
Abstract
Background:
Valgus bracing in medial knee osteoarthritis aims to improve gait function by reducing the loading of the medial compartment. Orthosis composition and optimal adjustment is essential to achieve biomechanical and clinical effectiveness.
Objectives:
To investigate biomechanical functionality during gait, pain relief and compliance in patients with knee osteoarthritis using a lightweight adjustable knee unloader orthosis.
Study Design:
Prospective observational clinical trial.
Methods:
Instrumented gait analysis in 22 patients with unilateral medial knee osteoarthritis was performed after a 2-week orthosis acclimatisation period. Kinematics and kinetics during gait as well as force transmission from the orthosis to the knee were analysed. Measurements were performed without, at individualised and at reduced orthosis setting. The assessment was supplemented by patient-related pain sensation and compliance questionnaires.
Results:
Orthosis wear significantly reduced the knee adduction moment by up to 20% depending on orthosis adjustment, whereas pain sensation was significantly reduced by 16%. A significant positive correlation was found between force transmissions and knee adduction moment as well as for frontal knee angle. Compliance was good with a main daily use of 2–6 h.
Conclusion:
The orthosis provides significant biomechanical improvements, pain relief and good patient compliance. Patients had a biomechanical benefit for the individualised and reduced orthosis adjustments.
Clinical relevance
In patients with medial knee osteoarthritis, a lightweight medial unloader orthosis effectively reduced external knee adduction moment and pain sensation during daily activities. Thus, use of lightweight orthoses effectively supports conservative treatment in medial knee osteoarthritis.
Background
Knee osteoarthritis (OA) is one of the major degenerative joint diseases of the lower extremity with an overall prevalence of around 3.8% and is often associated with pain and limited mobility.1–6 The highest incidence of knee OA is seen in patients between 55 and 64 years of age, indicating that knee OA is not only an issue of the aged population. 7 The onset and disease progression is associated with several etiological factors such as obesity, trauma, lack of physical activity and varus misalignment of the frontal knee axis.8,9 Medial knee OA is frequently associated with increased loads transmitted through the medial knee compartment, which primarily contribute to an increased external knee adduction moment (KAM) during gait.4,10,11 One conservative treatment strategy frequently used to counteract these increased loads is valgus bracing. The main biomechanical purpose of these orthoses is to shift the resultant ground reaction force vector more laterally in order to reduce the KAM.12–14 Several studies investigated these effects by the use of instrumented gait analysis, and recent systematic reviews reported that valgus bracing reduces KAM and therefore abnormal loading of the medial compartment.15,16 In contrast, some studies were identified, which did not find significant changes in this biomechanical key parameter. 16 This indicates that the biomechanical effects might be highly dependent on variables such as orthosis composition and adequate fitting. Stiff orthoses could lead to a higher load reduction, as observed in patients with increased varus deformities who showed profound biomechanical improvements by wearing rigid knee unloader orthoses.14,17 Other studies reported that the amount of valgus setting and orthosis design can influence biomechanical gait parameters as well as pain relief.14,18,19 Orthosis fitting is also important concerning patient compliance, which usually suffers from discomfort, inadequate setting, orthosis weight and skin irritation. 20 In order to address these important issues, orthoses with adjustable settings and decreased weight have been introduced. In this context, a new lightweight double upright self-adjustable knee orthosis (OA Nano, DJO Global™) promises biomechanical effectiveness as well as pain relief and high wearing comfort. Usage of this orthosis is intended for medial knee OA and accordingly composed of a manually adjustable unloading mechanism to reduce the load of the medial compartment. 21 However, the biomechanical and clinical effectiveness of this adjustable orthosis for patients with medial knee OA has not been investigated yet. The main focus of this study was to investigate gait analysis parameters and their changes in varying orthosis settings and in comparison with the unbraced condition. We wanted to check whether there is a causal link between the individual adjusted orthosis setting and the mechanical loading of the knee and whether the flexible and lightweight orthosis still provides adequate effects during gait in a setup with reduced external valgisation. Considering clinical relevance of orthosis usage, a further aim was to investigate pain relief and patient compliance. We hypothesised that wearing the knee orthosis reduces the external KAM and pain intensity in patients with symptomatic medial knee OA. Furthermore, we expected that the amount of mechanical loading, in this case the KAM, is related to the magnitude of knee valgisation and force transmission (FT) induced by the orthosis.
