
Abstract
Background:
Patients with medial compartment osteoarthritis of the knee suffer from pain and stiffness. However, current unloader braces are not being used for extended periods by knee osteoarthritis patients due to interface problems, so compliance is an issue. The aim of this study was to design a new bespoke orthosis that could be comfortable to wear while also providing the required correction to reduce medial compartment loading.
Case Description and Methods:
A new knee orthosis design was initially tested for its frontal plane correction of knee varus using a surrogate knee model. It was then assessed by a volunteer subject with grade 2 medial compartment knee osteoarthritis using a static standing radiograph.
Findings and Outcomes:
When fitted to the surrogate knee model, the brace corrected the knee from 10° of varus to neutral alignment in the frontal plane. When worn in situ during static stance on the affected leg of the volunteer patient, it corrected the knee by 6° to a less varus position.
Conclusion:
The orthosis provided frontal plane correction of the knee during static standing. It could therefore prove to be suitable for use by knee osteoarthritis patients.
Clinical relevance
This new custom unloader knee orthosis produced a more valgus knee alignment by adjusting the pneumatic components attached to the thigh and leg shells. During static stance, it corrected frontal plane varus knee rotation by 6° in a single subject with knee osteoarthritis.
Background and aim
Knee osteoarthritis (OA) is an age-related disorder that is prevalent in older people, especially women.1–3 Knee OA is more prevalent in the medial compartment than the lateral compartment principally due to the notion that approximately 62% of the weight passes through the medial side of knee joint in healthy subjects.4–6 Indeed, the disease may progress so severely in some subjects with medial compartment knee OA that 100% of the loading passes through the medial compartment of the knee. 7 Therefore, minimization of loading on the medial compartment is the ultimate strategic biomechanical goal of treatment for patients with medial compartment knee OA. 8
A biomechanical surrogate of knee loading is the value of the external knee adduction moment (i.e. the frontal plane moment applied by the ground reaction force during stance phase of gait), which is routinely used when analysing the efficacy of treatment in this patient group. Subjects with knee OA have been shown to have higher peak external knee adduction moments acting on their knee during walking when compared to age-matched controls,9–11 which has been linked to increased severity of the disease, increased abnormal joint loading and a greater risk of radiographic progression.12,13 Surgical interventions such as unicompartmental knee replacement and high tibial osteotomy are approaches that have been used. 14 However, many individuals do not need surgery or do not want surgery, and therefore, conservative management of the individual with medial knee OA is at the forefront of treatment in this population.
Any conservative treatment should therefore demonstrate a positive effect on reducing external knee adduction moments. Lateral heel wedges have been shown to reduce medial knee loading, but their effect on pain has been questioned in two recent studies.15,16 Unloader knee orthoses are an alternative conservative method of treating knee OA using direct application of forces to alter frontal plane knee alignment while simultaneously reducing the external knee adduction moment.17–30 They have also been shown to improve confidence, function, stiffness and varus rotation during walking. 31 Draper et al. 32 demonstrated that valgus braces immediately improved the function of patients with unicompartmental OA of the knee. Kirkley et al. 33 also demonstrated that such orthoses were effective in improving quality of life, function and pain in knee OA patients.
Most studies have concentrated on analysing the effect of knee unloader braces on pain levels and quality of life measures. Statistically significant knee pain reduction was noted in a review of OA knee brace efficacy by Feehan et al. 34 in 73% of the studies reviewed. Pain relief was experienced by 76% and 98.6% of the participating patients, depending on how many of the studies were included in the calculation. Consequently, Feehan et al. 34 reported that pain relief help was documented for 98.6% of the patients. One study 35 demonstrated that the knee was in a more valgus position when corrected by an unloader knee brace. Esrafilian et al., 30 by design of the new knee orthosis that adjusted by external screws, evaluated its effect on walking in two subjects. They reported that the adduction moment applied on the knee joint reduced while patients walked with the new knee orthosis. Fantini Pagani et al. 29 in evaluation of the valgus orthosis in 4° valgus and the flexible adjustment demonstrated that both orthosis adjustments provided subjective pain reduction and improvement in function compared to the without-orthosis condition. Knee adduction moment was significantly reduced with orthosis in both adjustments, whereas the reduction in orthosis with the 4° valgus adjustment was significantly greater than the flexible adjustment (25% vs 12.5%). Fantini Pagani et al. 28 in evaluation of the valgus orthosis in neutral 4° and 8° valgus positions in walking and running demonstrated that the mean of the knee adduction angular impulse was reduced by 25% and 36% in comparison between the without orthosis and 4° and between without orthosis and 8°, respectively, during walking. The mean reductions of 18% and 23% were reported between these same conditions in running. The reduction of the first and second peak knee adduction moments was observed during walking with different orthosis conditions. A significant reduction was reported only between the without-orthosis and 8° valgus adjustments conditions during running. Using a finite-element analysis, Stamenovic et al. 27 demonstrated that with a moderate level of applied pressure in pneumatic OA knee brace, this orthosis can counterbalance a greater fraction of external adduction moment in theory.
