
Abstract
Background:
Patients suffering from medial compartment knee osteoarthritis (OA) may be treated with unloader knee orthoses or laterally wedged insoles.
Objectives:
The aim of this study was to identify and compare the effects of them on the gait parameters and pain in these patients.
Study Design:
Quasi-experimental.
Methods:
Volunteer subjects with medial compartment knee OA (n = 24, mean age 59.29 ± 2.23 years) were randomly assigned to two separate groups and evaluated when wearing an unloader knee orthosis or insoles incorporating a 6° lateral wedge. Testing was performed at baseline and after six weeks of each orthosis use. A visual analog scale score was used to assess pain and gait analysis was utilized to determine gait parameters.
Results:
Both orthoses improved all parameters compared to the baseline condition (p = 0.000). However, no significant differences in pain (p = 0.649), adduction moment (p = 0.205), speed of walking (p = 0. 056) or step length (p = 0.687) were demonstrated between them. The knee range of motion (p = 0.000) were significantly different between the two interventions.
Conclusion:
Both orthoses reduced knee pain. Maximum knee range of motion was increased by both interventions although it was 3 degrees less when wearing the knee orthosis.
Clinical relevance
Both orthoses reduce pain and improve gait anomalies in medial compartment knee OA. Our results suggest a laterally wedged insole can be an alternative conservative approach to unloader knee orthosis for treating symptoms of medial compartment knee OA.
Background
Primary knee osteoarthritis (OA) is a degenerative articular joint disease which leads to erosion and degradation of the articular cartilage within the knee joint. Subjects with OA experience pain and stiffness due to alteration in the cartilage structure and a narrowing of the joint space. The presence of osteophytes is commonly seen, and muscle weakness can also occur. Secondary arthritis can also occur due to a previous causative agent or event such as trauma. The cause of knee OA has not been established but it is thought that mechanical factors play a major role in development of the disease 1 and obesity is a risk factor along with a varus knee alignment. Osteoarthritis of the knee joint has been shown to develop in approximately 10% of adults over 55 years of age, and approximately 90% of cases are seen in the medial compartment. This is due to the fact that approximately 60% of the total load passes through the medial compartment of the knee in normal subjects and further degenerative changes can occur with medial compartment OA resulting in the mechanical load passing more medially through the knee than normal.2,3
The external knee adduction moment is higher than normal in patients with medial compartment knee OA and has therefore been used as predictor of medial knee joint loading. 4 Alteration to the adduction moment acting on the knee joint during walking alters force transmission through the knee, and can result in increased loading through the medial compartment. The incidence of medial compartment osteoarthritis (OA) in patients with knee OA is therefore high.5-7
Current conservative approaches to treat medial compartment knee OA involve the use of laterally wedged insoles and specifically designed knee braces. These braces are available as bespoke items or off-the-shelf (OTS), and are designed to apply three point pressure systems to either push or pull the knee into a less varus position during both swing and stance phases of gait. They may also be designed to comprise of a single upright or with dual uprights and associated superstructures. Single upright braces comprise of either a medial side member (with a suitable orthotic knee joint linking the proximal and distal superstructures and appropriate strapping) or a lateral upright with inflatable sections or bladders to translate the knee into a more valgus position. Dual upright braces may either be manufactured to a specific knee valgus angle for an individual patient, or designed so that the lateral upright may be adjusted to adjust the knee varus position within the brace.
The braces used in this study were custom made, and manufactured from a plaster of Paris cast taken with the leg in extension with the knee corrected to a less varus position while still being comfortable for the patient. The varus angulation was adjusted at fitting to ensure comfort for the patient.
