
Abstract
Objective:
To analyze sports participation of Dutch lower limb amputees and factors influencing sports participation.
Study design:
A cross-sectional survey was performed. Dutch lower limb amputees (N = 2039) were invited to participate in a postal survey addressing personal and amputation characteristics, physical limitations, sports participation, skin problems, and prosthesis use. Only data concerning personal and amputation characteristics together with the data concerning sports participation were used for this study.
Results:
Of the 816 questionnaires received, 780 were suitable for statistical analysis. The mean age of the participants was 59.6 years (SD 14.8), 62% were men and 27% of the amputations was due to vascular diseases or diabetes. Only 15% of all respondents participate in sports at least 5 hours a month. Smoking (odds ratio: 0.55), an age older than 60 (odds ratio: 0.97 per year), and a vascular cause of amputation (odds ratio: 0.42) were negatively associated with sports participation.
Conclusion:
Less than 15% of the Dutch lower limb amputees participate in sports at least 5 hours per month. Older age, smoking and a vascular cause of amputation have a negative influence on the sports participation of these individuals.
Clinical relevance
Actual sports participation rate of lower limb amputees is much lower than earlier predicted. Older lower limb amputees with a poor health are less likely to participate in sports; therefore rehabilitation professionals working with this patient group should try to promote a healthier living style.
Introduction
In the near future, the number of lower limb amputees (LLA) is most likely to increase due to an increase in age and an increased incidence of diabetes mellitus and cardiovascular conditions. 1 Regular participation in sports and physical activity (PA) improves physical functioning and overall quality of life in LLA. 2 After a physical training program, cardiopulmonary function, physical fitness,3,4 walking speed, and walking distance 5 as well as overall functioning with the prosthesis6,7 improve. Additionally, LLA who participate in sports (athletes) also experience an improvement in psychosocial functioning. Athletes mention that sports participation helps them to increase the number of social contacts and to cope better with their amputation, and it also gives them a higher self-esteem.7,8 However, sport participation rates of LLA have scarcely been investigated. 2 Most of the studies addressing this topic are characterized by selection bias9–12 and/or do not mention criteria to differentiate between athletes and nonathletes. Consequently, large differences exist in reported sports participation rates of LLA. For example, in the Netherlands, sports participation rates of LLA range from 32% to 39%,9,10 while in the United States this rate is 60%. 13
The literature studying the factors that influence sports participation of LLA is scarce and contradictory. 2 Some studies identify older age,12–16 a proximal level of amputation,6,14,15,17 and a vascular cause of amputation 13 as factors that have a negative influence on sports participation of LLA, while other studies either do not identify those factors or identify other factors, such as sports participation prior to amputation 10 or gender. 16 Selection bias may have caused these contradictory results. Identifying the factors that influence participation in sports or PA of LLA may help rehabilitation professionals to predict more accurately the odds of such an individual participating in sports. Consequently, our aim is to analyze sports participation rate of LLA and factors influencing sports participation.
Methods
Data used in this study originated from a larger database used in previous studies.18,19 The aim of those studies was to identify skin problems, to identify determinants of skin problems of the stump in LLA, and to analyze the influence of skin problems on functioning in daily life. Detailed information regarding the sampling procedure can be found in those studies.18,19 In short, Dutch LLA ≥ 18 years old were invited, either via an orthopedic workshop (Orthopedische Instrument Makerij (OIM)) or via the National Society of Amputees (Landelijke Vereniging van Geamputeerden (LVvG)), to participate in this study. If they agreed, they had to return their signed informed consent together with their address details. Afterward they received an envelope containing the questionnaire, which they were asked to answer and then return. If an incomplete set of data was received, the sender was contacted in order to remedy the issue. No formal permission on behalf of the local medical ethical committee was needed to conduct this study. 20
For the purpose of this study, the answers to two questions, not previously investigated, together with personal characteristics and amputation characteristics were analyzed. These questions were related to sports participation and were formulated as follows: “Did you participate in sports in the last month? If so, how many hours did you participate in sports last month? Please choose one of the following: less than 1 hour, between 1 and 5 hours, more than 5 hours” and “For what sports did you use a prosthesis and how many hours did you spend at those sports?” Participants were divided into two different groups according to their sports participation level: LLA who participated in sports more than 5 h per month (athletes) and those who participated in sports less than 5 h per month (nonathletes).
