
Abstract
Background:
Positive adjustments to amputation and an artificial limb play important roles in the rehabilitation process.
Objectives:
To study the different facets of adjustments to amputation and an artificial limb in lower limb amputees and to assess the possible role of different background and amputation-related factors that could potentially influence these adjustments.
Study design:
Cross-sectional.
Methods:
Adult unilateral and non-congenital lower limb amputees (n = 368) met the inclusion/exclusion criteria. Face-to-face interviews were conducted using structured questionnaires including patient’s background, amputation and the Trinity Amputation and Prosthesis Experience Scales.
Results:
Amputees were on average satisfied with the functioning of the prosthesis, moderately psychosocially adjusted and not restricted in performing functional and social activities, except for athletic activities. Age, employment, daily use of prosthesis and assistive device use were the most important factors associated with adjustments to amputation and prosthesis, followed by gender, co-morbidity and amputation level.
Conclusions:
Evaluation of employment status and measures to curb unemployment through vocational rehabilitation and providing assistance for placement should be intrinsic to the rehabilitation programme. Future studies are envisaged to understand the underlying factors determining the extent of daily use of prosthesis and the reasons for the use of assistive devices by the amputees.
Clinical relevance
Proper appraisal and measures to alleviate employment and co-morbidity, related issues, routine evaluation of daily use of prosthesis and providing appropriate gait training might facilitate immediate and long-term adjustment.
Background
Adjustments to amputation and an artificial limb are intricate physical, psychological and social processes. 1 Physically, the body has to adjust to amputation setback, phantom limb pain, achieve functional abilities and his/her functional expectations with the artificial limb to be able to perform activities of daily living, resume work and other activities with respect to his/her roles and responsibilities and expectations; psychologically, the individuals have to cope with the amputation and its consequences, accept the changed body image and also get used to the physical and mechanical features of the artificial limb; and socially, the individuals have to perform social roles and maintain social contacts. Thus, adjustments to amputation and an artificial limb encompass the physical functioning, psychosocial functioning and satisfaction with the artificial limb 2 at an individual level as well as in the society with respect to the physical change brought about by amputation and the challenges posed by the changed state.
Adjustments to amputation and an artificial limb are important for functioning, quality of life, 2 and to enable social participation of amputees. Adjustment has mostly been implied as limiting and negative consequence after amputation. Horgan and Maclachlan 3 reviewed psychological adjustment in amputees in terms of depressive and anxious reactions, body-image anxiety, social functioning and social discomfort and sense of self and identity. However, Gallagher and MacLachlan 4 explored the perception of amputees about their amputated leg and their perception whether something good had emerged out of their amputation, and they found that almost half of the people thought positively about their amputation. It is to be noted that the study population mainly comprised young and traumatic amputees.
The prominent self-reported scales that are being used to study functioning with prosthesis and assessment of prosthesis are Prosthesis Evaluation Questionnaire (PEQ) 5 and Trinity Amputation and Prosthesis Experience Scales (TAPES). 6 Unwin et al. 7 analysed the influence of several demographic and amputation variables (age, gender, level and cause of amputation and intensity of phantom pain) on the positive adjustment to amputation and an artificial limb as measured by positive mood subscale of Positive and Negative Affect Scale (PANAS) 8 and general adjustment subscale of TAPES 6 and found no association between these variables.
There is a dearth of studies focussing on adjustments to amputation and an artificial limb that would indicate the acceptance of artificial limb by the amputees and their performance with it, as well as the different factors that play a role in the adjustment process. Considering the vital role of positive adjustments to amputation and an artificial limb in enabling the full participation of amputees in the society and limited information available about the influence of socio-demographic, medical and amputation-related factors on these adjustments, we aim to study first the different facets of adjustments to amputation and an artificial limb in amputees and second the role of different background and amputation-related factors that could potentially influence these. Although, the study population has been derived from India, the study results would provide insights about the adjustments to amputation and an artificial limb in general and more specifically would be of special relevance for developing countries and other countries with similar socio-contextual situation.
Methods
Participants
The study population consisted of a cross section of lower limb amputees aged 18 years and above from a limb fitting centre and a rehabilitation centre based in Mumbai and four limb fitting camps in and around Mumbai.