However, brace compliance is a problem. 36 In this article, it was demonstrated that the use of the knee brace was less than 3 h per day compared to insoles. This is likely to be due to the uncomfortable superstructure and non-user-friendly designs and is likely why these devices are not being used for extended periods by knee OA patients. 37 Existing knee OA braces have mostly been adapted from designs, technology and materials previously used for braces designed to protect anterior cruciate-deficient knees. Current corrective knee orthoses, both bespoke and off the shelf (OTS), are fabricated from metal, thermoplastic or composite materials, and provide corrective forces via straps, adjustable superstructures or inflatable bladders on either the lateral or medial superstructure, which translate and rotate the proximal and distal segments of the knee towards corrective alignment. The clinical effect of using these systems over long periods may cause skin irritation.33,38 This would indicate the need for a new design of bespoke orthosis to be developed based on providing both comfort and an adequate valgus/varus correction to reduce medial knee loading.
Unloader knee braces have historically used three points of pressure to apply the corrective forces required to place a knee with medial compartment OA into a competitively more valgus position. One force would be positioned at joint line on the lateral aspect via a pad, and the other two would be theoretically positioned on the opposite side, at the most proximal and distal aspects of the medial superstructure of the orthosis. This would indicate that higher interface forces would be expected between the orthosis and the leg at the proximal and distal medial borders of the orthosis, and also at the lateral joint line, especially on OTS devices. Therefore, the design and construction of a new design of bespoke unloader knee orthosis that resolves these limitations along with proof of clinical efficacy is required.
The aim of this case study was therefore to develop a user-friendly bespoke OA knee unloader orthosis incorporating a pneumatic system and a superstructure specifically aligned in a comfortable and corrected position for the knee, and to determine its effect on a surrogate leg model and in vivo with a single subject with knee OA.
Case description and methods
A single female volunteer subject with grade 2 medial compartment knee OA (age = 60 years, weight = 65 kg and height = 160 cm) was used in this case study.
Design considerations for the new orthosis
To encourage a more even distribution of force application, a bespoke moulded superstructure offering a larger surface area for correction was thought to be advantageous, as well as lateral air bladders to again redistribute the load applied to the lateral aspect. The newly developed knee unloader orthosis proposed in this study was designed to be used by subjects with medial or lateral unicompartmental OA of the knee with a Kellgren–Lawrence Classification scale grade of 1 or 2 of the disease, who also have sufficient valgus/varus rotational correction available during non-weight-bearing and weight-bearing conditions to make the application of a brace appropriate.
The knee unloader orthosis was individually constructed for the single subject from a cast of the subject’s lower extremity. The brace was manufactured from a cast taken in the maximally corrected valgus position at which the patient felt comfortable while the patient laid supine on a couch. Orthosis casting and construction was performed by an experienced orthotist. The orthosis comprised white copolymer polypropylene shells of 3 mm thickness positioned on the medial and lateral aspect of the thigh and calf. These were connected by custom-shaped bilateral aluminium side members 20 mm wide and 5 mm thick, which incorporated bilateral aluminium orthotic knee joints (Karino Company, Iran), which comprised a polycentric geared mechanism and lateral plates. These orthotic knee joints offered free knee flexion and extension while also facilitating mediolateral stability in a slim design, and incorporated a hyperextension stop. The total thickness (including the lateral plates) of the orthotic knee joints was 15 mm (Figure 1).
