
Abstract
Background
Medial knee osteoarthritis can contribute to pain and stiffness, interfere with balance and limit functional activities of daily living. Unloader knee orthosis or lateral wedged insoles are current conservative approaches used to treat these conditions. The aim of this study was to identify and compare the effects of them on the balance parameters.
Methods
66 subjects with mild to moderate medial knee osteoarthritis were randomly assigned to wear unloader knee brace or full-length 6° lateral wedge insole. Primary outcome balance parameters were stability %, path length and average velocity of center of pressure and mobility score which were investigated by HUMAC® Balance and Tilt system. Secondary outcome measures were knee function score using Knee Injury and Osteoarthritis Outcome Score scale. Assessment was performed at baseline and six months post orthotic intervention period.
Findings
Both orthoses improved all parameters compared to the baseline condition (p < 0.05). Unloader knee orthosis showed a significant improvement in all balance parameters compared to lateral wedged insoles (p < 0.001) except mobility scores (p = 0.527). Except activities of daily living (p = 0.752) and sports and recreational activities (p = 0.437), unloader knee orthosis had a greater effect on the pain (p = 0.002) and symptoms (p < 0.001) sub scales than lateral wedged insoles. However, quality of life sub-scale scores for insoles were more effective than the knee orthosis.
Interpretation
Unloader knee orthosis improved balance and knee function scores more than lateral wedged insole, though both orthoses produced significantly improved results compared to baseline assessment.
Introduction
The maintenance and control of balance, whether under static or dynamic conditions, is an essential requirement for physical and daily activities. Balancing is the process by which postural stability is maintained. Postural stability is the ability to maintain or control the center of mass (COM) in relation to the base of support (BOS) to prevent falls and complete desired movements. Static balance is the ability to maintain postural stability and orientation of COM over the BOS while the body is at rest. 1
Osteoarthritis (OA) is a degenerative and progressive joint disease that mainly involves weight- bearing joints such as the hip, knee and ankle. Degenerative OA of knee is one of the most common forms 2 and it has been estimated that approximately 6% of the population 30 years or older and 12% of the population aged 65 years or above have knee OA. 3 Patients with knee OA usually present with major involvement in the medial compartment characterized by joint inflammation, loss of cartilage and joint space and experience increased loads across this compartment. These contribute to pain, changes in muscle control and interferes with balance and postural control. 4 Initial therapeutical approaches in the management of knee OA include non-surgical treatments such as physiotherapy, pharmacologic therapy or use of orthoses. 5 Common orthoses used for OA are wedged insoles, knee sleeves and corrective realigning knee (unloader) braces. The goal of lateral wedged insoles (LWI) for medial compartment knee OA is to increase foot pronation and to shift the center of pressure (COP) of the foot lateral to shorten the moment arm between the ground reaction force and the knee joint center, thereby reducing medial compartment loading. 6 The results of a previous study show that LWI do not have an immediate effect on balance parameters of individuals diagnosed with medial OA. However, after using LWI for four weeks, a reduction in postural sway (displacement and velocity) of these individuals in medio-lateral direction was observed, which can be indicative of improved balance. 7 Corrective realigning orthoses are modified for patients with knee OA by changing the orientation of the hinge in the frontal plane to create a valgus or varus force, with the goal of reducing loading and symptoms of uni-compartmental knee OA. There are numerous models of realigning knee OA orthoses. In general, the degree of correction is adjusted by either single or double upright hinges, dynamic force straps, or adjustment of the femoral condyle pads. 7 However, orthoses and insoles are likely underused, possibly due to lack of knowledge of providers or poor response and compliance of patients. Although there may not be evidence for disease modification, results of several clinical trials that used realignment orthosis have shown pain reduction in patients with uni-compartmental knee OA.8,9
From the literature survey, it was observed that most of the studies on unloader knee orthosis (UKO) have evaluated its effect on gait, pain, muscle action, knee adduction moment and joint loading.9,10 There are very few studies on effect of static balance in knee OA using unloading knee orthoses. Studies evaluating static balance using balance machine or instrumentation are scarce; mostly the investigators have used questionnaires, self-report or balance scales.3,11 In addition, there are conflicting results among studies which compared between knee orthosis and LWI. Studies have also questioned the clinical significance of improvements in postural control with a brace, while others questioned on small improvements that were observed in an eyes-open, stable surface, single-leg stance task.10,12 Therefore the aim of this study was to compare the efficacy of UKO and LWI on static balance in patients with knee OA. It was hypothesized that there would be a significant difference in the static balance between these two orthotic conditions.
