
Abstract
Isolated femoral condyle fracture is an uncommon entity. It accounts for only 0.65% of all femoral fractures, with lateral condyle involvement three times more frequently than the medial condyle. In neglected cases, nonunion and malalignment may occur, which results in osteoarthritis of the knee due to uneven distribution of load across respective compartments. In treating such cases, both osteoarthritis and nonunion have to be tackled to reconstruct a stable, mobile, pain-free, and well-aligned knee joint. There are a number of surgical options, including excision of the nonunion fragment, fixation of the nonunion fragment with or without bone graft, and total knee arthroplasty with or without stem extension. In the following, we present a case of 40-year non union of the lateral condyle and our rationale of management for a relatively young lady. During the course of treatment, there was an unexpected success even though arthroplasty was not performed. A management strategy for this challenging condition was also suggested.
Introduction
Isolated femoral condyle fracture, be it medial or lateral, is an uncommon entity. It accounts for only 0.65% of all femoral fractures, with lateral condyle involvement three times more frequently than the medial condyle. 1 In most developed countries, it is treated surgically with the aims of maintaining articular congruity and decreasing risk of fracture displacement. However, in neglected cases, nonunion and malalignment may occur, which results in osteoarthritis of the knee due to uneven distribution of load across respective compartments. 2,3
Patients with secondary osteoarthritis of the knee due to femoral condyle nonunion often complain of knee pain. Surgeons often find it challenging as both nonunion and osteoarthritis have to be tackled to reconstruct a stable, mobile, pain-free, and well-aligned knee joint. There are a number of surgical options, 4,5 including excision of the nonunion fragment, fixation of the nonunion fragment with or without bone graft, and total knee arthroplasty (TKA) with or without stem extension. Careful preoperative planning is essential to achieve a good surgical outcome. The patient should also be well informed of the procedure, associated risks, and complications so as to fulfill the patient’s expectation.
We present a case of the aforementioned condition and our rationale of management for a relatively young lady. During the course of treatment, there was an unexpected outcome in pain control for the lady. At the latest follow-up of 8 years after operation, the patient remained symptom free and was able to walk unaided even though arthroplasty was not performed as originally planned. The patient was informed that data concerning the case would be submitted for publication, and she consented.
Case report
A 57-year-old lady experienced left medial knee pain. She has a history of left knee injury during her teenage years, more than 40 years, which was left untreated. Throughout the years, she experienced increasing left knee pain, especially over the medial joint line. The pain was mechanical, which worsened on weight bearing. She could only tolerate level ground walking for 20 min with one cane. She needed to climb stairs with rail.
Physical examination of the left knee revealed no swelling or tenderness. The range of motion was from 10° to 100°. There was 20° genu varum. There was no collateral ligament laxity. Plain radiograph of the left knee showed nonunion of the medial femoral condyle fracture (Orthopaedic Trauma Association type 33B2) associated with tricompartmental osteoarthritis (Figure 1). 6 Computed tomography of the left knee confirmed the nonunion with proximal migration of the medial femoral condyle fragment (Figure 2). The medial femoral condyle fragment measured 35 × 35 × 50 mm3.