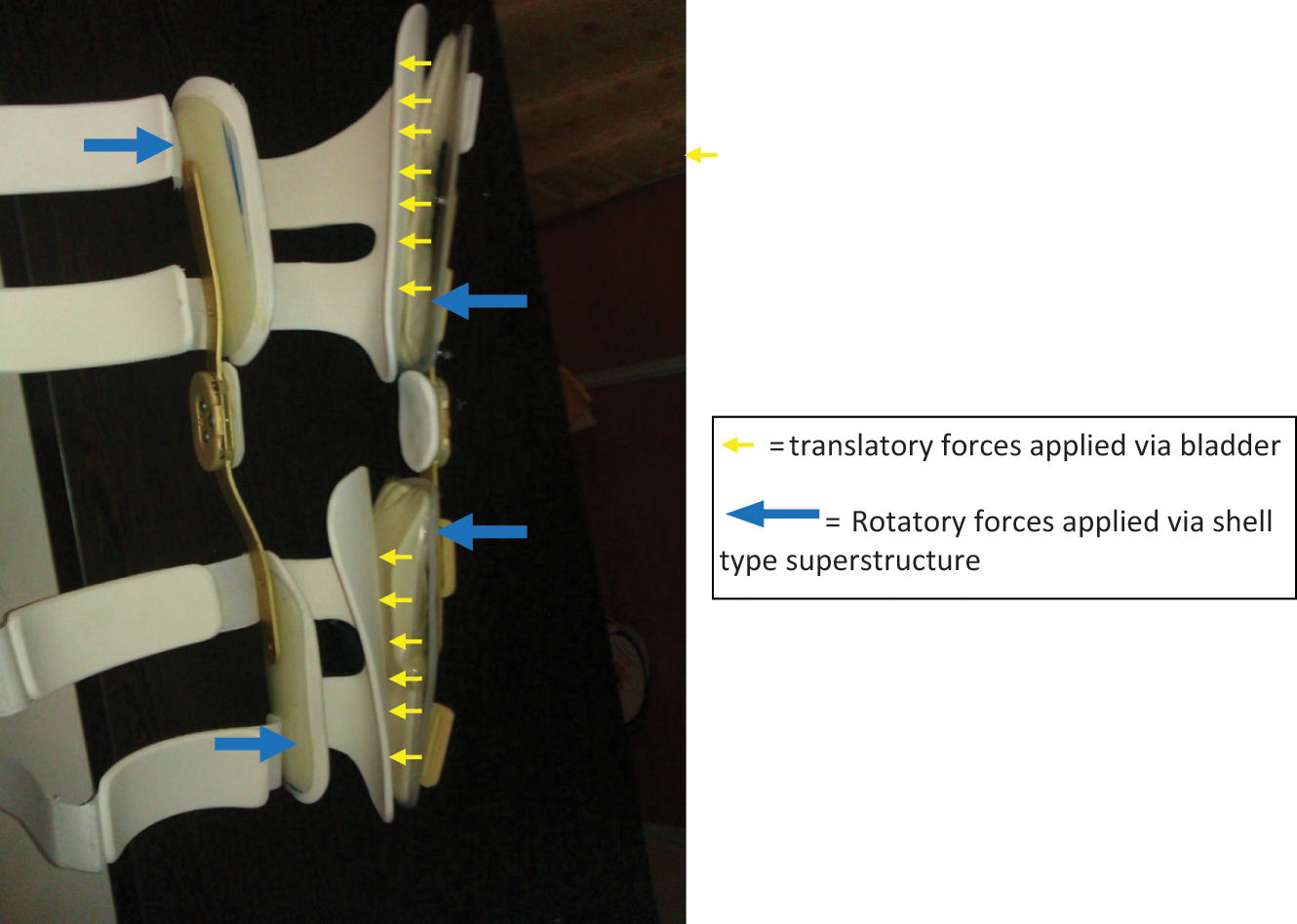
The side members used in the new orthosis and the forces acting to correct a varus knee alignment.
The superstructure extended proximally and distally from the knee joint sagittal plane centre so as to cover 2/3 of the femoral and tibial length. The extended length of the orthosis was considered important to provide suitably long lever arms for varus control within the orthosis. The orthosis was lined with 5-mm plastazote, which extended around the posterior aspect of the thigh and leg with a central cut out to reduce heat retention and to keep creasing to a minimum. The orthosis utilized four nylon straps (width = 4 mm) with hook and loop fastening that passed through plastic loops riveted to the lateral superstructure (which were designed to swivel for an accurate and comfortable fit of the straps on the front of the leg and thigh). Each strap had a protective pad made from 5-mm plastazote positioned to protect the skin on the anterior aspect of the leg. A protective pad made from 5-mm plastazote was adhered to the medial border of the orthotic knee joints.