Methods
Subjects
A total of 22 patients (12 male, 10 female; age = 61.5 ± 8.8 years; body mass index (BMI) = 29.04 ± 4.86 kg/m2) with unilateral medial knee OA agreed to participate in this observational clinical trial. Inclusion criteria were an age between 40 and 70 years, radiological secured cartilage damage according to Kellgren & Lawrence Grade II and III, index of severity for knee disease (ISK) according to Lequesne greater than or equal to 10 points and pain intensity on 100 mm visual analogue scale (VAS) larger or equal to 40 mm.22,23 The presence of medial compartment OA and grading of OA severity was confirmed by X-ray. Exclusion criteria were diseases influencing walking ability, acute joint effusion, prior surgery, other joint disorders or implants and contraindications for orthosis utilisation (skin disorder, infection, diabetes) or use of another orthosis. Patients fulfilling the inclusion criteria were informed about the project and gave their written consent. The clinical study was approved by the ethics commission of the Bavarian Medical Association (Nr. 12103), conducted according to the guidelines of the Declaration of Helsinki of the World Medical Association and registered in the German Clinical Trials Register (DRKS00009714).
Orthosis setup and acclimatisation period
Each patient received the lightweight knee orthosis (OA Nano, DJO Global™) consisting of a self-adjustable 3-point off-loading mechanism which induces a mechanical weight shift to the lateral compartment of the affected knee. 21 For the individual adjustment, two regulating screws at the lateral frame can be individually tightened using a hex-wrench. The orthosis consists of polyaxial hinges to match with natural knee kinematics and three fixation straps that anchor the tibia and the femur to the proximal and distal cuffs. An additional strap across the back lower thigh pushes the femur anteriorly, whereas a distal strap at the shin prevents the tibia from anterior translation. A malleable lightweight magnesium frame allows for patient-specific cuff adjustment in order to optimise individual fitting and to provide strength to unload. After a standard medical examination, individual orthosis adjustments were performed for each patient by an orthopaedic technician who was completely blinded to the study design. Briefly, orthosis alignment was adjusted to patients’ leg contours and strap fixation was performed during sitting with the knee flexed. It was visually ensured that the hinges were centred above the top of the patella and slightly behind the midline of the leg. Afterwards, valgisation was individually adjusted to patients’ demand. Prior to orthosis fitting, pain sensation using the VAS score as well as drug medication was documented. To familiarise themselves, patients were instructed to wear the orthosis during physical activity over a period of 2 weeks. Patients were permitted to adjust their orthosis setting due to discomfort and/or pain sensation. A simple patient diary was used to document daily wearing time (<2 h, 2–6 h, 6–10 h, >10 h or not worn). After the 2-week period, patients returned to the clinic and were asked about comfort, handling and further use of the orthosis by a short questionnaire. Proper fit of the orthosis was reassessed by the orthopaedic technician. Pain sensation as well as analgesic treatment was also documented at the same time.
Instrumented gait analysis
The biomechanical effectiveness for braced and unbraced conditions was investigated through instrumented gait analysis after the 2-week acclimatisation period. Measurements of gait kinematics and kinetics were performed at a sampling frequency of 200 Hz using an eight-infrared-camera system (Vicon MX-T20, Oxford, UK) synchronised with two embedded force plates (AMTI OR6-7-2000, Watertown, USA). A total of 21 reflective markers were placed on subjects according to the Conventional Gait Model.24,25 As knee markers had to be placed on the polycentric hinges of the orthosis, total knee width (knee and hinges) was measured and implemented in the biomechanical model for adjusting the calculation of the knee joint centre. Gait analysis was randomly performed for the following conditions: unbraced, braced and reduced braced. The reduced braced setting was performed in the same way for every patient by one turn of the proximal and distal regulation screws while wearing the orthosis during standing. It was ensured that there was still contact between skin and condyle pads of the orthosis. To minimise orthosis condition bias, three patient blinded washout trials were performed between each measurement. A total of six valid gait trials per measurement condition were used for further kinematic and kinetic analysis. To eliminate influence of shoe wear, gait measurements were performed barefoot. In order to measure force interaction between the skin and the lateral condyle pad, a portable pressure distribution system (Novel Pedar X, Munich, GER) with an elastic measuring mat (sensitivity: 50–200 kPa; 100 Hz sampling frequency) was used. This setup was used to measure the maximum FT during the first part of the stance phase at both orthosis settings (Figure 1).