Laterally wedged insoles are designed to position the ground reaction force more laterally during stance phase and increase the externally applied subtalar valgus moment. Both laterally wedged insoles and so-called unloader knee braces are designed to reduce the load acting through the medial compartment by re-alignment of the knee joint, 8 to reduce pain and increase activity levels by reducing the external adduction moment applied at the knee joint, which is required for reduction of the habitually loaded contact area of the joint. 9 Lateral wedges alter the position of the center of pressure (i.e point of application of the ground reaction force) by re-positioning it more laterally, in order to reduce the knee adduction moment.10-13 A biomechanical study by Kerrigan et al. reported that a 5° lateral wedge-type insole significantly reduced the knee adduction moment, 14 but in a randomized, crossover design of clinical efficacy, Baker et al. demonstrated that 5° laterally wedged inlays had no significant clinical effect on patients with knee OA. 15 Crenshaw et al. announced a 4% reduction in medial knee compartment contact force with 5° lateral wedge insole on healthy subjects. 16 Biomechanical studies have been performed using 3°, 5°, 6° and 10° lateral wedges.14,17 It was decided to use a 6° lateral wedge in this study to reflect the minimum correction angle proven to be effective in previous studies. Studies by Kakihana 18 and Maly 19 both demonstrated that a 5° lateral wedge was not effective in reducing the external knee adduction moment. In addition, previous studies have demonstrated that a full length lateral wedge was more effective than a rearfoot wedge only.
Knee orthoses have also been shown to decrease the net adduction moment applied by the ground reaction force by themselves applying a constant abduction (valgus) moment about the knee joint.8,11 A number of studies have demonstrated that knee orthoses decrease the knee adduction moment, 11 but very few have quantified the concomitant change in medial compartment load. 20 Pollo et al. reported an 11% reduction in medial compartment load for walking with a valgus brace, while Richards et al. demonstrated that valgus bracing gave volunteer subjects improved confidence during loading and the ability to push off vertically. 21
Despite the evidence currently available, studies directly comparing the effectiveness of knee orthoses or inlays in treating osteoarthritis of the knee are scarce and further evidence is needed of their effect on lower limb kinetics, kinematics and alterations to knee pain levels. The purpose of this study was therefore to evaluate and compare the effect of a laterally wedge inlay or a bespoke, dual upright, valgus knee brace on the following primary outcome measures: knee pain, knee adduction moment, knee range of motion (ROM), the speed of walking and step length, in volunteer subjects with medial compartment OA. To the authors’ knowledge, no evidence currently exists comparing fully bespoke dual upright knee OA unloader knee braces to laterally wedged insoles in reducing the parameters analyzed in this study.
Methods
Patients
Twenty-four patients with medial compartment knee osteoarthritis were referred to the orthotics and prosthetics department of University of Social Welfare and Rehabilitation Science for this study by orthopaedic specialists. Radiological evaluation combined with reported knee symptoms were the clinical principles used to diagnose knee osteoarthritis. The osteoarthritis classification system developed by Kellgren and Lawrence was used for grading of patients. 22
Inclusion criteria included existence of medial compartment knee OA of grade 1 or 11 confirmed by radiological examination. Exclusion criteria for the study included arthroscopic surgery in the past six months, knee trauma and amputation of lower limb, neurological disease, symptomatic spine, hip, ankle, foot disease, intra-articular steroid injection in the past three months, hyaluronic acid injection in the last nine months, previous fracture of the tibia, skin disease, peripheral vascular disease, blindness, severe cardio vascular defect and an inability to apply a brace (e.g. because of arthritis in the hand, or difficulty in bending).
Selected patients were formally enrolled into two randomly assigned intervention groups and were chosen to wear either a laterally wedged insole or an unloader knee orthosis. Once supplied and fitted with the orthosis, all patients were then asked to use the test condition for six weeks immediately prior to the time of the initial formal biomechanical evaluation. The six-week period was considered sufficient to verify wearing compliance and permit adequate acclimation to the brace or insole. The patients with bilateral knee pain wore laterally wedged insoles or knee orthoses bilaterally. The ethics committee of the University of Social Welfare and Rehabilitation Sciences approved the performance of this study.
Functional description and fitting methods of the laterally wedged insoles
The laterally wedged insoles were prepared from a cork composite (Thermocork™ (Aetrex Worldwide, Inc, Teaneck, New Jersey)) with a density of 60 durometers which gave a high resistance to compressive deformation. The insoles were constructed with a medio-lateral elevation of 10 mm along the entire length of the foot, which represented a 6° lateral wedge (Figure 1). 15 An elevation higher than this has been shown to be too uncomfortable to wear. 10 The insoles were trimmed to fit the subjects’ shoes and placed inside instead of the removable inserts of the shoes. In subjects with unilateral knee osteoarthritis, the lateral wedge inlay was used on the affected side. A flat 10-mm thick inlay (i.e. with a 0 mediolateral incline) was used on the non-affected side. All subjects in the inlay test condition group were supplied and fitted with a pair of comfortable, identically styled lightweight shoes pitched with a one-inch heel height for use during the study (Figure 2). The shoe was chosen to reflect a typical heel height and pitch which could be worn by men and women.