Data analysis
Statistical analyses were performed in the Statistical Package for the Social Sciences for Windows (Version 18.0.3; SPSS Inc., Chicago, IL). Possible associations between sports participation (athletes versus nonathletes) and gender, civil status, education, work status, smoking, presence of additional health problems, presence of complaints of the sound leg and etiology, and side and the level of amputation were investigated using Pearson’s chi-squared test. A t-test for independent samples was used to analyze differences in age of athletes and nonathletes. The influence of the time elapsed since the amputation and sports participation were analyzed using a Mann–Whitney test. The significance level for all tests was preset at 0.05. In order to facilitate the statistical analysis, the following variables were categorized: level of amputation into transtibial, knee disarticulation and transfemoral, and amputation etiology into vascular and nonvascular. Age was centered at 60 years. Factors that were associated with sports participation (p ≤ 0.1) were entered into a logistic regression (LR) analysis (method: backward LR).
Results
A total of 2.309 LLA, representing 25% of the possible Dutch population of LLA, were invited to participate, of which 872 agreed to complete and to return the questionnaire, while 816 actually returned the questionnaire.18,19 Eventually, the responses of 780 (34%) participants (mean age = 59.6 (standard deviation (SD) = 14.8)) were suitable for statistical analysis (Table 1). In total, 665 (85%) were nonathletes and 115 (15%) were athletes. No significant differences were found between nonathletes and athletes regarding gender, presence of complaints at the sound leg, presence of bilateral amputation, or the level of amputation. Age, work status, and the reason of amputation significantly associated (p < 0.001) with participation in sports for athletes. Age centered at 60 years, civil status, cause of amputation, months since amputation, additional health problems, work status, and smoking were entered in the regression analysis. Individuals older than 60 years, with an amputation due to vascular etiology, and who are smoking were less likely to be athletes (Table 2).
Overview of the characteristics of the participants divided into nonathletes and athletes.
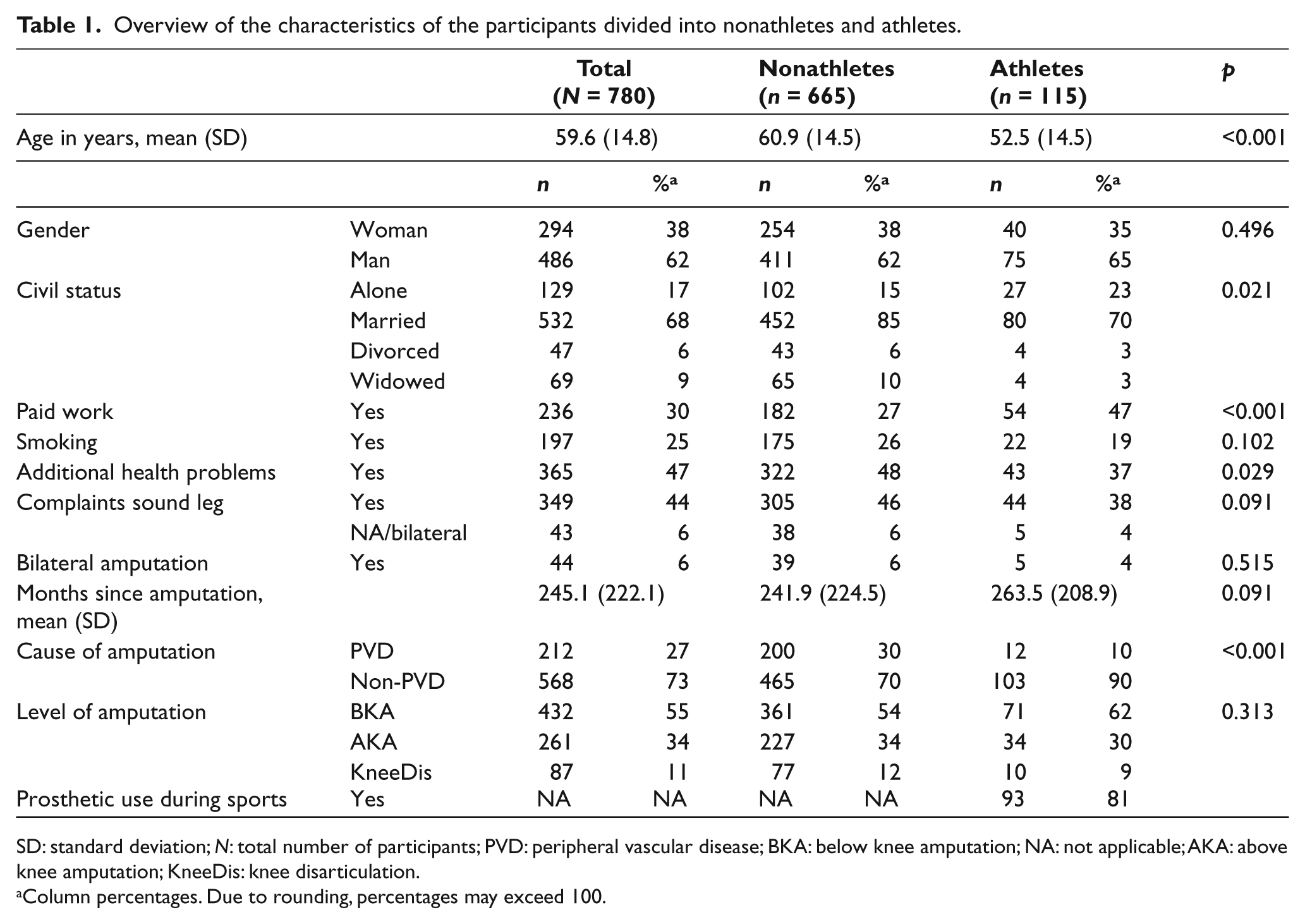
SD: standard deviation; N: total number of participants; PVD: peripheral vascular disease; BKA: below knee amputation; NA: not applicable; AKA: above knee amputation; KneeDis: knee disarticulation.
Column percentages. Due to rounding, percentages may exceed 100.
Results of LR analysis (backward LR) to statistically predict sports participation (>5 h per month) in lower limb amputees.
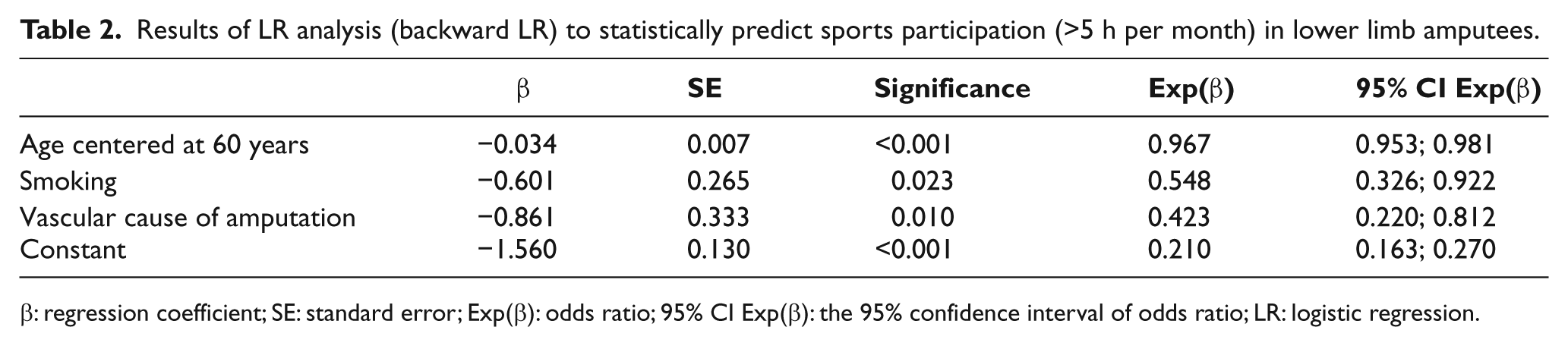
β: regression coefficient; SE: standard error; Exp(β): odds ratio; 95% CI Exp(β): the 95% confidence interval of odds ratio; LR: logistic regression.
