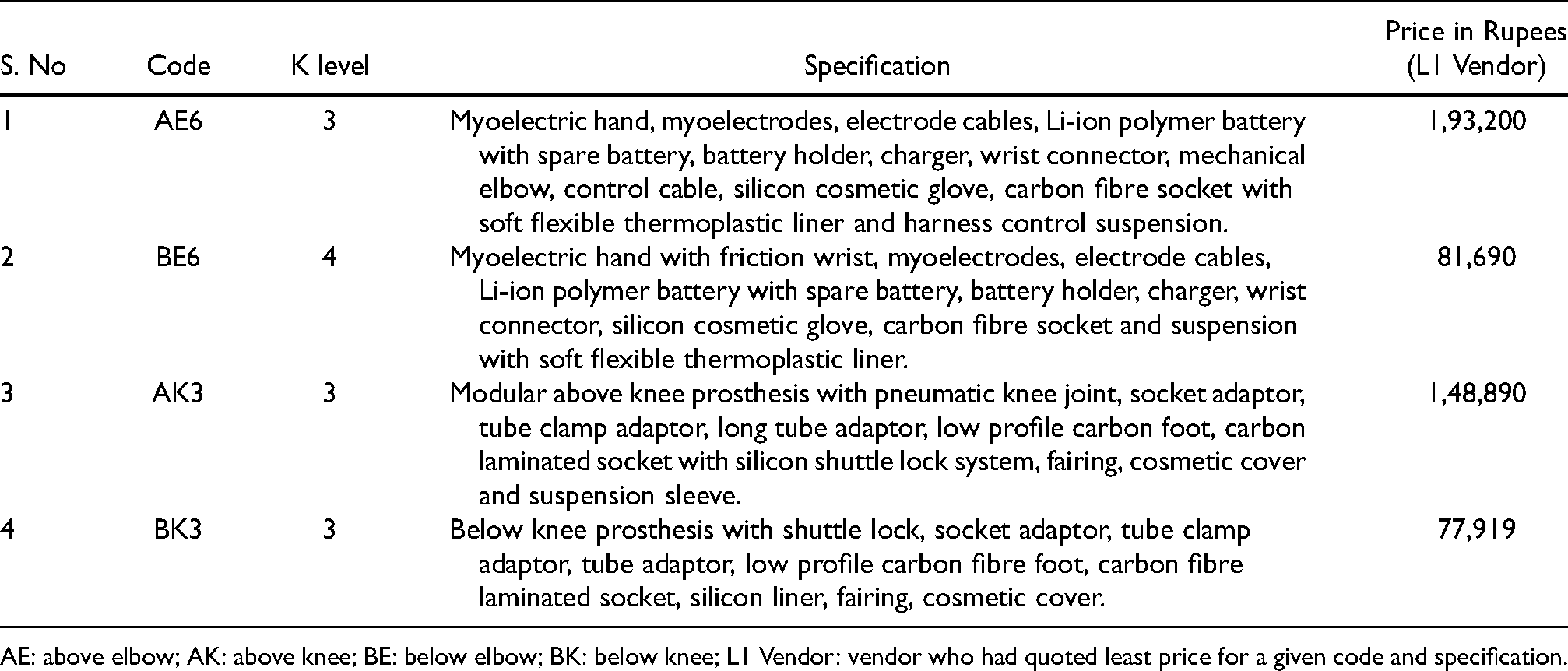
AE: above elbow; AK: above knee; BE: below elbow; BK: below knee; L1 Vendor: vendor who had quoted least price for a given code and specification.