Methods
Subject characteristics
66 subjects with symptomatic knee osteoarthritis reported in clinical out-patient department, underwent radiological evaluation combined with Knee Injury and Osteoarthritis Outcome Score (KOOS) scale to diagnose knee OA have participated in the study. It included subjects of either sex between 40–58 years of age with knee OA of medial compartment and severity of grade II to grade III by the Kellgren-Lawrence Grading Scale. 13 The Knee OA was bilateral in 37 (56%) and unilateral in 29 (44%) patients. The subjects with any neuromuscular problems, previous surgical records of the knee, injection of corticosteroids or use of foot orthoses for past 6 months or use of any assistive devices while walking were excluded.
Description of orthoses
The unloader knee orthosis (Figure 1) was fabricated on a 3-point bending mechanism to provide a medially directed force to the lateral aspect of the knee joint. The components of the knee orthosis were hard shell cuff around the thigh and shank, hinges with condylar pads and strap. Z1 Osteo-align orthotic knee joint (Zodiacal Overseas Private Limited) was used that can provide medially directed force to the lateral aspect of the knee joint through condylar pad. The knee orthosis was constructed according to the casted mould that is custom fit and adjustable. Group B subjects were fitted with full-length 6° LWI which were made from high density ethaflex sheet of appropriate thickness. LWI were custom made after taking measurements of the foot of the subject and was inserted in sports shoe of appropriate size for each subject. To maintain uniformity, all subjects in the test conditions were fitted with a pair of comfortable, identically styled lightweight sports shoes.

Custom designed unloader knee orthosis used in the study.
Study tools and instrumentation
The balance parameters were investigated by HUMAC® Balance & Tilt System (CSMi, Stoughton, MA). The KOOS is a valid, reliable and responsive self-administered knee-specific instrument which holds 42 items in 5 separately scored subscales; Pain, other Symptoms, Function in daily living (ADL), Function in Sport and Recreation (Sport/Rec), and knee-related Quality of Life (QOL) was used to assess the patients’ opinion about their knee and associated problems 14
Study procedure and protocol
In this randomized trial, the participants were allocated to either group through computer generated random allocation sequence. This was concealed by blinding the participants and investigators who recruited them. The participants divided into two groups of equal numbers (33 each); Group A and Group B. Subjects in Group A were fitted with unloader knee orthosis and Group B with LWI. The patients wore UKO or LWI for at least six hours per day for six months without interruption. The well informed written consent was obtained from the individuals prior to their participation in study. This study was approved by the ethical committee of Swami Vivekananda National Institute of Rehabilitation Training and Research, Cuttack, India. All the participants were assessed for static balance without any orthotic intervention for pre data collection. The subjects were instructed to use orthosis and the balance test was performed in three sessions with an interval of 5 min (Figure 3). The sessions were consecutive on the same day. The average of three sessions was considered for analysis. The set level is defined as the distance (degrees) to the center of the farthest target, higher level indicating higher perturbation. Hold time is the time in seconds the patient should remain on the target. Static balance parameters were accessed with a hold time of 60 s. Level III and a time period 30 s were maintained for all dynamic balance parameters during single leg stance following standard protocol of the instrument. Level III indicates moderate level of perturbation. For dynamic balance check, the subject needs to reach the targets each at 45 degrees from center consecutively at 8 different points, covering total sphere of 360 degrees. At each target points, the subject is instructed to maintain his balance with a hold time of 30 s. Tests were performed in eyes open conditions and data was recorded for bipedal static posture. The static and dynamic stability were recorded for parameters like: center of pressure (Stability, path length, average velocity) and dynamic stability. The data was collected six months after fitment of the Unloader Knee Orthosis or LWI with shoe, as the case may be. No use of medications was administered in test days. Then data was analysed and comparison was made between two readings in three different conditions.