Two inflatable bladders manufactured using nylon (240 mm long and 80 mm wide) were adhered to the lateral aspect of the proximal and distal sections of the orthosis (Figure 1). The bladders were designed to translate the thigh and leg segments against the medial superstructure, which was anatomically shaped in the comfortably corrected non-weight-bearing position. The bladders were designed to be inflated by the wearer using a detachable inflation bulb. The tube attached to the inflation bulb was permanently attached. The bladders could also be deflated so that a comfortable correction pressure could be reached.
The mechanical design of the knee joints in the knee orthosis permitted free movement in the sagittal plane, which caused the path of flexion and extension to be performed in the corrected knee position. Correction of the knee position into a more valgus position with the brace in situ was achieved by a combination of four de-rotating forces (rather than three), and inflation of the adjustable pneumatic components (Figure 1). The two lower leg frontal plane forces were designed to alter the alignment of the lower leg segment into a less rotated position via the custom-made shells (in this case to rotate it anticlockwise). Similarly, the more proximal forces via the shells acting on the thigh segment would rotate the thigh segment in a clockwise rotation. The bladders were designed to add translatory forces to both leg segments to maintain corrected position within the orthosis and also to increase comfort. The device was therefore designed to reduce the interface problems experienced from wearing previous orthoses evidenced in the literature. This was done by offering frontal plane correction via close fitting custom-made shells that would redistribute load and interface pressures over a wider area, and inflatable bladders that would not only add extra cushioning to the lateral aspect of the orthosis but also reduce friction effects and reduce leg motion relative to the orthosis during wear while maintaining the corrected lower leg position. The force system in this new orthosis is a four-point force system (Figure 1).
Figure 2 shows an overall view of the new orthosis prototype. The distinct potential advantages were its low weight (0.55 kg), its user-friendly design and the easily adjustable corrective system.

New unloader knee orthosis prototype.
The design and construction of the new orthosis was performed in the Orthotics and Prosthetics Department of University of Social Welfare and Rehabilitation Sciences. Ethical approval for undertaking the study was granted by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences.
Bench testing of the new orthosis
The first step in the assessment of the orthosis was via bench testing in the laboratory without a user in situ. The prototype was fitted to a static plaster of Paris surrogate model of the human lower leg and foot (Figure 3), which allowed an initial evaluation of the corrective performance demonstrated by the orthosis during simulations to be evaluated. The surrogate leg was manufactured from a cast of the patient used in the study. This dummy model was prepared and designed to simulate an adult female subject with 160 cm height and 65 kg weight, and incorporated a surrogate knee joint. The knee joint that was embedded in the surrogate leg model comprised a hinged joint to provide adduction and abduction movements to evaluate how effectively the new orthosis altered frontal plane motions in a static situation. The bladders therefore translated the surrogate knee in the frontal plane to react with the medial superstructure to produce valgus knee rotation.

Static plaster of Paris surrogate model of the human lower leg and foot.
The aim of this experimental testing of the orthosis was to determine any problems with corrective function applied by the new orthosis and pneumatic system, and to resolve them. To verify the functionality of the orthosis, the measured knee varus angle was compared before and after applying corrective force using the pneumatics bladders while fitted to the surrogate model using a goniometer.
Performance of the orthosis in vivo
The aim was to identify and analyse the range of frontal plane knee joint alignment that could be comfortably corrected into the device and also to analyse any alteration to active knee flexion range with the brace in situ. The thigh and leg portions were custom moulded for the subject individually and connected via the orthotic knee joints to match the subject’s corrected varus position during the non-weight-bearing casting. It was thought prudent to utilize a single volunteer subject initially to prove the structural integrity and corrective capability of the design prior to a future study involving a larger sample size.