The Institutional Review Board of a co-author’s institute approved the study. The purpose of this study was explained to the participants, and informed signed consent was requested. Face-to-face interviews were conducted by three trained interviewers. In total, there were 622 potential participants: 360 (58%) from limb fitting centre, 99 (16%) from rehabilitation centre and 163 (26%) from camps. Out of this, participants were primarily excluded because of non-willingness to participate (8), hearing or speech impairment (4), mental incapacities (3) and other reasons (2), and additionally, amputees who were undergoing limb fitting and gait training were not included in this study. Thus, a cross section of unilateral and non-congenital amputees who were using an artificial limb was considered for this study keeping in view the objective of the study, resulting in a total of 368 amputees.
Measures
Data were collected using structured questionnaires, which included patient’s background (socio-demographic and medical information), amputation, artificial limb and assistive device use–related information, and TAPES. 6
TAPES is a multidimensional questionnaire assessing adjustment to amputation and prosthesis use developed specifically for use with lower limb amputees. TAPES consists of three psychosocial adjustment subscales (general adjustment, social adjustment and adjustment to limitation), three activity restriction subscales (functional, athletic and social restriction) and three prosthesis satisfaction subscales (functional, aesthetic and weight satisfaction). The higher score of these subscales indicates better psychosocial adjustment, increased restriction in performing activities and greater satisfaction with artificial limb, respectively.
Statistical analysis
Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS version 15). 9 Descriptive statistics were performed for background and amputation characteristics and TAPES subscales. Cronbach’s alpha coefficients 10 were calculated for the TAPES subscales to assess internal consistency.
Stepwise regression analyses 11 were performed with TAPES subscales as dependent variables and background (sex, age, marital, education and employment status and co-morbidity) and amputation, prosthesis and assistive device use–related variables (time with prosthesis; cause, level and side of amputation; daily prosthesis use; residual stump pain; phantom limb sensation and phantom limb pain; stump skin problem and use of canes or crutches as assistive devices) as independent variables. Binary coding was done for the categorical variables. 12 The regression procedure resulted in a parsimonious model based only on the factors that achieved statistical significance (p < 0.05). Stepwise regression was used due to the exploratory nature of the model.
Results
The majority of the amputees were men (88%), and the mean age was 43 years. On average, they had an amputation since 13 years, and trauma was the main cause of amputation. Over half of the amputees were employed (59%), and quite a significant percentage of amputees used assistive devices (40.8%), such as canes and crutches (Table 1).
Study population characteristics.
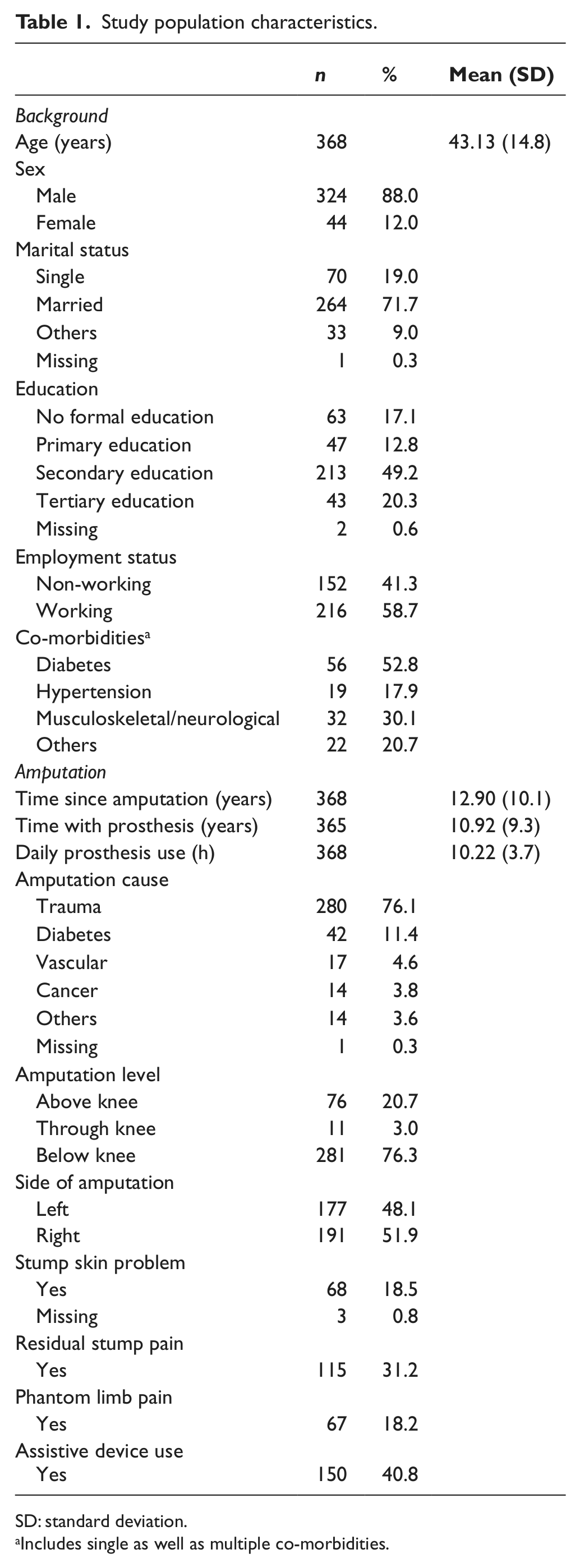
SD: standard deviation.
Includes single as well as multiple co-morbidities.
TAPES 6 is a validated instrument with three scales (prosthetic satisfaction, psychosocial adjustment and activity restriction). Each scale has three subscales. All the subscales of TAPES had an acceptable Cronbach’s alpha (> 0.7), except for aesthetic satisfaction and general adjustment subscales (Table 2). Therefore, these were excluded from the regression analyses.
Descriptive statistics for TAPES subscales.
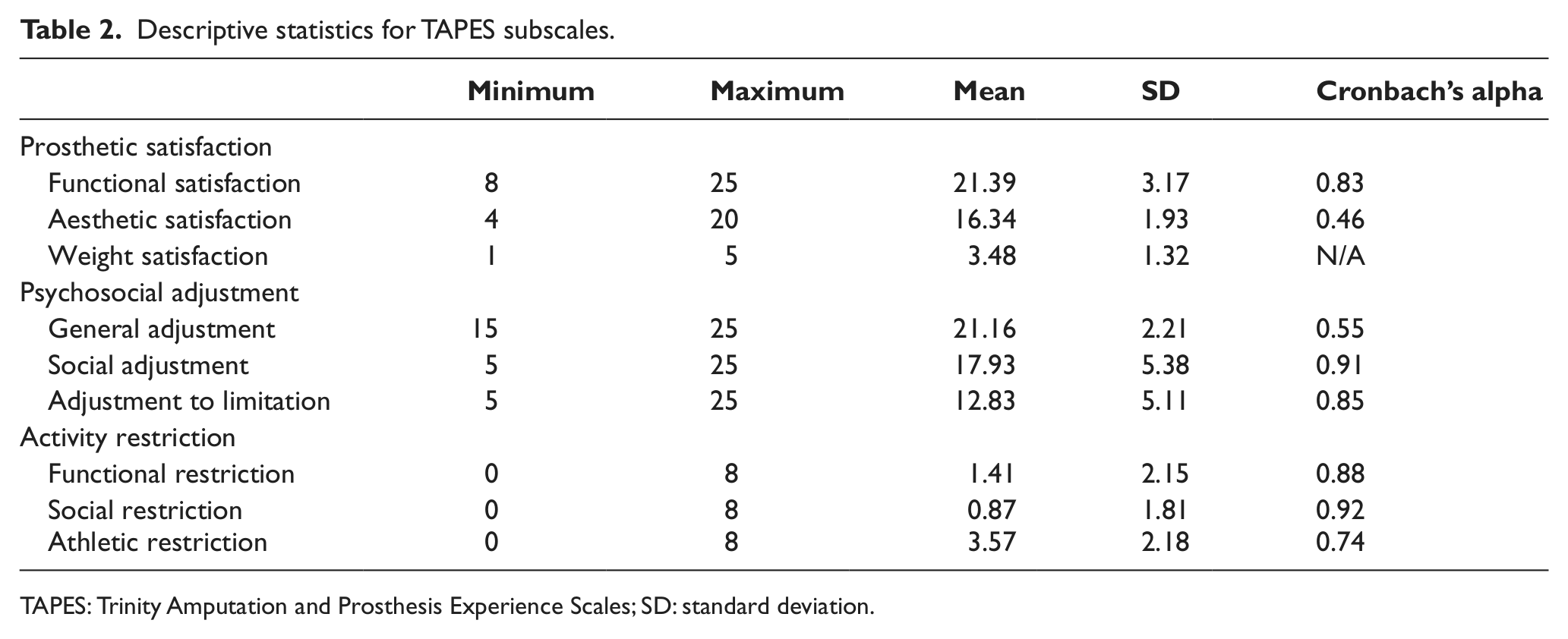
TAPES: Trinity Amputation and Prosthesis Experience Scales; SD: standard deviation.