Baseline versus UKO Baseline versus LWI UKO versus LWI
Data analysis
Raw data were exported from HUMAC® Balance & Tilt System (Figure 2) into Microsoft Excel, and final data analysis was performed in SPSS version 23.0 (SPSS Inc, Chicago, Illinios). Paired t test was used to analyse the difference between baseline, with LWI and with Unloader Knee Orthosis. The tests were applied at 95% confidence interval on α value set at 0.05. The results were taken to be significant of p-value <0.05.

HUMAC® balance & tilt system and set up.
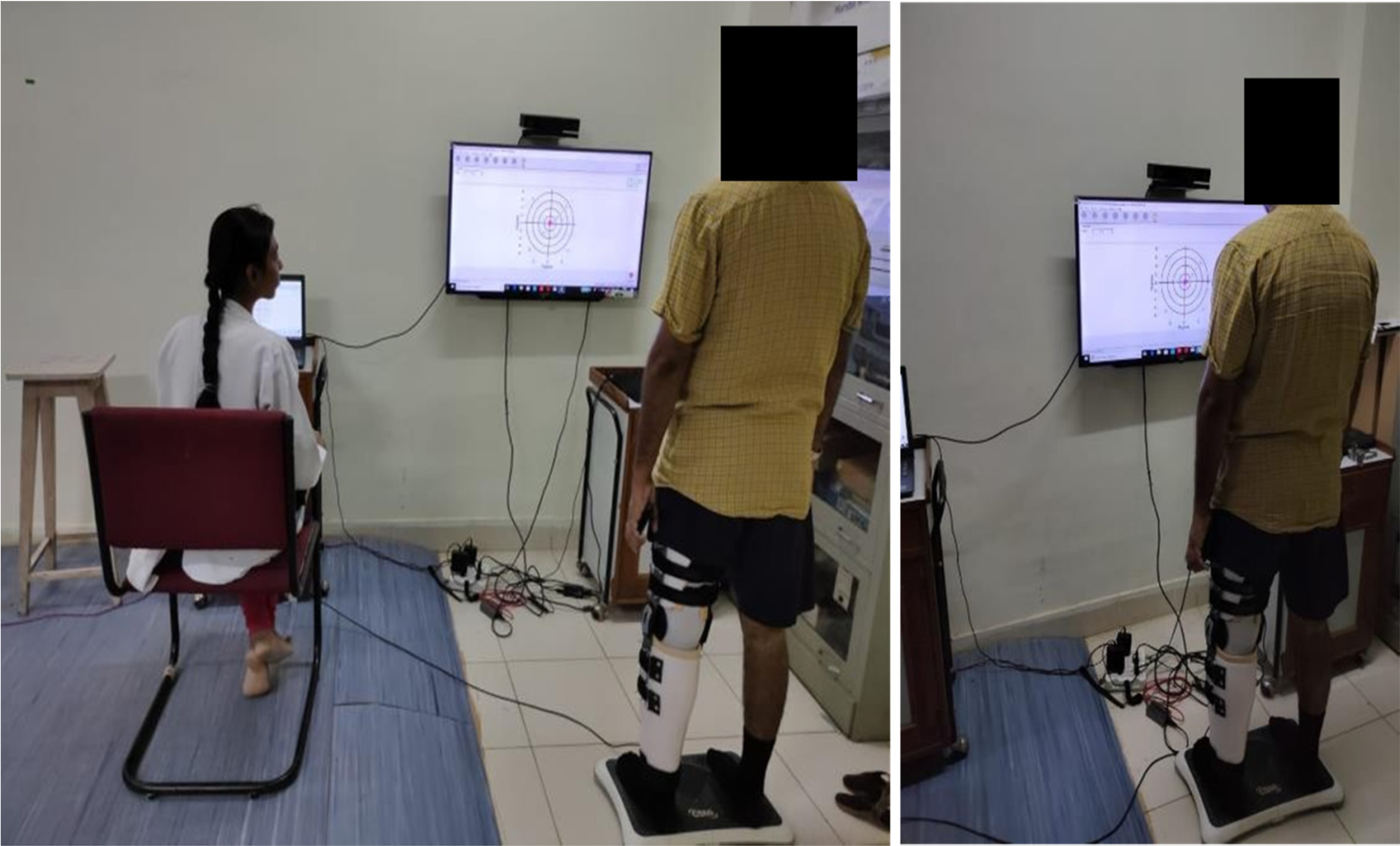
Performance of balance test.