Analysis of the corrective performance offered by the brace during static standing by the subject was achieved by analysing anterior/posterior (A/P) radiographs of the affected lower limb while she stood weight bearing as evenly as possible on both legs. The varus angulation was measured on the radiograph using a hand-held goniometer and following the centre line of the affected femur and tibia. During repeated tests, the accuracy of using a goniometer was shown to be repeatable. The angles were measured along bisectors of the mediolateral external contours of the thigh and lower leg. The lines so produced were kept on the dummy during addition of the orthosis and could still be measured. One person (orthotist) measured knee angle five times at each condition. The value reported in Tables 1 and 2 is a mean of five measurements.
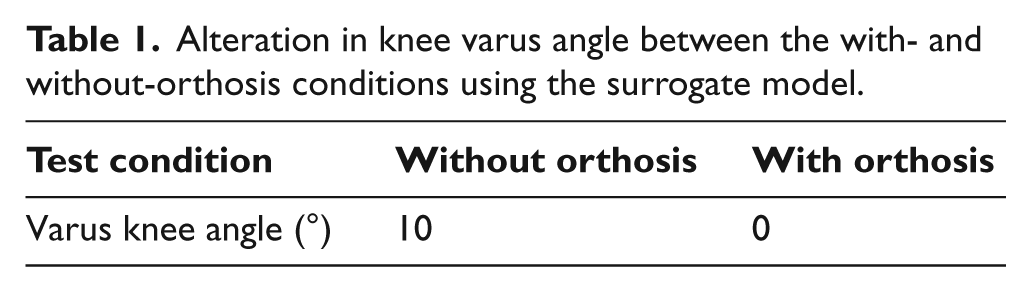
Alteration in knee varus angle between the with- and without-orthosis conditions using the surrogate model.
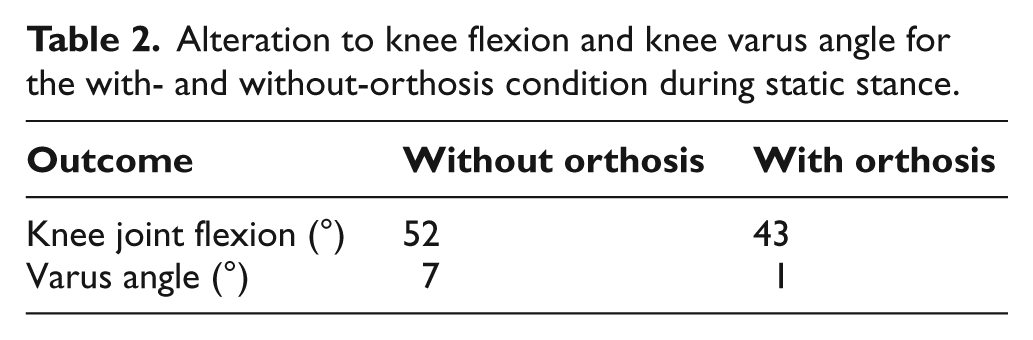
Alteration to knee flexion and knee varus angle for the with- and without-orthosis condition during static stance.
Results
Table 1 shows the knee varus angle measured between with- and without-orthosis conditions on the surrogate model. It can be seen that the varus knee angulation was reduced successfully to a neutral alignment with the new orthosis on the surrogate model.
Figure 4 shows the knee joint alignment with and without the orthosis during static standing. The orthosis reduced the varus rotational angle by 6°.