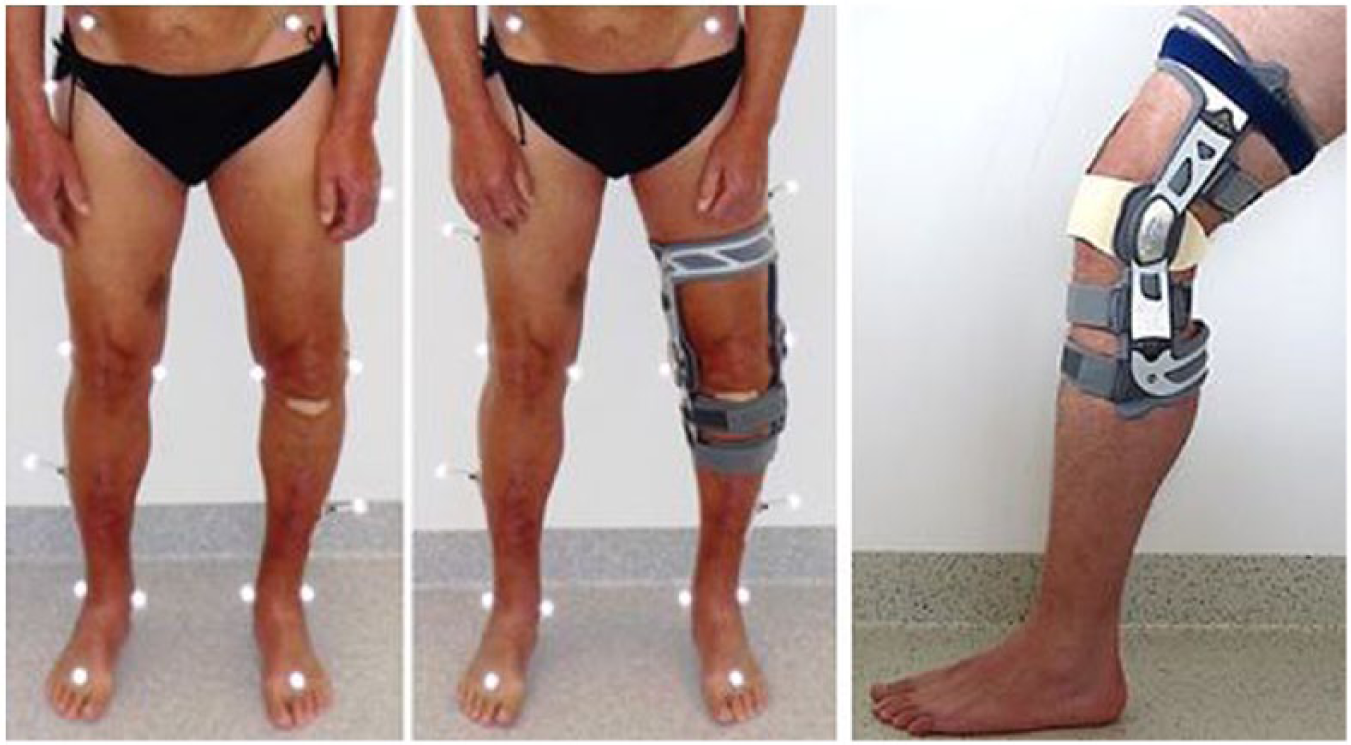
Patient with unilateral medial knee OA equipped with and without the knee unloader orthosis (left and middle). Knee orthosis equipped with the measuring mat between lateral knee and lateral condyle pad (right).
Gait parameters were subdivided into loading phase (LP) and push-off (PO) phase which consisted of 0%–50% and 50%–100% of stance phase, respectively. 26 The maximum external KAM, maximum normalised ground reaction force, maximum frontal knee angle and maximum foot progression angle of the affected knee were analysed. Walking velocity, step length and cadence were also measured. Maximum FT of the orthosis at heel strike (LP) was normalised by body weight and was measured for both adjustments.