Results
The demographic data showed that a distribution of 60% males and 40% females were evaluated for this study with average age of 49.7 years, height 1.69 m, weight 80.9 kg and BMI 26.4 kg/m2 respectively. The two groups showed non-significant differences when assessed in baseline condition (p > 0.05) as shown in Table 1. Therefore they presented with similar balance parameters to facilitate the comparison of the primary outcome measures.
Participant demographic information.
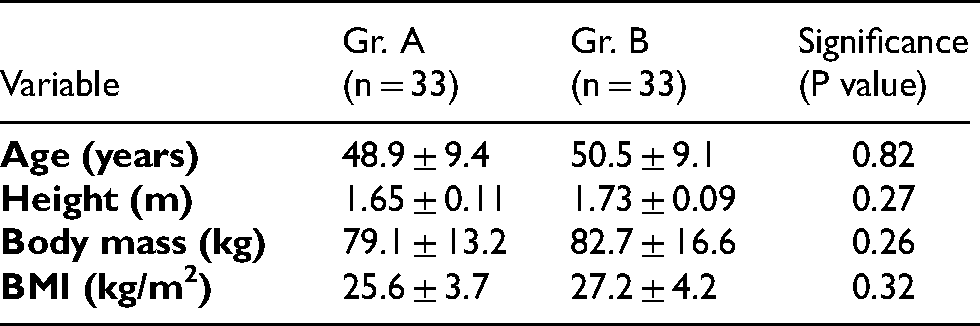
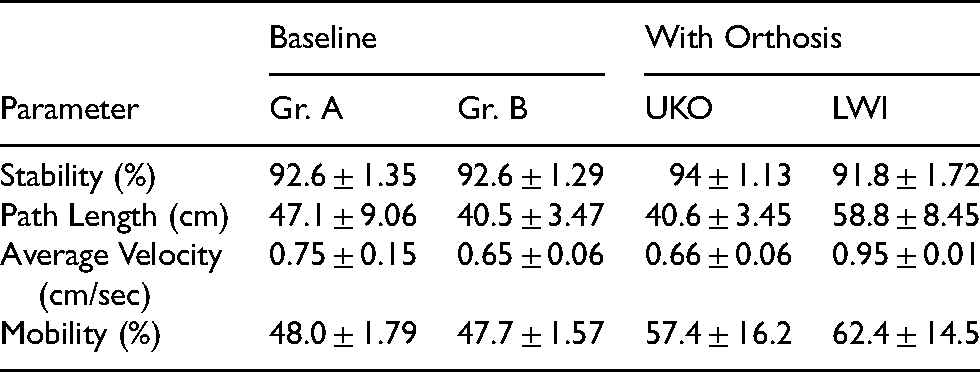
Table 2 demonstrates the comparison of different balance parameters in baseline and orthotic conditions for different groups and Table 3 shows significant differences, if any for intergroup and intragroup comparison of the mentioned parameters.
Results of comparison of different balance parameters.
Results of statistical significance in different conditions for balance parameters.
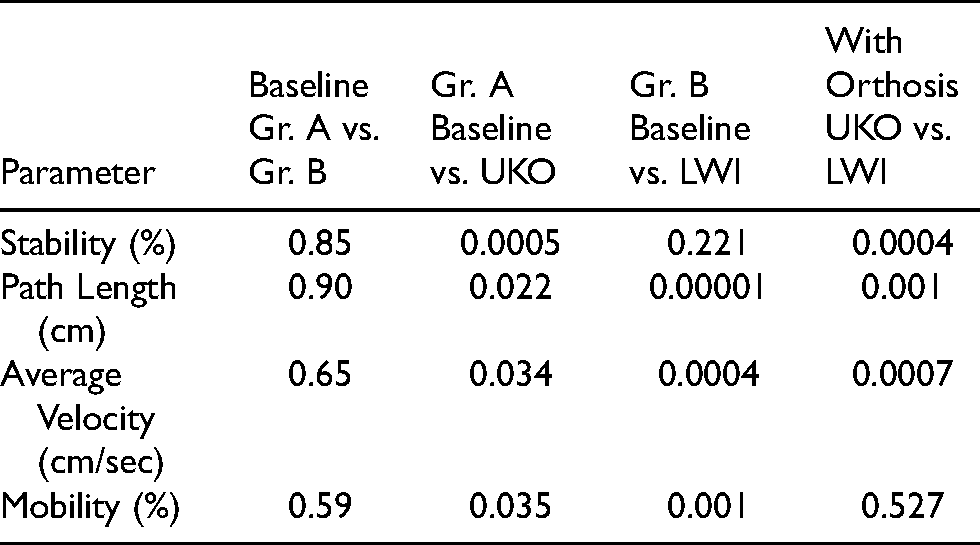
A significant difference was observed between baseline condition and UKO for all investigated parameters in favor of Unloader Knee Orthosis (Group A). While comparing baseline condition with LWI, there was a significant difference in path length, average velocity and mobility scores (p < 0.05), whereas stability score was non-significant (p > 0.05). Use of UKO in Group A subjects showed statistical significant improvement in all stability parameters except mobility scores compared to LWI in Group B.