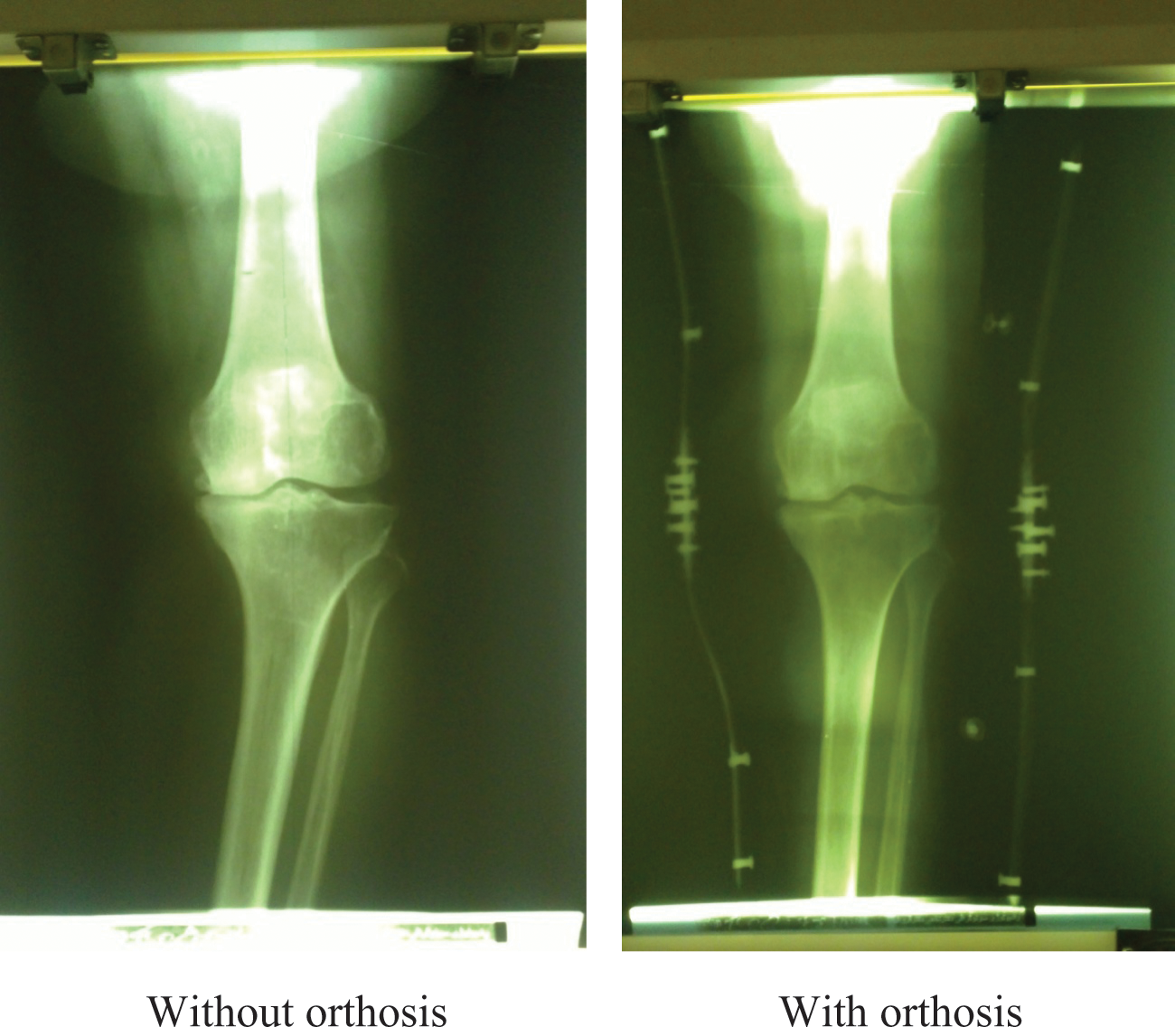
Frontal plane knee joint alignment with and without the orthosis during bilateral static stance.
The amount of active knee flexion attainable by the volunteer subject during static standing when wearing the brace was also compared to the without-brace condition while standing by being supported on the contralateral leg. It can be seen that the orthosis reduces knee flexion slightly when wearing the device.
Discussion
In this study, a new unloader knee orthosis, capable of applying a pneumatic adjustable corrective force for the purpose of altering knee joint alignment for patients such as those with medial compartment knee OA, is presented. A prototype of the novel orthosis was evaluated both with a surrogate model and with a single volunteer patient. The results demonstrated that the knee joint alignment during static standing was reduced and slightly less than that demonstrated during simulation testing.
The reduction in knee flexion possible when wearing the brace described in this study has also been demonstrated in previous publications when analysing the knee kinematics of patients wearing an unloader-type knee brace. Knee flexion was reduced by 9° when wearing the orthosis that is similar to previous gait research by Richards et al. 3 and Jones et al. 36 This may be important as adequate knee flexion is required for swing phase of gait. This could be attributed to friction within the orthotic knee joints and also obstruction of the superstructure and associated strapping posteriorly in preventing full knee flexion. Nevertheless, this gave the group confidence that the new orthosis could be used by subjects with medial compartment knee OA.