Laterally wedged insole used in this study.

Shoes used in this study.
Functional description and fitting methods of the bespoke unloader knee braces
The other group of subjects used a knee unloader brace which utilized a bilateral side bar design. The knee unloader orthoses were custom molded from a cast of each subject’s lower extremity (Figure 3) and used the application of the three point pressure principle in applying forces to correct the varus knee angulation. The patients were cast when lying down. Each orthosis was constructed by an experienced orthotist, and comprised of thigh and calf polypropylene shells which extended in length to 2/3 of the femoral and tibial length. The proximal and distal shells were connected via free orthotic knee joints (Figure 4). Adjustment of the valgus force was performed and set as needed for each volunteer subject at the initial fitting prior to the six-week period. The initial valgus angle was set at a position which did not exert excessive and un-acceptable interface pressure at either the proximal and distal ends of the superstructure of the orthosis or at the orthotic knee joint position adjacent to the lateral knee joint space while providing valgus correction to the knee.23,24 Patients subsequently attended on a weekly basis to adjust the orthosis fit. The adjustment was performed by the orthotist according to the satisfaction of patient in acceptance of the brace knee valgus angle.

Anterior and lateral view of lower extremity casting.

Knee unloader orthosis used in this study.
Subjective assessment
Before the biomechanical evaluations, the patients were evaluated regarding the quality of orthoses fitting and comfort. Daily self-reported wearing times by the patients of the assigned orthosis were analyzed to assess compliance when using either test condition. A visual analog scale (VAS) ranging from 0 (‘no pain’) to 10 (‘worst pain imaginable’) was also used for pain assessment when walking in both groups.
Biomechanical analysis
For each patient, gait analysis was conducted under two conditions: without the orthosis and with the orthosis, in random order. Five walking trials were recorded for each condition. The marker data were captured by a Vicon digital motion capture system (Oxford Metrics, UK, 640), using six cameras (Vicon, Infrared) at a frequency of 100 HZ and two force platforms set apart and positioned to capture a left and right heel strike (Kistler 9286BA, Switzerland). Fourteen markers were placed bilaterally over the position of the greater trochanter, lateral condyle of the femur, head and lateral malleolus of the fibula, the second metatarsal, ASIS, calcaneus. The following parameters were analyzed: knee pain levels (using the VAS), sagittal plane knee range of motion (ROM), maximum externally applied knee adduction moment, walking speed and step length.
Data analysis
Due to the normality of data (which was confirmed using the Kolmogorov-Smirnov technique), a paired t test was used for comparing baseline and the sixth-week post-intervention. An independent t test was used for analyzing the efficacy between two orthoses. SPSS statistical software was used for analysis of data. The level of significance was set at 0.05.
Results
There were no significant differences in the means of the age, gender, body mass index (BMI) or knee osteoarthritis grade between the randomly-assigned test groups at baseline (Table 1). The two groups were therefore appropriately similar to facilitate comparison of the primary outcome measures.
The self-reported duration of knee orthosis and lateral wedge inlay usage (by using a log book) was 7.33 ± 0.88 and 7.66 ± 0.77 hours/day respectively. The usage time was reported whenever the brace was worn and during any activity. When compared to assess compliance, no significant difference between two groups were demonstrated (p = 0.745).
Subject characteristics at baseline (n = 24).