The scores of the TAPES subscales indicated that amputees were on average satisfied with the way they could function with the prosthesis, were moderately psychosocially adjusted, as they scored relatively less on social adjustment and adjustment to limitation subscales of TAPES, and did not show much restriction in performing functional and social activities, except for athletic activities. The scores of social activity restriction subscale demonstrated that the amputees did not feel socially restricted (Table 2).
Functional satisfaction
The regression analyses results revealed that not using assistive devices such as canes and crutches, not having phantom limb pain and more hours of prosthesis use on a daily basis were associated with being more functionally satisfied with the prosthesis (Table 3).
Summary of stepwise regression results for TAPES.
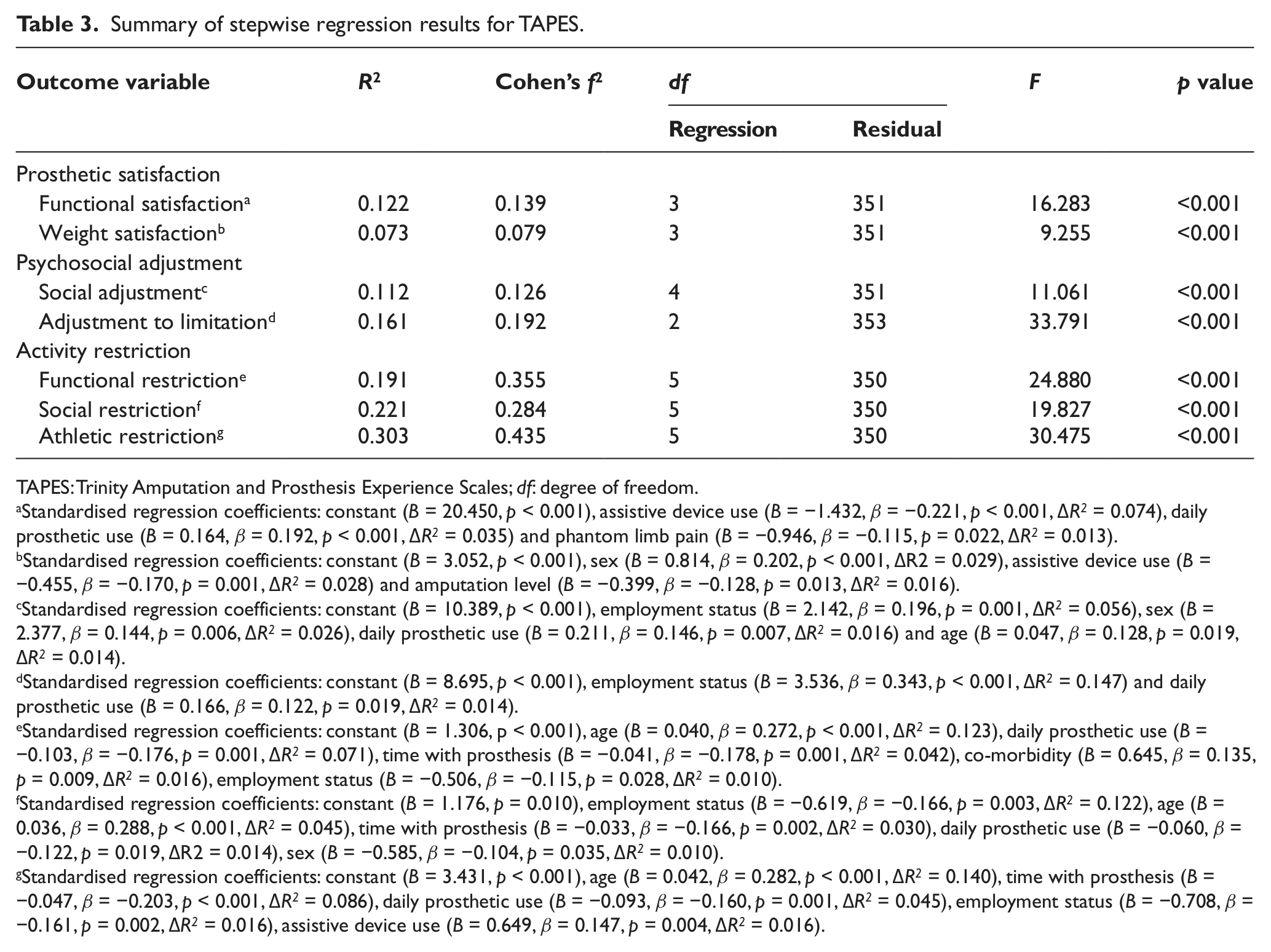
TAPES: Trinity Amputation and Prosthesis Experience Scales; df: degree of freedom.
Standardised regression coefficients: constant (B = 20.450, p < 0.001), assistive device use (B = −1.432, β = −0.221, p < 0.001, ΔR2 = 0.074), daily prosthetic use (B = 0.164, β = 0.192, p < 0.001, ΔR2 = 0.035) and phantom limb pain (B = −0.946, β = −0.115, p = 0.022, ΔR2 = 0.013).
Standardised regression coefficients: constant (B = 3.052, p < 0.001), sex (B = 0.814, β = 0.202, p < 0.001, ΔR2 = 0.029), assistive device use (B = −0.455, β = −0.170, p = 0.001, ΔR2 = 0.028) and amputation level (B = −0.399, β = −0.128, p = 0.013, ΔR2 = 0.016).