Rehabilitation with advanced artificial limbs was carried out by adopting a replicable process. Initial evaluation, recommendation of a specific prosthesis to a given patient and issuance of estimation for the Chief Minister's relief fund (CMRF) was done in the first visit of the amputee. The amputee's attendant would apply for CMRF and once sanctioned, they would submit the original CMRF credit letter to a designated Orthopaedic surgeon for processing and procurement of the befitting prosthesis. After ascertaining the feasibility of procurement for a given prosthesis, indent was raised through proper channel (Head of the department/Unit chief) to the controller of surgical stores who would in turn forward the indent to the supplier with a request to supply the required prosthesis. Having received the request letter, the prosthetist attached to the vendor agency would take the measurements of the stump, customize the artificial limb, train the subject and submit the artificial limb to the central stores of the institute within 45 days. Once received, the subject would be admitted for final fitment and functional assessment. Feedback/satisfaction letter would be taken and utilization certificate was generated after the subject is discharged (Table 2). Self-Assessment Scoring (SAS) System – an indigenous, comprehensive, simple and all-inclusive method devised by the authors was followed to evaluate this system and provide feedback to the government authorities/funding agencies. Finance section would claim the final bill from CMRF duly producing all the requisite documents. All the amputees supported under this scheme received advanced prosthesis at free of cost with 3 years of replacement warranty. Statistical analysis was done using MedCalc (Ver.19.5.1).
Self-assessment Scoring (SAS) system.
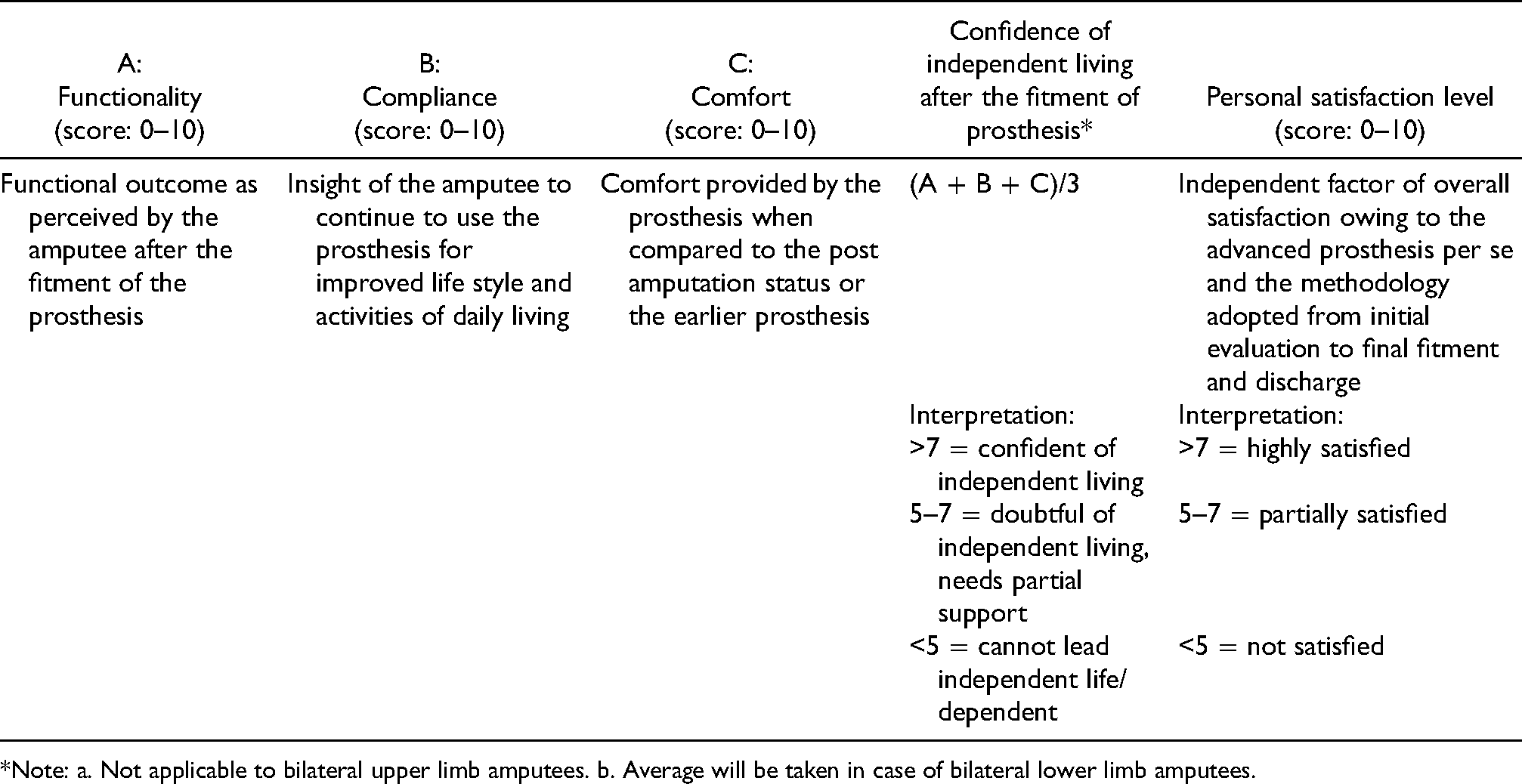
*Note: a. Not applicable to bilateral upper limb amputees. b. Average will be taken in case of bilateral lower limb amputees.