Statistical analysis
Data analysis was performed using SPSS version 19.0 (SPSS Inc, Chicago, USA). Power analysis revealed that a total of 20 patients provided 80% power (α = 0.05) to detect a clinically relevant difference of 0.1 Nm/kg of knee adduction. Normal distribution of data was confirmed by Shapiro–Wilk test. Analysis of variance (ANOVA) for repeated measurements was used to determine differences between the three conditions. Bonferroni correction was performed for post hoc pairwise comparisons. The relationship between orthosis setting and gait parameters was investigated using the Pearson correlation coefficient. The level of significance was set at 0.05.
Results
Wearing the orthosis resulted in a significant (p < 0.05) reduction of the KAM and the frontal knee angle during both gait phases (LP and PO) and both orthosis adjustments (Figure 2). Furthermore, KAM was significantly larger at heel strike (LP) compared to PO for the individual (p = 0.04), reduced (p = 0.02) and unbraced (p = 0.003) conditions.
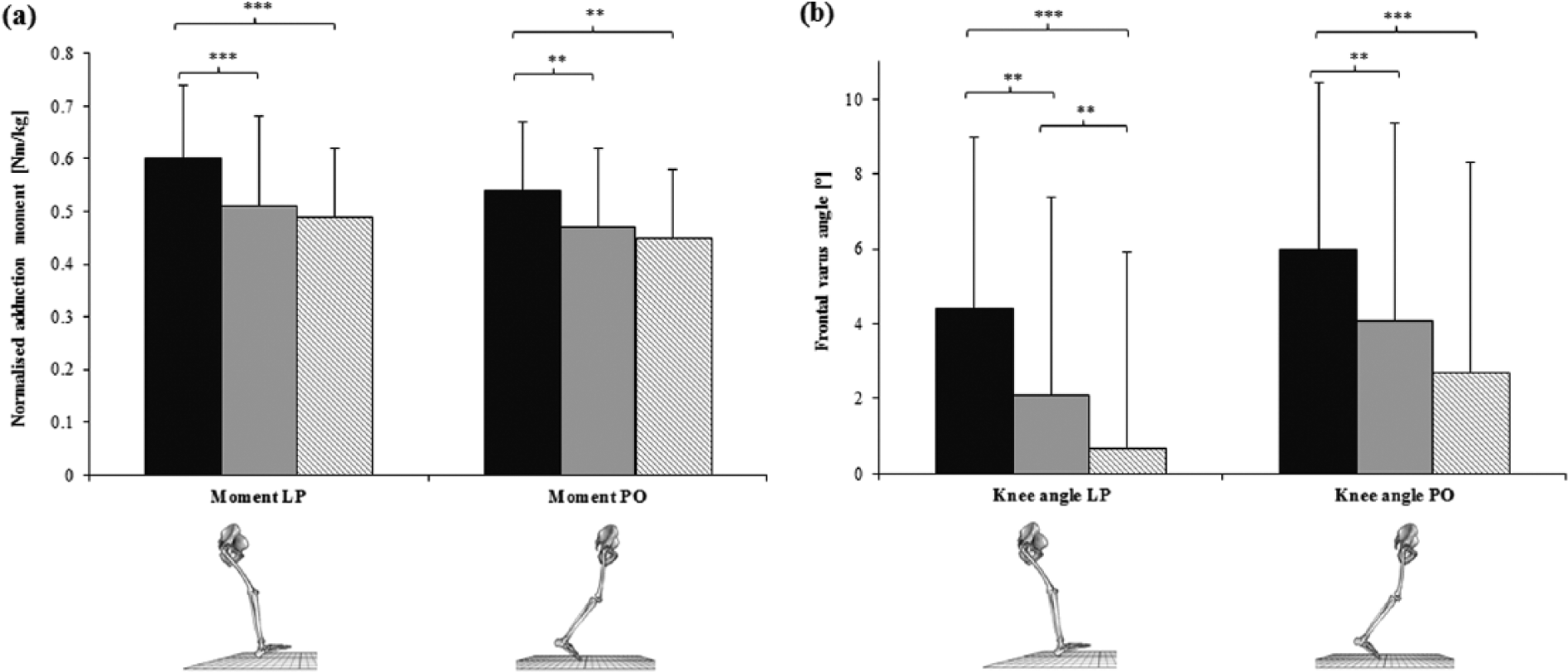
(a) Peak KAM and (b) peak FKA during loading and push-off phase for the unbraced (black), reduced braced (grey) and individual braced (dashed) setting.