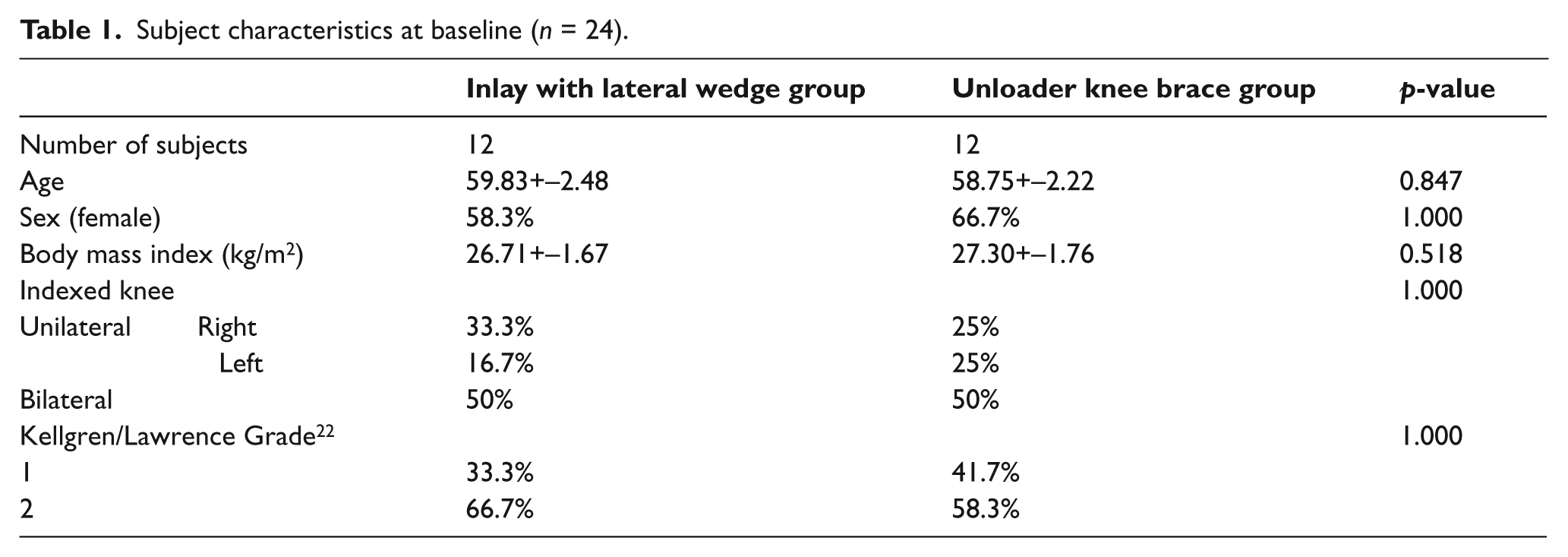
Table 2 shows the overall results following use of the assigned orthosis over the test period. The VAS pain scores, when walking without a knee orthosis (6.08 ± 0.90) or a lateral wedge inlay (6.75 ± 0.86), were significantly reduced to 3.83 ± 0.83 when walking with a knee orthosis and to 3.91 ± 0.79 when walking with a lateral wedged inlay (p = 0.000). However, there were no significant difference in reduction of pain scores between the two test groups for these conditions (p = 0.649).
When comparing the change between baseline and six-weeks post-intervention, the knee range of motion, adduction moment, speed of walking and step length all demonstrated a significant improvement (p = 0.000) for both test conditions. There were no significant differences in the adduction moment (p = 0.205), speed of walking (p = 0. 056) and step length (p = 0.687) noted. However, significance was noted in the effects on knee ROM (p = 0.000). Patients walked with a significantly larger sagittal plane knee ROM with the laterally wedged inlays inserted in their footwear compared to when walking with the knee orthosis condition (Table 2).
Mean (SD) of variables in OA patients in baseline and six weeks after intervention.