Results
Out of the total 136 subjects served in this pilot project, 92% (n = 125) subjects were men and 8% (n = 11) were women. Of these 136 subjects, 142 artificial limbs were provided. One hundred and thirty subjects received unilateral and 6 subjects received bilateral prosthesis. Eighty-eight percent (n = 125) of the total prosthesis supplied were lower limb prosthesis and 12% (n = 17) were upper limb prosthesis. 54.4% (n = 68) of the lower limb prosthesis were above knee and 45.6% (n = 57) were below knee prosthesis. Forty-seven percent (n = 8) of the upper limb prosthesis were above elbow and 53% (n = 9) were below elbow prosthesis. Of all the prosthesis supplied, codes AK3 and BK3 (n = 41 and 51, respectively) were the commonly used prosthesis (Table 3). All the amputees fitted with advanced artificial limbs were highly satisfied at the end of the procedure and were confident of independent living to the best possible extent (Figures 1 and 2).

Picture depicting amputees replacing their exoskeleton above knee prosthesis with advanced endoskeleton prosthesis.
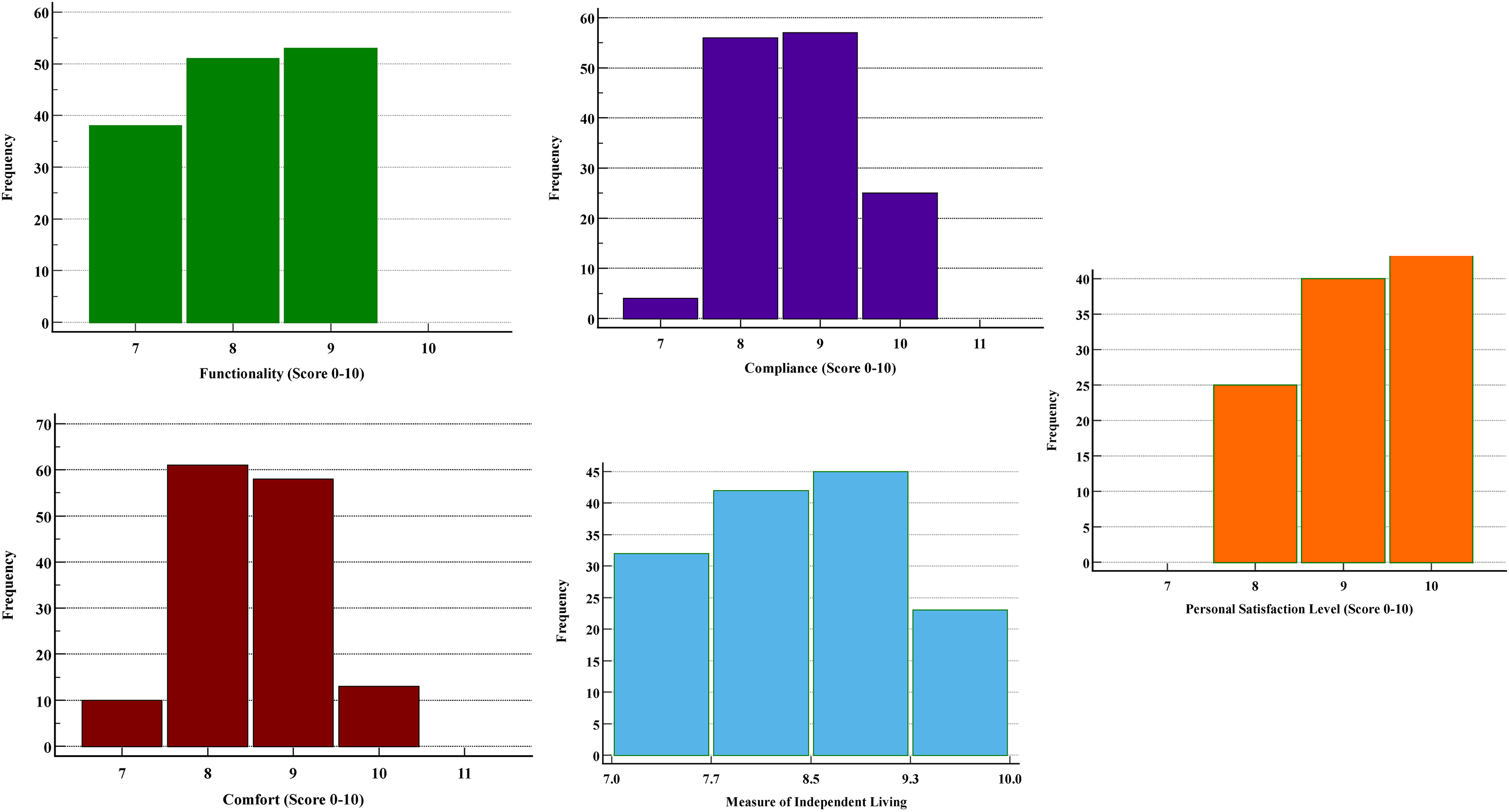
Graphical representation of the Functionality, Compliance, Comfort and Confidence of independent living and overall satisfaction.
Summary statistics.
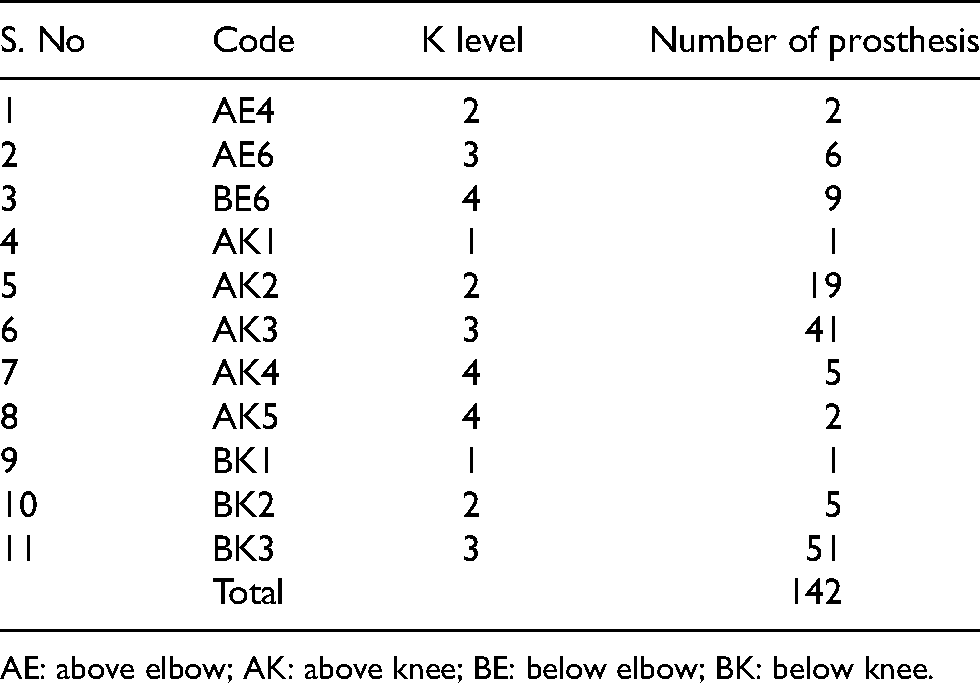
AE: above elbow; AK: above knee; BE: below elbow; BK: below knee.