The frontal knee angle (FKA) was significantly reduced if the orthosis was worn with larger reductions observed for the individual orthosis adjustment compared to the reduced adjustment (Figure 2). A significant difference between LP and PO with larger varus knee angles during PO was also found for the individual (p < 0.001), reduced (p = 0.002) and unbraced (p = 0.007) conditions. Pain, as assessed by VAS scoring, was significantly reduced (p = 0.005) by 25% (65 ± 17 mm to 49 ± 25 mm) after wearing the orthosis for 2 weeks.
Four subjects had to be excluded from the analysis of FT, as no force was detected by the measuring mat during walking. FT was significantly (p = 0.001) smaller after the adjustment was reduced. No significant differences between the three conditions were found for ground reaction force, foot progression angle and spatiotemporal parameters. KAM was strongly correlated with the frontal knee angle during the LP (Figure 3). The forces transmitted by the orthosis were moderately associated with both the KAM and the knee angle (Table 1).
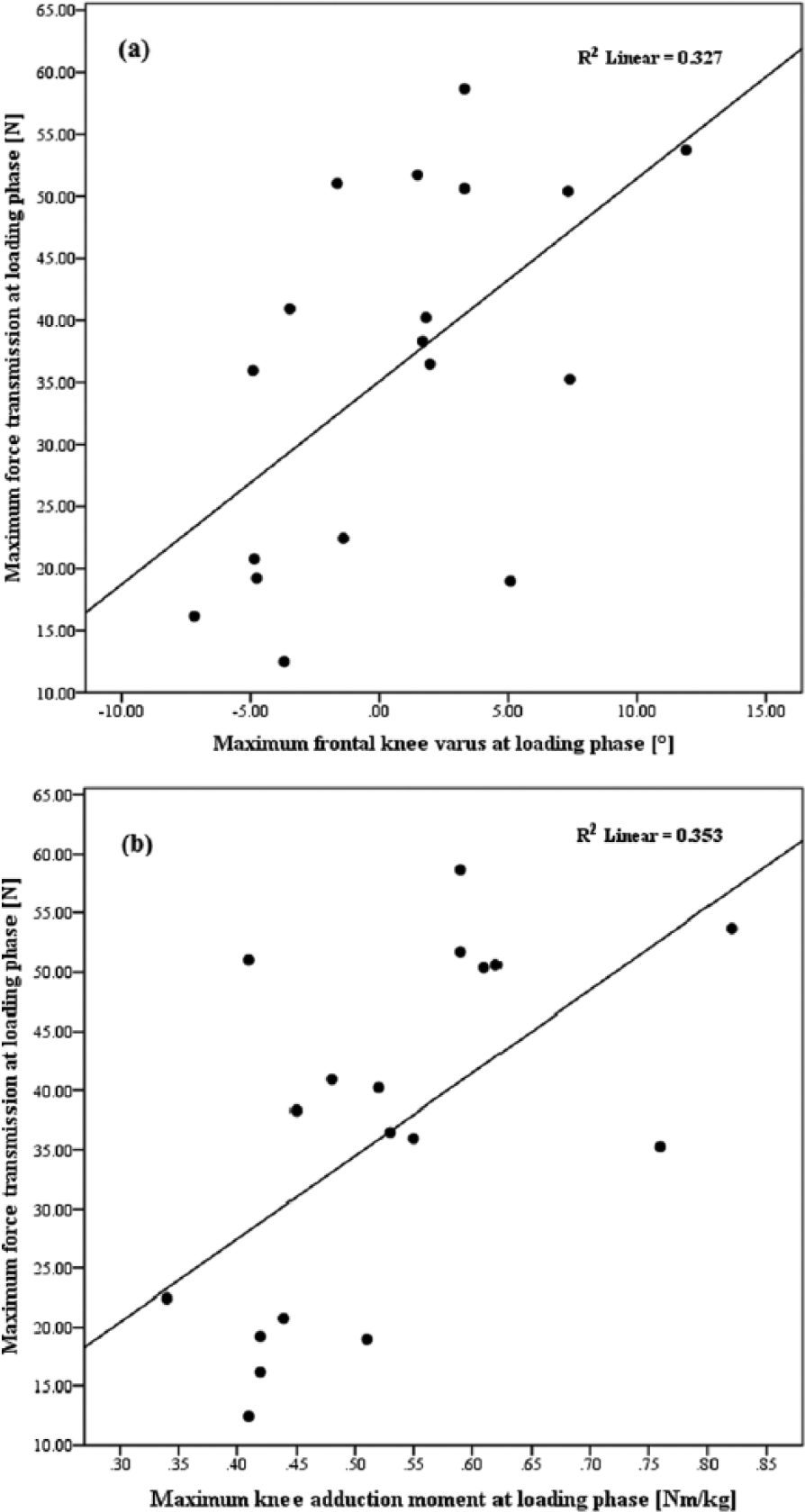
Scatter plots with linear regression lines for analysis of relationship between orthosis force transmission and frontal knee angle (a) and knee adduction moment and (b) at individual orthosis setting.