Standardised regression coefficients: constant (B = 10.389, p < 0.001), employment status (B = 2.142, β = 0.196, p = 0.001, ΔR2 = 0.056), sex (B = 2.377, β = 0.144, p = 0.006, ΔR2 = 0.026), daily prosthetic use (B = 0.211, β = 0.146, p = 0.007, ΔR2 = 0.016) and age (B = 0.047, β = 0.128, p = 0.019, ΔR2 = 0.014).
Standardised regression coefficients: constant (B = 8.695, p < 0.001), employment status (B = 3.536, β = 0.343, p < 0.001, ΔR2 = 0.147) and daily prosthetic use (B = 0.166, β = 0.122, p = 0.019, ΔR2 = 0.014).
Standardised regression coefficients: constant (B = 1.306, p < 0.001), age (B = 0.040, β = 0.272, p < 0.001, ΔR2 = 0.123), daily prosthetic use (B = −0.103, β = −0.176, p = 0.001, ΔR2 = 0.071), time with prosthesis (B = −0.041, β = −0.178, p = 0.001, ΔR2 = 0.042), co-morbidity (B = 0.645, β = 0.135, p = 0.009, ΔR2 = 0.016), employment status (B = −0.506, β = −0.115, p = 0.028, ΔR2 = 0.010).
Standardised regression coefficients: constant (B = 1.176, p = 0.010), employment status (B = −0.619, β = −0.166, p = 0.003, ΔR2 = 0.122), age (B = 0.036, β = 0.288, p < 0.001, ΔR2 = 0.045), time with prosthesis (B = −0.033, β = −0.166, p = 0.002, ΔR2 = 0.030), daily prosthetic use (B = −0.060, β = −0.122, p = 0.019, ΔR2 = 0.014), sex (B = −0.585, β = −0.104, p = 0.035, ΔR2 = 0.010).