The frontal plane alignment with the newly developed orthosis indicated that it could feasibly be used for assisting in correcting the position of the knee joint for OA patients with grades 1, 2 and 3 medial and lateral compartment OA. The amount of inflation of the pneumatic components in this new orthosis may also be altered according to an individual’s characteristics, making the brace convenient to use. The brace adjustment was tailored for the subject used in this study according to her individual requirements, with the valgus angle of the orthosis superstructure set at a position that was both comfortable and acceptable for the subject.39,40 The main advantages of the currently developed orthosis were therefore the capability to provide an adjustable corrective force within the orthosis, while positioning the knee in an acceptable corrected position via the superstructure, and provision of a user-friendly design.
The key findings were that design and simulation of a bespoke knee unloader orthosis to combat the misalignment of medial compartment knee OA were achievable. The results show that partial correction of knee frontal plane alignment may be feasible when adapting a knee orthosis with pneumatic components such as those added to the thigh and leg shells in this study, albeit during static stance, and is worthy of further development. The authors were sufficiently encouraged by the static weight-bearing correction obtained within the brace, to feel confident that the design may offer a viable alternative to current designs in offloading the medial compartment of the knee.
The mean adduction moment value during normal gait is 3.3% of bodyweight times height. 41 This mean increases to 4.2% in patients with medial knee compartment OA.41,42 When the value of the adduction moment increases by 1%, values of the maximum reaction force on the medial compartment increase to 25% higher than normal. 11 Previous studies in this field have suggested that an increased adduction moment and malalignment of the lower extremity can cause pain and reduced function.43,44 A 20% increase in the peak adduction moment has also been shown to increase the risk of disease progression. 45 Studies have demonstrated that a valgus unloader orthosis is capable of reducing the adduction moment by 10% 46 and 13%. 47 However, this has not been correlated with the amount of valgus rotatory correction that may be expected. In this study, we only evaluated the performance of new orthosis in a static position but encouraging results in terms of the varus reduction were found, and one would hope that this would occur during free walking, but further research is needed to determine this.
As the unloader knee brace is light, there may also be long-term effects of wearing this brace in terms of comfort; maintenance of correction; alteration to quality of life, including long-term reduction in pain levels; and alteration to the degree of disease progression, all of which need to be determined in the future by a randomized controlled trial. The addition of long collateral shells, which were custom-made for the patient, linked with adequate internal padding and pneumatic translation away from the lateral aspect of the orthosis gave it the potential to overcome the shortcomings of the development of skin problems demonstrated by previous designs. The interface problems experienced from wearing previous orthoses evidenced in the literature could be overcome in this orthosis by redistributing loads and interface pressures over a wider area. The inflatable bladders would also add extra cushioning to the lateral aspect of the orthosis, and also reduce friction effects and reduce leg motion relative to the orthosis during wear.
It is therefore the intention to evaluate the efficacy of the new orthosis in providing appropriate reduction in the adduction moment for knee OA patients during walking trials, and a further study is therefore planned to assess the effect of this type of orthosis on gait parameters by unicompartmental knee OA patients and other comparative devices.
Limitations of the study
This was only a single-case study and therefore would not be valid for application of the results to a wider patient population. There may have been errors associated with using a hand-held goniometer to measure frontal plane angular data. However, strong concurrent validity has been previously found between hand-held goniometers and radiographs, as well as between hand-held goniometers and three-dimensional (3D) motion analysis in a systematic review when analysing psychometric properties of measurement tools for quantifying knee joint position and movement. 48 We did not evaluate user friendliness and comfort of orthosis use in this study. For further design of studies in this field, comfort level and user friendliness of the new orthosis can be evaluated with a specific questionnaire designed for this orthosis and by assigning the participants with a final score of the brace on a Visual Analogue Scale (0–10). The discussion on force distribution and interface problems and how they are addressed by this new knee orthosis is important and interesting. Future studies on this point will be beneficial in this field. The influence of limited gaps on the dummy at knee level and effect of it on the possible mediolateral position and correction angles was limitation of this study.
Conclusion
The new custom unloader knee orthosis showed proof of concept in providing standing assistance for medial compartment knee OA patients by adjusting the pneumatic components attached to the thigh and leg shells to produce a more neutral knee alignment. It has the potential to provide an alternative means of correcting malalignment of the knee for such patients, which needs to be confirmed following a large-scale clinical trial.
Footnotes
Conflict of interest
The authors have no conflict of interest in this study.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.