There was significant improvement in KOOS sub-scale score for both post orthotic intervention compared to baseline (p < 0.05). Comparison of UKO and LWI demonstrated no significant differences in the ADL (P = 0.752), or sports and recreational activities (P = 0.437). The UKO had a greater effect on the pain and symptoms sub scales than the LWI. However, QOL sub-scale scores for LWI were more effective than the UKO (Table 4). P1: comparison of the means between baseline and post intervention in Group A
Comparison of the knee injury and osteoarthritis outcome score (KOOS).

P2: comparison of the means between baseline and post intervention in Group B
P3: comparison of the means between Group A and B
Discussion
This study was aimed to compare the efficacy of UKO and LWI on static balance in patients with knee osteoarthritis. In our study, the mean of stability score in baseline (92.6 ± 1.35) was lower than UKO (94 ± 1.13) and was statistically significant (p < 0.05). The mean of stability score in baseline (92.6 ± 1.29) was found to be slightly greater than LWI group (91.8 ± 1.72), however the difference is non-significant (p > 0.05). Inter-group comparison between UKO (94 ± 1.13) and LWI (91.8 ± 1.72) with respect to stability scores showed significant differences in favor of knee orthosis (p < 0.05). Identical results were observed by Chuang et al. who found significant improvement (28%) in balance scores with the use of an elastic knee sleeve 15 and Hassan et al. with 3% improvement in postural sway when subjects wore a loose elastic bandage. 16
The mean of COP path length in baseline (47.1 ± 9.06) was found to be greater than UKO (40.67 ± 3.45) in group A. In contrast, it was observed that baseline scores for mean path length (40.5 ± 3.47) was lower than LWI (58.8 ± 8.45) in group B (p < 0.05). While comparing the mean of both orthotic interventions, UKO group (40.6 ± 3.45) showed significant improvement than LWI (58.8 ± 8.45). Similar results were reported by Ahmadi et al. who observed difference in COP parameter did not reach significance and the balance was not affected by using insoles. 4 Zangi et al. found that lateral wedged insoles had no immediate effect on the center of pressure and medio-lateral displacements (p = 0.70). 5 In contrast Sayadnejad et al. found an improvement of approximately 20 to 30% in standard deviation of pressure center displacement in both anterior-posterior and internal-external directions using wedged insoles in medial knee OA. 17 However, Iglesias et al. reported that the immediate effect of using LWI on the average displacement and velocity of COP in medio-lateral direction was also in-significant. 18
Path length and area are different measures of COP displacement. Path is the length of the COP displacement trajectory and is therefore independent of direction. It infers that the human control system is independent of the direction of the COP trajectory and used as a basic parameter to analyse balance. The COP trajectory (Figure 4) shows larger sway area in bipedal standing in baseline assessment, which was reduced with orthotic intervention, especially with the use of UKO. Instead of being independent in direction, the subject demonstrated larger antero-posterior sway compared to medio-lateral direction. This could be due to the fact that, use of orthoses encourages a wider support of standing to enhance stability and thereby reduces the postural sway in medio-lateral direction.