Correlation analysis between gait parameters and force transmission for the individual braced condition during loading phase.
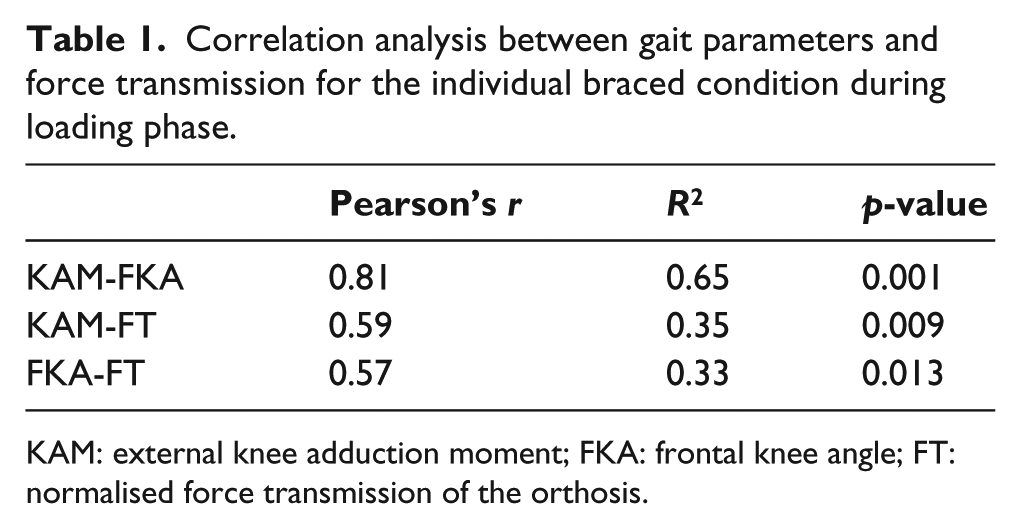
KAM: external knee adduction moment; FKA: frontal knee angle; FT: normalised force transmission of the orthosis.
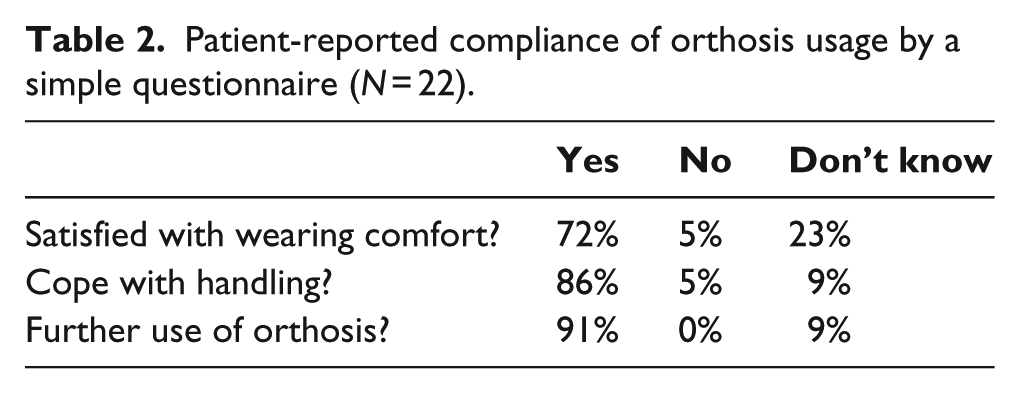
Patient-reported satisfaction of orthosis comfort, handling and further use revealed positive results indicating a good patient compliance (Table 2). Daily wearing time ranged from more than 10 h to not worn, while patients predominantly used the orthosis between 2 and 6 h/day (Figure 4). A total of 12 patients used the orthosis every day over the 2-week acclimation period, whereas 10 patients did not use it continuously (range: 1–6 days).