Discussion
Amputation is the last resort for a surgeon when a limb cannot be salvaged and at times a sole means to save a life. It causes severe mental and physical agony to the suffering patient and their family.1–3 Youngsters are the most common victims owing to high-velocity motor vehicle accidents apart from vaso-occlusive, infectious, congenital and neoplastic etiologies.11,12 Lower limb amputations and prosthesis used here in this report are more common than the upper limb prosthesis akin to the earlier reported literature. 13 Early rehabilitation plays an important role in restoring the amputees back to life so that they can support themselves and contribute to their family.3,4 Adequate rehabilitation requires concerted efforts from the family and the society as a whole including the health care delivery system. 5 Getting the amputees back to near normal function involves the provision of a suitable/ideal prosthesis which can anatomically and physiologically replace the lost limb.3,6 Apart from the functional restitution, ideal prosthesis spares the ipsilateral and contralateral joints from early wear and tear due to compensatory over usage or strain and allow greater independence by decreasing the performance-based additional workload and reaction time.14–18 Ideal prosthesis is costly and most of the amputees cannot afford it. As a means of financial adjustment, most of the amputees settle down with prosthesis like mechanical /cosmetic hand, Jaipur foot/ Sach foot, exoskeleton above knee prosthesis with manual hinges and primitive sockets as against myoelectric hand, carbon foot, endoskeleton prosthesis with pneumatic/hydraulic/microprocessor knees with shuttle lock adaptors, carbon fibre sockets and total contact silicon soft liners which optimize the biomechanical properties of otherwise passive prosthesis. Sometimes, they end up not using any prosthesis at all.3,7,19–23 Many of them abandon those prosthesis for various reasons after a short period of usage and few continue them to use only to present later on with strain pattern about the supporting structures and joints.7–10,14 Few fortunate amputees have the privilege of utilizing state funds for procuring advanced prosthesis. They were sanctioned the complete amount or partially basing on the evaluation, estimation and recommendation of private prosthetists in the past. Lack of established systems to address this issue in the past had posed a significant burden on the exchequer owing to frequent overestimations from the private vendors of advanced artificial limbs.
As of means of bridging the gap in this field of rehabilitation, a pilot project was designed by the Department of Orthopaedic surgery at Nizam's Institute of Medical Sciences, Punjagutta, Hyderabad, India and was fully supported by the Government of Telangana to procure advanced artificial limbs from renowned vendors through rate contact. By this process, we could procure advanced prosthesis at reasonably lower rates (30% to 70% lesser than the earlier market rates) duly saving public money released by the state through various means for the said purpose and could support as many amputees as possible without compromising on the quality of the prosthesis or the requirements of the amputee. This curbed the earlier private practice of overestimation and inappropriate recommendations owing to the scientific process followed in the selection of an appropriate prosthesis for an appropriate amputee including the K levels. State government relied upon such standardized institutional practice for the study period by releasing CMRF only to the institute and routed all such cases through this channel. All the amputees rehabilitated under this programme were highly satisfied with the prosthesis supplied and were confident of independent living to the best possible extent as per the SAS system to prove the fact that an experienced and dedicated team effort can achieve the goal of earliest and highest possible functional restitution.24,25
Having accomplished the successful fitment of 142 prosthesis in a single institution, few areas in this field were felt to be addressed like addition of disarticulation prosthesis and few more varieties of prosthesis for better customization to a given patient and means to ease out the process of sanction of CMRF at the level of hospital itself before implementing it across the government institutions of the state and country at large. This replicable process can be adopted by many other states and the central government in future. This would also boost many of the indigenous startup companies for research and development, bulk manufacturing of advanced prosthesis thereby decreasing the cost of existing prosthesis and imports.
Conclusion
Amputees require adequate rehabilitation for leading an independent and useful life. Paucity of institutional support and monitory challenges keep them away from advanced artificial limbs. State-sponsored, institute-based supply of advanced artificial limbs at free of cost to the beneficiaries is a replicable and feasible option for rehabilitation of amputees with an appropriate prosthesis at the lowest possible price incurred by the state. This process has not only served the purpose of effective rehabilitation but also has saved the public money to serve more subjects.
Footnotes
Acknowledgements
The authors would like to thank our beloved departmental colleagues, administrative, billing and all the supportive staff for their kind help in this endeavor. We sincerely thank the Government of Telangana for providing an opportunity to serve the needy in the best possible way.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.