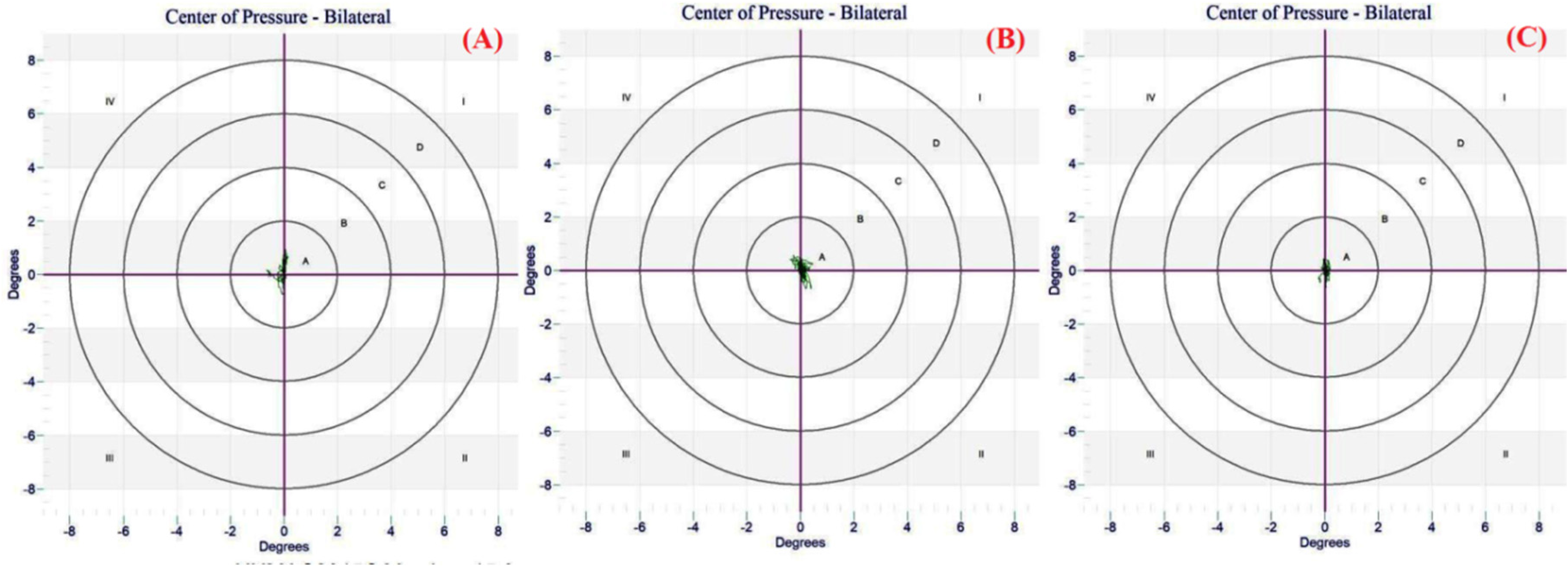
COP trajectory (A) baseline (B) LWI and (C) UKO.
The mean of average velocity of COP in baseline (0.75 ± 0.15) was greater than UKO group (0.66 ± 0.06) and is significantly different. (p < 0.05).Significant difference was observed for average velocity in baseline (0.65 ± 0.06) compared to LWI (0.95 ± 0.01) in favor of no insoles (p < 0.05). The mean of average velocity with UKO was found to be significantly lesser than with LWI (p < 0.05). Similar reports were reported by earlier investigators (Zangi et al. and Iglesias et al.) who found non-significant differences using LWI.4,18 In contrast, the study of Ganesan et al. reported decreased average velocity of the COP in standing on a surface with lateral wedge compared to the flat surface. The authors consider this change in displacement of the COP in medio-lateral direction to be related to changes in limb alignment, especially those of the hip and ankle and probable changes in muscular activity. 19 In another study, Collins et al. found no significant improvement in static balance with neoprene knee sleeve adjunct with electrical stimulation only in single-leg stance. 10
The mean of mobility score in baseline (48.0 ± 1.79) was found to be significantly lower than UKO group (57.4 ± 16.2) for our subjects (p < 0.05). The score in baseline (47.7 ± 1.57) was found to be significantly lower than LWI (62.4 ± 14.5) group (p < 0.05). However, inter group comparison between UKO (57.4 ± 16.2) and LWI (53.6 ± 15.6) did not show statistical difference (p > 0.05). This may be due to the fact that mobility scores are based on task specific activities and require all body movements for achieving the target job within a stipulated time. Restriction of knee motions with UKO may have contributed to limited functional movements and reduced mobility scoring compared to LWI and resulting in non-significant comparison (Figure 4). There was significant improvement in KOOS sub-scale score for both orthoses compared to baseline assessment (p < 0.05). There was no significant differences in the ADL (P = 0.752), or sports and recreational activities (P = 0.437) while comparing UKO and LWI. The UKO had a greater effect on the pain and symptoms sub scales than the LWI. However, QOL sub-scale scores for LWI were more effective than the UKO. This indicates that UKO was more effective than LWI in broader sense. Similar results were observed by Arazpour et al.. 20 Conversely Van Raaij et al. found no significant differences in pain and function WOMAC sub-scales between LWI and knee braces in subjects with medial knee OA. 21 Baker et al. found no statistical or clinical significance in WOMAC pain sub scale using LWI in a cross-over trial. 22
Various studies have assessed balance, risk of fall in subjects with knee OA with orthotic intervention using other parameters such as knee adduction moment, gait analysis, 6- minute walk test, Activities-specific Balance Confidence and Time up and go test along with pain which was measured through various scales. Some of those found improvement in balance using orthosis. Jones et al. compared valgus knee brace with LWI and demonstrated that both reduce the early stance external knee adduction moment and knee adduction angular impulse during walking. Greatest reductions were achieved by the LWI (12% reduction compared to 7% for the valgus knee brace). These reductions might be regarded as modest but these biomechanical changes were accompanied by significant clinical responses in both cases. 