Patient-reported compliance of orthosis usage by a simple questionnaire (N = 22).
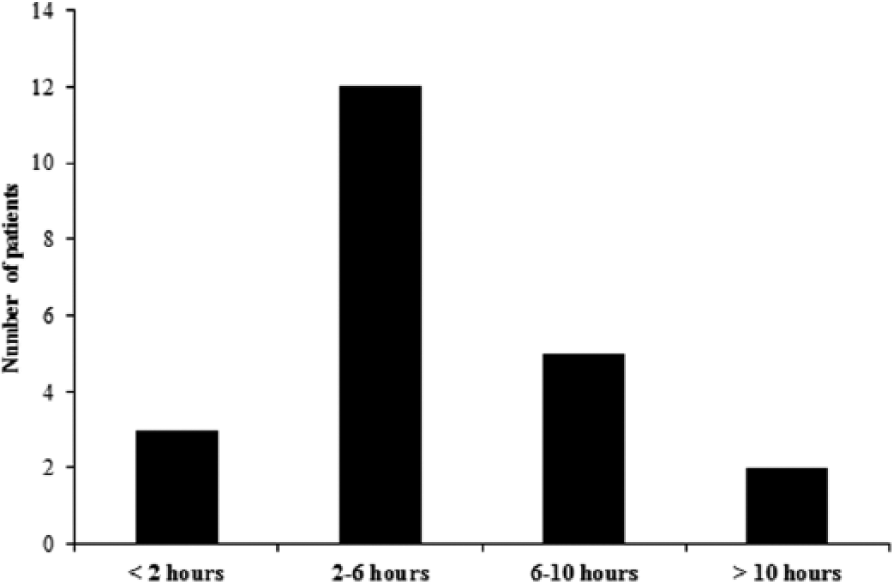
Number of patients with corresponding predominant wearing time (mode) during the 2-week acclimatisation period.
Discussion
The aim of the study was to evaluate the clinical and biomechanical effectiveness of a lightweight knee unloader orthosis in patients with symptomatic medial knee OA. Wearing the orthosis improved knee function by reduction of KAM and frontal knee angle. The functional improvement was accompanied by a clinically relevant reduction in pain during walking. Load transfer to the knee was directly associated with the level of functional improvement.
Several advantages of wearing the knee orthosis were identified in this study on patients with symptomatic medial knee OA. Supporting our first hypothesis, wearing the knee orthosis decreased the KAM and the medial knee load independently of the individual adjustment. This finding agrees with other studies which found comparable reductions of the KAM by valgus bracing.18,19,27–36 In our study, the KAM for the individual and reduced orthosis settings compared to unbraced settings showed reductions of up to 18% and 15% for LP and up to 16% and 13% for PO, respectively. These results underline a certain clinical relevance as KAM compensations of around 10% were thought to be the main mechanism for pain relief and overall function in knee OA. 36 The measured reductions were also comparable to those reported previously.14,27 Pollo et al. 19 also investigated the KAM at different orthosis settings and found differences for the net knee varus moment of up to 20%. However, no significant reductions were found for the KAM. In contrast to these studies, we did not use exact settings given by fixed angles for the valgus adjustment, which might be one explanation for a smaller percentage of reduction when wearing the orthosis. As a comfortable individual orthosis setting is intended and since increased valgus settings or unrealistic tight adjustments might not be tolerated by patients for long-term use, we chose a setting according to patient comfort. Differences might also come from various orthosis designs that immediately influence the mechanical axis of the knee and therefore the KAM. The orthosis investigated by Pollo et al. 19 consisted of one strap and only one hinge, whereas Fantini Pagani et al. 27 investigated an orthosis with two hinges and longer lever arms. The orthosis investigated in our study consisted of two hinges and a very tight strap fixation. Due to differences in design, material properties, number of straps and cuff position, several alterations in stiffness, orthosis migration or compensatory movement of the thigh and the shank during walking might occur. This could be an explanation of differences in the biomechanical outcome of various knee unloader orthoses. Nonetheless, the positive biomechanical changes of both orthosis settings compared to walking unbraced also underline that adjusted as well as unadjusted orthoses have the potential to improve knee function in medial knee OA.