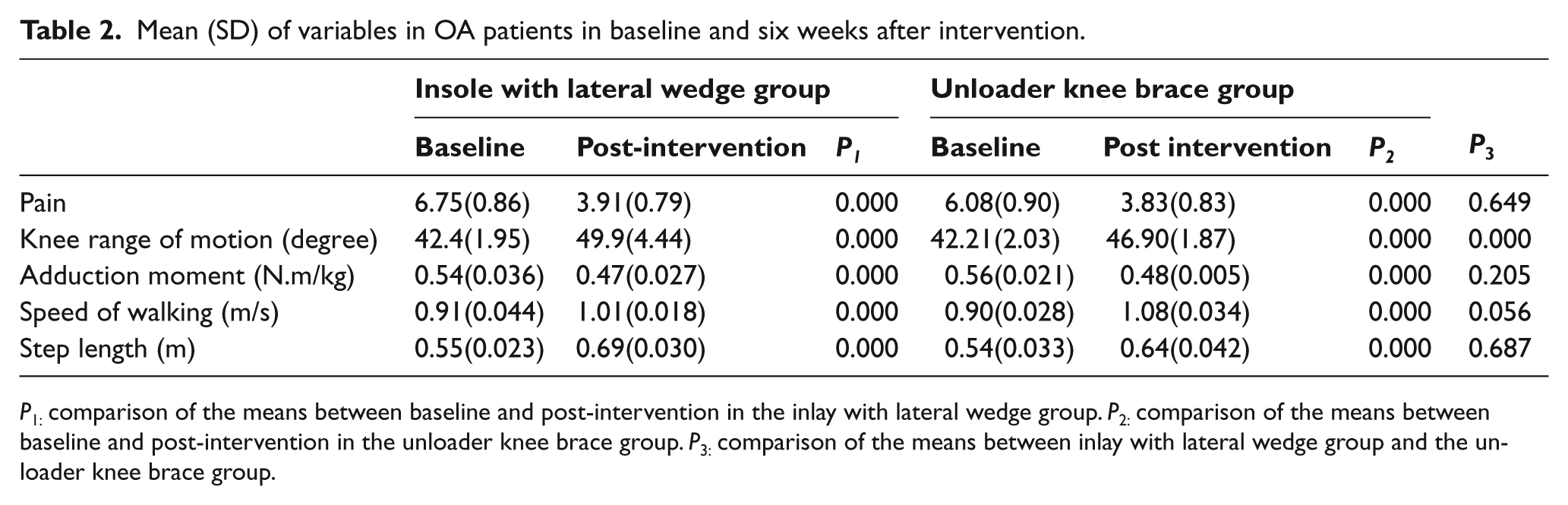
P1: comparison of the means between baseline and post-intervention in the inlay with lateral wedge group. P2: comparison of the means between baseline and post-intervention in the unloader knee brace group. P3: comparison of the means between inlay with lateral wedge group and the unloader knee brace group.
Tables 3 and 4 show the results demonstrated by patients who were either unilateral or bilateral users of the interventions.
When analyzing the data acquired for patients with unilateral knee OA (Table 3), again no significant differences were noted between the conditions in reducing pain levels. However, significance was noted in the knee ROM between the two test conditions. The increase in knee ROM for the lateral wedge condition, 46.98(±1.88) degrees, was significantly less (p = 0.205), than that noted for the unloader knee brace group; 53.6(±3.00). This did not occur in the patients with bilateral medial compartment knee OA (Table 4).
The effect of knee orthosis and insole with lateral wedged insoles in patients with unilateral knee osteoarthritis.
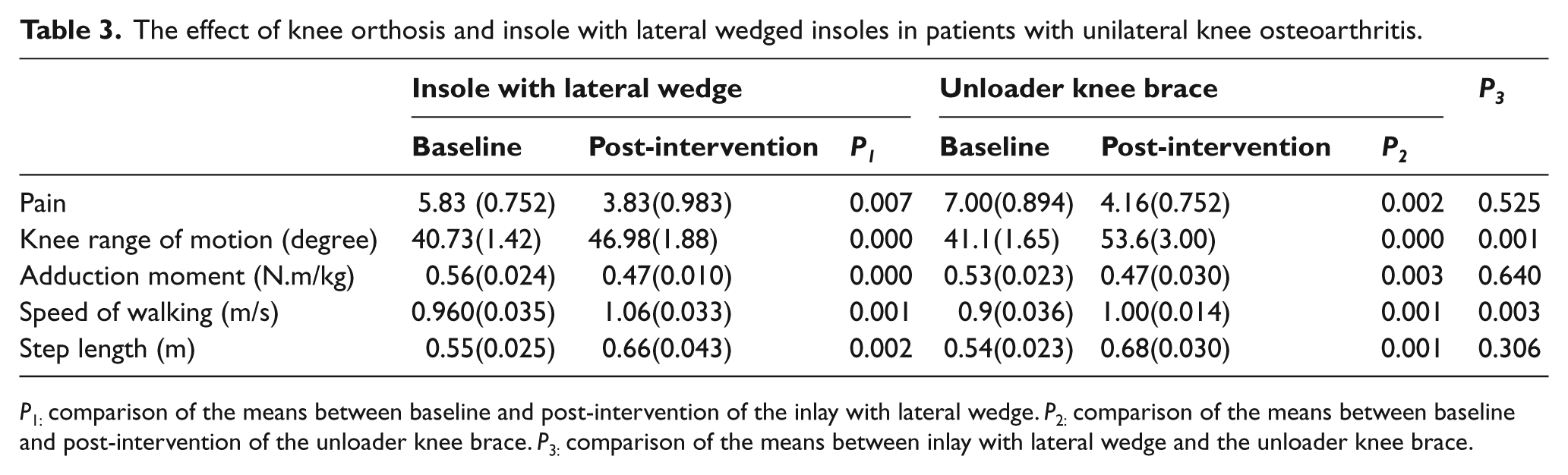
P1: comparison of the means between baseline and post-intervention of the inlay with lateral wedge. P2: comparison of the means between baseline and post-intervention of the unloader knee brace. P3: comparison of the means between inlay with lateral wedge and the unloader knee brace.