23 Dessery et al. found alleviation in knee pain with knee orthosis (p < 0.01). These knee orthoses allowed a significant reduction in peak knee adduction moment during terminal stance from 0.313 to 0.280 Nm/Bw-Ht (p < 0.001). 24 Khan et al. found that the reduction in first and second peak knee adduction moment was greatest (19.75% and 12%) when toe in was combined with knee orthosis and LWI respectively. 25 Tokunaga et al. combined toe in gait with wedged insoles, suggesting a synergistic effect of both the interventions in reducing the first peak of the knee adduction moment. 26 A crossover study by Baker et al. reported that LWI can accentuate foot pronation and retard foot supination during gait in a well-balanced foot and ankle and might accentuate pronation in an already over-pronated foot and ankle. 22 Hence, conservative management using knee braces and foot orthoses could have a positive impact on many aspects in knee OA. Moreover, treatment with orthoses has significant beneficial effects and can reduce the morbidity for these conditions. 27
The major limitation of this study may be attributed to small sample collected from a single national institute. Though, the enrollment of participants was difficult because of the strict inclusion and exclusion criteria, the study design was maintained to evaluate the true comparative effect of both orthoses use while eliminating any confounding variables. The potential confounding effect of fatigue during balance performance test was probably controlled by intermittent rest between the sessions. Further correlational studies on gait and postural balance focusing on long term effect of these orthoses are encouraged for justifying their efficacy in knee OA.
Conclusion
This study demonstrated that the use of either laterally wedged insole or unloader knee orthoses improves balance parameters and knee function scores compared to baseline assessment in subjects with mild to moderate medial knee OA. In comparing both orthotic interventions, the unloader knee orthosis shows significant improvement in all static balance parameters compared to lateral wedge insoles except mobility scores. Except ADL and sports and recreational activities, unloader knee orthosis had a greater effect on the pain and symptoms sub scales than lateral wedged insoles. However, quality of life sub-scale scores for insoles were more effective than the knee orthosis.
Footnotes
Availability of data and material
The authors declare that they have written entirely original work, and if the authors have used the work and/or words of others, then this has been appropriately cited or quoted. All data and materials will be furnished upon request.
Code availability
Not applicable.
Authors’ contributions
This is to state that all those who have made substantial contributions are only listed as co-authors including study conception and design. Material preparation, data collection and analysis were performed by Kunmun Behera and Rajesh Kumar Mohanty. The manuscript draft was written by Rajesh Kumar Mohanty and all authors read and approved the final version of it.
Ethics approval
This research followed guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board of Swami Vivekanand National Institute of Rehabilitation Training and Research (SVNIRTAR), India.
Consent to participate
The well informed written consent was obtained from the individuals or their parents prior to their participation in this study.
Consent for publication
Not applicable.
Acknowledgements
The authors would like to thank our subjects and their parents for their sincere cooperation throughout this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.