Standardised regression coefficients: constant (B = 3.431, p < 0.001), age (B = 0.042, β = 0.282, p < 0.001, ΔR2 = 0.140), time with prosthesis (B = −0.047, β = −0.203, p < 0.001, ΔR2 = 0.086), daily prosthetic use (B = −0.093, β = −0.160, p = 0.001, ΔR2 = 0.045), employment status (B = −0.708, β = −0.161, p = 0.002, ΔR2 = 0.016), assistive device use (B = 0.649, β = 0.147, p = 0.004, ΔR2 = 0.016).
Psychosocial adjustment
Being employed and more hours of prosthesis use on a daily basis were associated with being more socially adjusted as well as being more adjusted to limitation. Being male and older were associated with being more socially adjusted (Table 3).
Activity restriction
Being younger was associated with being less functionally and socially restricted, as well as less restricted in performing athletic activity. Being employed was associated with being less functionally and socially restricted, as well as less restricted in performing athletic activity. A lower number of years with prosthesis was associated with being more functionally and socially restricted, as well as greater restriction in performing athletic activity. More hours of prosthesis use on a daily basis indicated being less functionally and socially restricted, as well as less restricted in performing athletic activity. Additionally, having co-morbidity was associated with increased functional restriction (Table 3).
Discussion
Age, employment, daily use of prosthesis and assistive device use were the most important factors associated with adjustment to amputation and prosthesis (TAPES subscales), followed by gender, co-morbidity and amputation level. Employment contributed the most in influencing adjustment to amputation and prosthesis (explained by change in variance), followed by daily prosthesis use although to a much lesser extent.
Less use of assistive devices such as canes and crutches, more use of prosthesis on a daily basis and not having phantom pain were linked to being more functionally satisfied with the prosthesis. Murray 13 also found not having pain and more use of prosthesis on a daily basis to be associated with being more functionally satisfied, although pain was not segregated into phantom pain and stump pain, as has been done in this study.
Gender, use of assistive device and amputation level were related with weight satisfaction, while Murray 13 found pain, daily prosthesis use and time with prosthesis to be contributing to it. However, the study by Murray did not include background, amputation- and assistive device use–related factors in the analyses as has been done in this study. In general, females are not as strong as males to carry the extra weight of the prosthesis, and this could be a reason that being female was related to less weight satisfaction. Also, people who found their prosthesis to be heavy, which could be related to the residual muscle power, might be using assistive device as a means to carry their limb, and therefore, use of assistive device was linked to weight satisfaction. Higher level of amputation also meant less satisfaction with the weight of the prosthesis, which could be because of the additional weight of more components, such as thigh socket and more reinforcement lining for extra strength and prosthetic joints being involved in case of higher level amputees.
The above results indicate that it is important to evaluate the functional satisfaction with the prosthesis during the rehabilitation programme, and prosthesis prescription should also consider prosthesis weight and attributes of other prosthetic components to suit the individual requirements. Also, if amputees are functionally satisfied, then they would not require other assistive devices, as they would have confidence in the prosthesis. In certain situations, for example, frail-elderly and weakness due to diseased condition, the use of assistive device will support independency. However, considering the average age of this study population and the traumatic nature of amputation, it seems logical to believe that perhaps prosthetic prescription or the features of different prosthetic components, for example, weight and functionality, might not be up to the level to suit the individual requirements. Probably, poor prosthetic prescription will be related to the resources available with the rehabilitation centres and the economic boundaries within which the centres have to operate, which also might be influencing the choices in prosthetic prescription.
Unemployed amputees were found to be less socially adjusted and less adjusted to the limitations, functionally and socially restricted and also restricted in performing athletic activities. It might be that people who are adjusted to amputation and prosthesis have more chances of being employed. It could also be that economic independency due to employment status makes people more psychosocially adjusted and they tend to be more physically active. Commuting to work and performing the job would be requiring of amputees to perform some physical activity as compared to a non-working person; therefore, the underlying motivation factor cannot be undermined, and the socio-economic status would be playing an important role here. Future research is required to unravel the relation (what affects what) between employment and psychosocial adjustment.