The reduction of the KAM during gait is often explained by maintaining an external foot progression angle, which is known as a strategy to reduce the KAM, especially during PO. However, in this study, foot progression angle was not significantly altered. This is in agreement with previous studies, which demonstrated that toeing out was not changed by knee bracing.17,31 Nonetheless, we assume that a combination of both maintenance of external foot rotation and reduced knee varus might be the mechanism of reducing medial knee load in valgus bracing. In our study, the frontal knee angle was significantly reduced by wearing the knee orthosis. Supported by the strong positive correlation with the KAM, alteration of frontal knee angle is a main parameter for reducing medial knee load. 37
The results support our second hypothesis that the amount of mechanical loading of the knee is related to the magnitude of knee valgisation and FT induced by the orthosis. These findings agree with Pollo et al. 19 who showed that an increased valgus correction achieves a greater amount of unloading of the affected compartment. Furthermore, our results are also somewhat comparable to a study from Hunt et al. 37 who found significant positive correlations between the peak KAM and the frontal knee lever arm in patients with medial knee OA. This study is one of the first that measured force interaction at the contact zone between the skin and the orthosis during gait in medial knee OA. The positive correlations between the induced forces and the resulting kinematic and kinetic changes indicate that increased knee moments and knee varus angles create larger contact forces at the lateral condyle pad. It could be assumed that patients with larger varus knee alignment and higher KAM might therefore increase the manual adjustable valgus setting, which consequently results in a greater contact force. As the individual orthosis setting was not quantitatively measured, further more detailed investigation is needed to fully understand causes and effects of orthosis adjustments.
Pain was significantly reduced after wearing the orthosis which supports our first hypothesis. These results agree with previous studies demonstrating a decrease in pain sensation after valgus bracing.17–19,27,32 In our study, the mean reduction of pain after 2 weeks was 16 mm, which is within the range of the minimal clinically important difference. 38 An extended acclimation period might possibly allow for a more clinically relevant outcome. Nonetheless, patient compliance was good while using the orthosis during the 2-week period. Mean daily wearing time among patients was between 2 and 6 h which is comparable with findings in other studies where regular orthosis usage at an average of 5 h/day was stated.39,40 However, some patients in our study also wore the orthosis for more than 10 h/day which widely exceeds regular daily wearing time. Patients generally rated the orthosis as handy and comfortable and intended further usage. As no long-term follow-up was performed in this study, only immediate effects can be presented. It must be considered that a decrease in patient compliance occurs beyond a 1-month period after orthosis ambulation with even higher decreases of up to 72% after 1 year. 20
This study has some limitations. In all gait studies, the kinetic and kinematic results strongly depend on spatiotemporal parameters. These parameters (i.e. walking speed) were not significantly different among orthosis conditions; hence, our findings were unlikely to be biased by differences in walking, potentially caused by different pain sensation or discomfort. 41 Correlation analyses could only be performed for a subgroup of 18 patients due to inability of measuring contact forces in four patients. This might be explained by inadequate orthosis fitting as well as insufficient sensitivity of the measuring mat. The acclimatisation period of only 2 weeks might have been insufficient for testing the overall clinical effectiveness of the orthosis. However, our follow-up coincides with that of several studies that investigated the effects of knee orthoses19,29,35,40 and generally is within the range of 1–6 weeks of familiarisation.17,18,28,30,32,36,39 Therefore, we believe that this short period provides useful information concerning immediate clinical and biomechanical effects of valgus bracing. Furthermore, we did not quantitatively measure individual valgus settings of each patient. This would have provided substantial information for a closer understanding of the functionality and the relationship with knee loading moments while wearing the orthosis.
Conclusion
We found several biomechanical and clinical improvements by wearing the lightweight malleable adjustable knee orthosis in a representative population with unilateral medial knee OA. The majority of kinetic and kinematic analyses demonstrated a significant reduction of varus alignment and knee load at individual and at reduced orthosis adjustments. This would indicate that the knee orthosis is still effective even if adjustments were performed by the patients. Clinically, the orthosis significantly improved knee function, decreased pain and showed good patient compliance. At least for temporary usage, an unloader orthosis appears to be a viable conservative treatment option for patients with symptomatic knee OA.
Footnotes
Acknowledgements
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was financially supported by Ormed GmbH and by the Association for Orthopaedic Research (AFOR).