The effect of knee orthosis and insole with lateral wedge insole in patients with bilateral knee osteoarthritis.
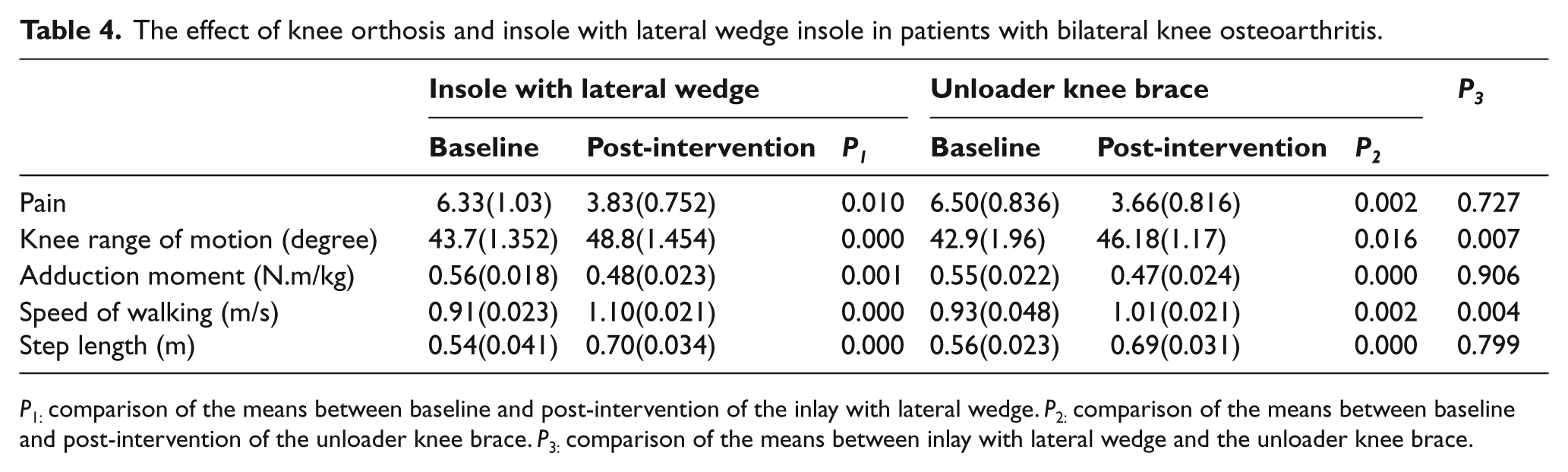
P1: comparison of the means between baseline and post-intervention of the inlay with lateral wedge. P2: comparison of the means between baseline and post-intervention of the unloader knee brace. P3: comparison of the means between inlay with lateral wedge and the unloader knee brace.
Discussion
The aim of this study was to determine, analyze and explain the effects of lateral wedges and valgus knee braces on the knee adduction moment, knee ROM, speed of walking and step length during gait, as well as their effect on knee pain scores in subjects with medial compartment knee OA.
Previous studies have demonstrated the effect of these two types of intervention in the treatment of medial compartment knee osteoarthritis, but have not compare the effectiveness of these orthoses directly. This study utilized a randomized group design to compare their effect on the selected parameters. It was thought that a crossover design would not be ideal because blinding would not be attainable. In addition, the carryover effect of bracing in the treatment of medial compartment knee OA is unknown. It was decided to utilize two randomized treatment groups (those using a laterally wedged inlay or an unloader brace) in order to reduce expectation bias, as the patients were unaware of the effective mechanism of the two orthosis options.