Of the athletes, 93 (81%) used their prosthesis during sports. LLA used their prosthesis for participating in 22 different sports. Most practiced sports with a prosthesis was cycling (37%) followed closely by fitness (30%) and walking (12%).
Discussion
Of the 780 LLA who participated in this study, only 15% participate in sports for more than 5 h a month. An age of above 60 years, smoking, and a vascular cause of amputation were negatively associated with sports participation.
Previous research in a small national 9 or a regional sample 10 of Dutch LLA found a sports participation rate of 32% and 39%, operationalized as ≥1 h per week. Our sports participation rate, based on the analysis of a national sample of Dutch LLA, was considerably less. However, a difference in the definitions of sports participation is present between this study and the previous ones. Therefore, the group of athletes, according to this study (>5 h per month), may exclude individuals who were considered athletes according to the definition used in the previous studies (≥4 h per month).9,10 Our results are in even larger contrast to those of American LLA (60%). 2
According to recent studies, between 37% and 56% of the general Dutch population participates in sports at least ≥1 h per week,21–24 hence more people in the general population are active than LLA. This statement is also supported by previous findings stating that individuals with physical disabilities, including LLA, achieve up to 40% of the PA level of the general, able-bodied population. 12 Additionally, this large difference between the participation rate of general population and that of LLA may imply that the current strategies to advocate sports participation of LLA are ineffective and that the factors that promote or prevent sports participation of LLA are being inadequately addressed. Future research on this topic is recommended as its results can be used to develop programs that will ultimately lead to an increase in sports participation of the LLA.
According to our analysis, factors usually associated with poor health, namely, an age above 60 years, smoking, and an amputation due to vascular etiology, have a negative association with sports participation of LLA. Age above 60 years was also identified by others as a predictor for not participating in sports of LLA12–16 as well as for the general population.25,26 The negative association between an amputation due to vascular etiology and sports participation of LLA supports previous results. 13 Similar to earlier studies,25,26 our univariate analysis identified an association between civil and working status and sports participation of LLA. The working status, namely, having a paid job, usually relates to a better economic status. The influence of the marital status, being married or having a partner, may imply that family plays an important role in the participation in sports of LLA. However, in the logistic regression analysis, civil and working status did not predict sports participation. Several studies identified that a more proximal level of amputation has a negative impact on the sports participation of LLA.6,14,15,17 Additionally, it was identified that the energy expenditure during walking is directly proportional to the level of amputation.27,28 Contrary to these statements and in agreement with others,10,11,13 our analysis did not identify a significant association between the level of amputation and the participation in sports of LLA. The fact that 81% of the athletes used their prosthesis during sports comes to support earlier findings that mention that the use of prosthesis is an important element of the rehabilitation and social reintegration of LLA.29,30
Strengths and limitations
The response rate in our study was rather low (34%), which may have led to selection bias, but the rate is in agreement with that of a postal survey. 31 The extent of selection bias cannot be analyzed in detail because we do not have access to the characteristics of the source population.18,19 One form of bias is clear: while the majority of amputations are performed for a vascular problem, only a small amount of the participants had an amputation due to a vascular problem. Next to this, the participants in our survey were relatively young compared with the general population of LLA. 32 LLA who participated in this study were not focused on sports participation; we, therefore, believe that selection bias (of sports enthusiasts) that may occur in studies that specifically focus on sports participation is not present. Our estimate of sports participation rate of LLA is therefore probably lower than that of others. Using a clear cutoff point to differentiate between nonathletes and athletes makes our results easier to compare with the results from others.
Due to limitations of the instrument used to gather data, it was impossible to calculate the exact number of hours per week each LLA participated in sports. Because it was our intention to include only those persons who are active at least 1 h per week, similar to previous research, 10 we decided upon the use of a cutoff point of ≥5 h per month.
Conclusion
Sports participation rate of LLA is only 15%. Age above 60 years, smoking, and a vascular cause of amputation are negatively associated with sports participation.
Footnotes
Conflict of interest
No party having a direct interest in the results of the research supporting this article has or will confer a benefit on us or on any organization with which we are associated. The authors have no known conflict of interests.
Funding
No sources of funding were used to assist in the preparation of this article.