Age, employment and daily prosthesis use had an influence on activity restriction. According to a study by Raichle et al., 14 being employed was found to be a significant predictor of prosthesis use on a daily basis. This is especially relevant with context to developing countries where there might not be adequate social and financial support available for conditions like disability and unemployment. Compounded with it, amputees would also have obligations and financial responsibilities towards family. Generally, studies do not evaluate the influence of employment status on the functioning of amputees. It is recommended for studies to include this variable and analyse its influence.
Women were less socially adjusted as compared to males. This could have a link with the social system and mindset of the people. Perhaps, there would be a stigma 15 attached with disability in general and more so when it comes to females. 15 There is a greater gender inequality when compared with many countries (ranked 129 in 2011 as per United Nations Development Programme (UNDP) report). 16 Reaction of other people in the society might be shaping up the notion of female amputees, and therefore, they might be feeling less socially adjusted as compared to their male counterparts. This finding has an implication for the rehabilitation programme especially while treating female amputees. Psychologists might play an important role and take appropriate measures to alleviate such feelings and predispositions from the female amputees.
Phantom limb pain or residual stump pain was found not to be important for adjustment to amputation and an artificial limb. Phantom pain had a very small influence on prosthesis satisfaction scale and did not have influence on psychosocial adjustment and activity restriction scales. Similarly, Desmond et al. 17 did not find phantom pain to influence the psychosocial adjustment scale, and also its link to other TAPES scales was not assessed in this study.
Strengths
There are relatively few studies evaluating psychosocial adjustment to amputation and prosthesis, more so in developing countries. This study involves a large sample size from three different sources and gives a profile of the amputee’s psychosocial adjustment to amputation and prosthesis and association of factors possibly influencing adjustment to amputation and prosthesis, a relatively untouched area of study with respect to amputees’ rehabilitation. With the rising amputation rates in the developing countries because of accidents and predisposing health conditions, which lead to amputation, it becomes imperative to know the potentially influencing factors contributing to the adjustment process, so as to consider these during the rehabilitation of amputees.
Limitations
The study design being cross-sectional poses certain limitations with respect to the relationships between the dependent and the independent variables. It only provides a single time assessment of patients and does not address how variables interrelate over time. Therefore, it is possible that the relationship might be different if patients would be evaluated over a time period. Nevertheless, the study results could be considered to be indicative of potential factors influencing adjustments to amputation and an artificial limb.
The study population was not derived from a primary source, such as hospital; therefore, the possibility that the study population comprises those people who are motivated, interested in their health and well-being and who can access the rehabilitation centre/limb fitting centre and therefore visiting the limb fitting centre for procuring leg cannot be totally disregarded. Longitudinal study with study sample derived from the primary source is envisaged as it will provide in-depth knowledge of the adjustment to amputation and prosthesis over time. Since the amputation-related questionnaires were self-reported, the chance of recall bias cannot be totally excluded.
Approximately one-tenth of the study population was females. Low representation of females has also been observed elsewhere. 18 It is highly uncertain that such a difference is just a matter of chance, as the study population was recruited from three different types of sources. Rather, it gives an indication about the amputee epidemiology in India. With the ageing population and the increasing incidence of diseases that lead to amputation, as well as the growing population and infrastructural constraints posed by developing economy, which poses more risk of traumatic accidents, it becomes important to investigate the adjustment to amputation and prosthesis more vividly in females as well. This study findings indicate that females were found to be less socially adjusted.
Conclusion
To conclude, employment, daily prosthesis use, age, assistive device use, and to a lesser extent, gender and amputation level are the most important factors contributing to adjustment to amputation and prosthesis. Except for age, gender and level of amputation, the other factors predominantly contributing the most to adjustment to amputation and prosthesis are addressable. Employment status evaluation and appropriate vocational rehabilitation should be incorporated as a routine practice in the rehabilitation protocol. Furthermore, measures to facilitate employment for amputees by co-operating with employment agencies or organisations should be considered. Female amputees are possibly more at risk, and therefore, rehabilitation professionals need to consider this while planning the frequency of follow-up and take pertinent actions as per the follow-up findings. Future studies are envisaged to understand the underlying factors contributing to the extent of daily use of prosthesis and the reasons for the use of assistive devices, like canes and crutches by amputees. Addressing these issues would be helpful in ensuring a higher level of adjustment to amputation and prosthesis by the amputees.
Footnotes
Conflict of interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.