The authors were, however, aware of the previous evidence demonstrating effectiveness of use of a laterally wedged inlay and also an unloader brace in isolation for patients with osteoarthritis of the knee, and wanted to directly compare the effectiveness of these treatments. Secondly, if a study showed no significant difference in symptoms and specific biomechanical measures were demonstrated between uses of a laterally wedged inlay to that of a custom-made unloader brace, this would have ramifications for clinical practice.
The present study clearly demonstrated a reduction in pain for all of the patients who were treated with the unloader brace or lateral wedge insole. There was no significant difference noted between them in the reduction of knee pain. Both orthoses reduced the adduction moment in these knee OA patients, but there was no significant difference observed between the two test conditions. Lindenfeld et al. found a significant difference in the adduction moment when walking with an unloader type knee brace. 8 Similarly, Pollo et al. found a decrease in the applied adduction moment in their small group of nine subjects, 20 but Hewett et al. found no change in the adduction moment in patients who used an unloader brace. 25 Horlick and Loomer found some decrease in pain but no improvement in function with use of an unloader brace. 26
It should be noted that, although the unloader brace and laterally wedged inlay were both effective in the treatment of patients in this study, it is not yet clear which subjects are ideal candidates for either orthosis and additional studies are required in this field. The long-term effects on the foot and ankle when wearing either type of orthotic intervention, or indeed the ideal biomechanical foot type, also need to be explored further.
Alterations in the gait pattern between the knee orthosis, lateral wedge insole and without orthoses conditions in this study could have been influenced by changes in knee range of motion, walking speed and step length. A reduction in the adduction moment and improvement in knee ROM resulted in significant differences in the speed of walking and step length when compared to the without-orthosis condition. Walking without the knee orthosis or the laterally wedged inlay in this study may therefore be characterized by a decrease in walking speed accompanied by significant step-length asymmetry. These findings were similar to those demonstrated by Schmalz et al. and Kaufman et al.23,24 Inducing an alteration to gait patterns can therefore feasibly be an effective mechanism to decrease joint pain, via the reduction in the external varus moment, which correlates directly with a reduction in joint contact forces. The present study demonstrated that two types of orthoses can also contribute to a more symmetrical gait pattern as evidenced in both unilateral and bilateral cases. This reduction in asymmetry may relate with the pain-decreasing effect of these orthoses.
The two types of orthoses used in this study, demonstrated via the use of gait laboratory techniques, both increased the sagittal plane knee ROM for the varus gonarthrosis subjects included in the study, but the mean values still remained lower than that of normal walking. The knee unloader orthosis, which provided its corrective effect through three pressure point systems, had less effect than the lateral wedge. This was thought to be due to the restriction caused by the brace superstructure and strapping and the friction applied in the orthotic knee joints. The lateral wedge inlay probably provided its effect through an indirect alteration of the adduction moment and a subsequent decrease in compartment loading.
One limitation of this study was that only the external adduction moment calculated from the reflective markers and data acquisition system plus embedded force plates acting on the knee was reported. Moreover, the authors did not determine the contribution of the brace and laterally wedged inlay to the displacement of center of pressure and ground reaction force about the knee, as well as moments acting on the knee in other planes and their associated powers. A future study in this field is required for evaluation of these parameters.
Conclusion
This study demonstrated that the use of either laterally wedged inlays or knee unloader orthoses both improve knee pain and ROM and increase speed of walking and step length in conjunction with a reduction in the adduction moment applied to the knee in subjects with symptomatic medial compartment knee OA. In comparing both interventions, no significant differences in pain, adduction moment, speed of walking and step length were noted. The inlay condition was more effective in increasing knee ROM. In improving pain, knee ROM, adduction moment, speed of walking and step length, lateral wedges also showed that they were a suitable alternative to knee unloader orthoses for conservative treatment of the medial compartment knee osteoarthritis patients. The results of this study support the theory that both valgus bracing and laterally wedged inlays can significantly reduce medial compartment loads, which is consistent with patient reports regarding pain improvement with the use of both orthoses. It would be interesting to determine the effect of wearing both orthoses in combination on the same lower limb to see if the positive effects of both interventions would be compounded.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None