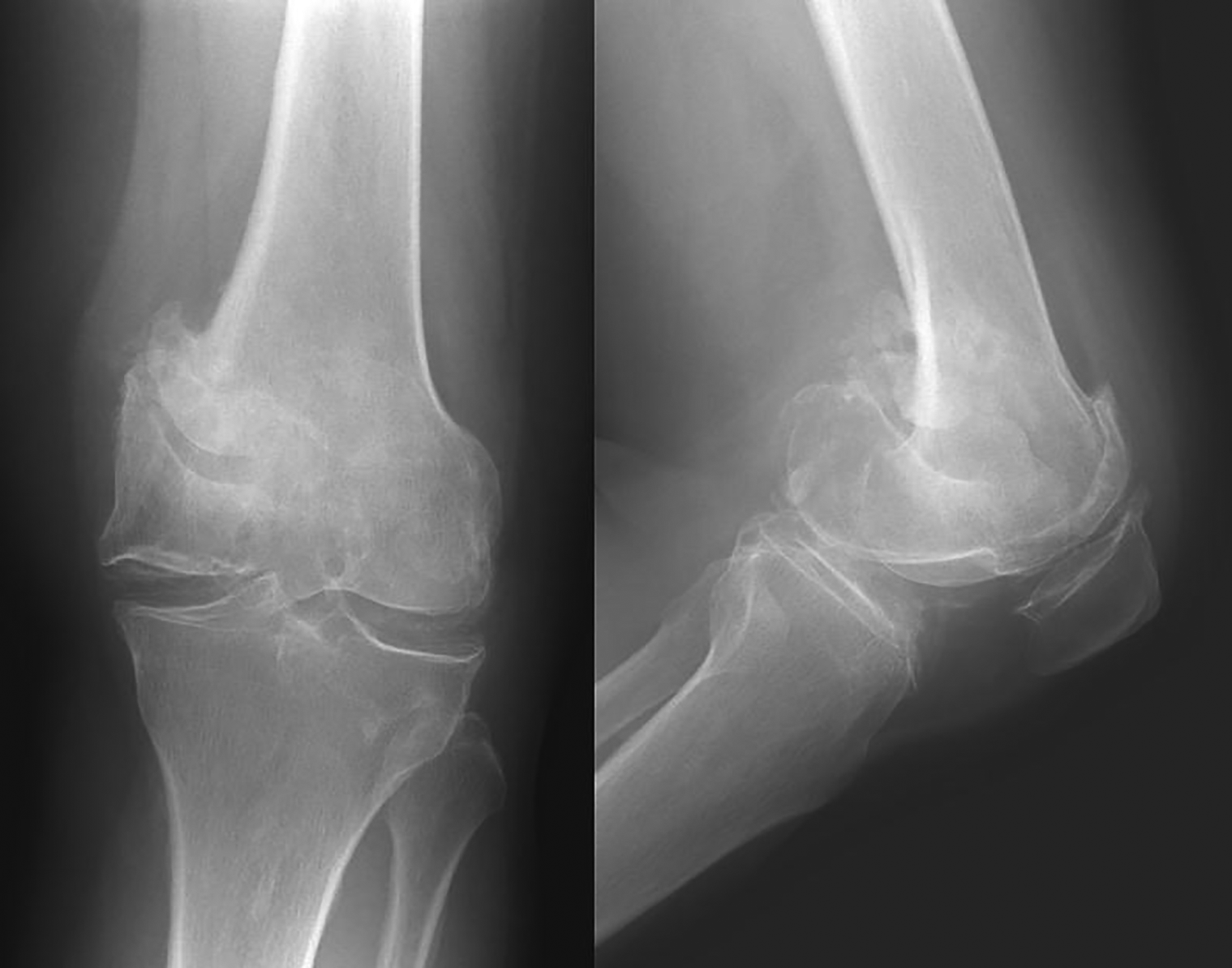
Radiograph showing medial femoral condyle nonunion and osteoarthritis of the knee.
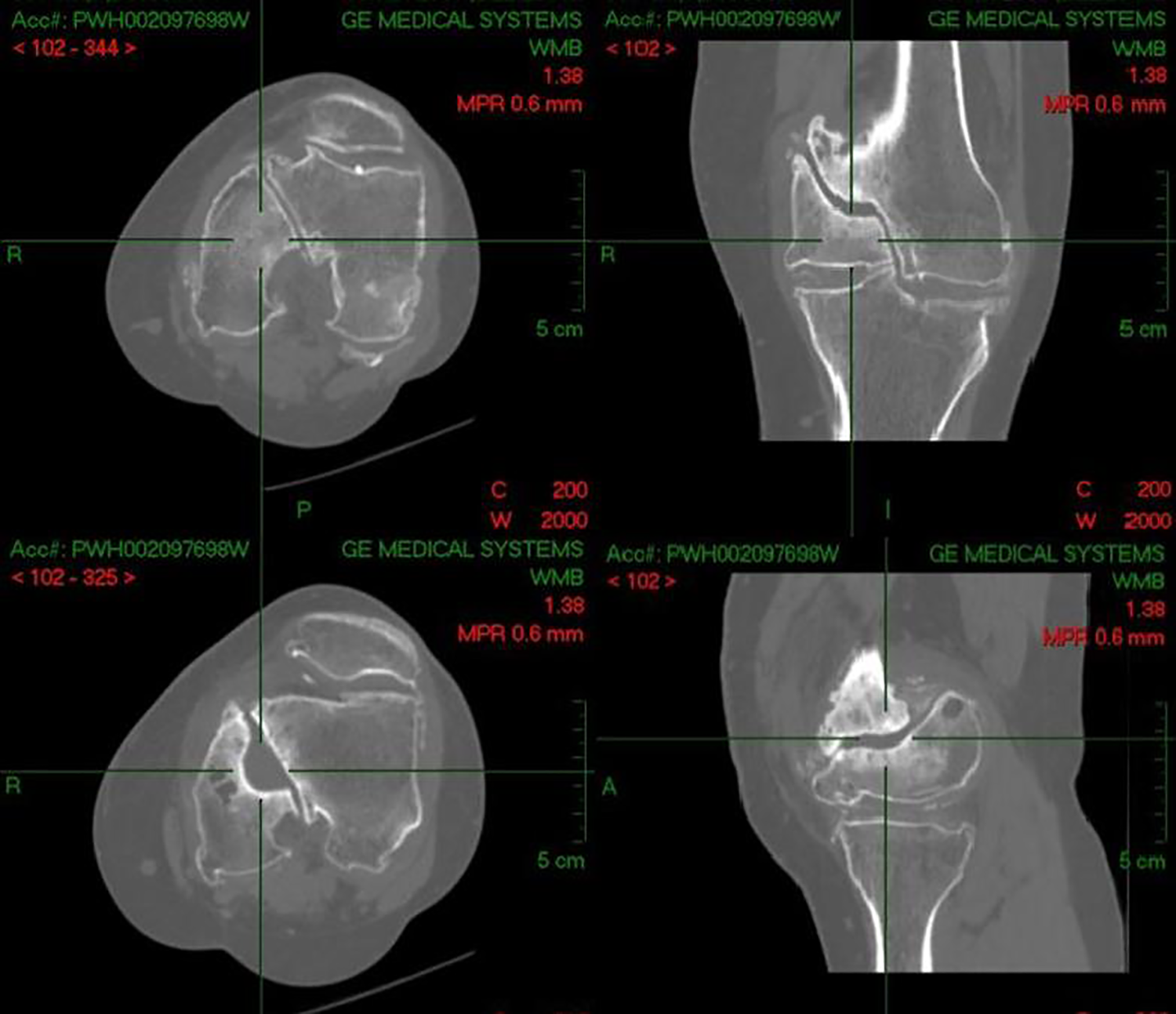
Computed tomography showing the nonunion.
Patient expected the treatment to alleviate her left knee pain so as to enhance her walking capacity. Nonoperative treatment with analgesics and physiotherapy was tried but failed to treat her symptoms. Surgical treatment was considered after failed conservative management. After a thorough discussion with the patient, a two-staged operation was planned. First stage fixation of medial femoral condyle nonunion was scheduled with the aims of preserving of original bone stock and achieving union of the medial femoral condyle fracture. This would be followed by a second-stage TKA after healing of the nonunion if there are significant residual symptoms as the patient was concerned with TKA-associated complications.
The first-stage operation was performed under general anesthesia. Midline incision was employed to facilitate the TKA in the later stage, followed by medial parapatellar arthrotomy for a better approach to the distal medial femoral condyle fracture fragment. The nonunion medial femoral condyle fragment was identified, and the sclerotic rim of the nonunion was debrided until there was healthy bleeding signifying well-vascularized bone. The nonunion fragment was reduced to its anatomical position and temporarily fixed with two guide pins. Autologous cancellous bone graft was harvested from the ipsilateral iliac crest and packed into the nonunion site. The nonunion fragment was then fixed with two 6.5-mm partially threaded cannulated screws with compression (Figure 3). Postoperatively, a long leg hinge brace was applied, allowing the knee free range of motion as pain tolerated. Protected weight bear regimen was commenced with nonweight bear walking for 4 weeks, followed by partial weight bear walking for 4 weeks more, and followed by weight bearing as tolerated. Computed tomography of the left knee at 5 months after the index operation confirmed the healing of medial femoral condyle fragment (Figure 4). At this juncture, her left knee pain had much improved. She could walk for more than 60 min without any walking aid. Lower limb long film revealed improved alignment of 20° genu varum to 10° genu varum (Figures 5 and 6). There was no bone graft donor site morbidity. She was very satisfied with the improvement in knee pain and function and the planned second stage of TKA was put on hold as she had minimal complaints and her quality of life was well maintained. She was then followed up regularly for monitoring of her symptom. Eight years after the operation, she only experiences minimal on and off symptoms similar to postoperative period and is able to walk unaided for at least 60 min. The initial plan of second-stage TKA was abolished indefinitely due to the significant improvement in symptoms with the patient’s expectation well met.
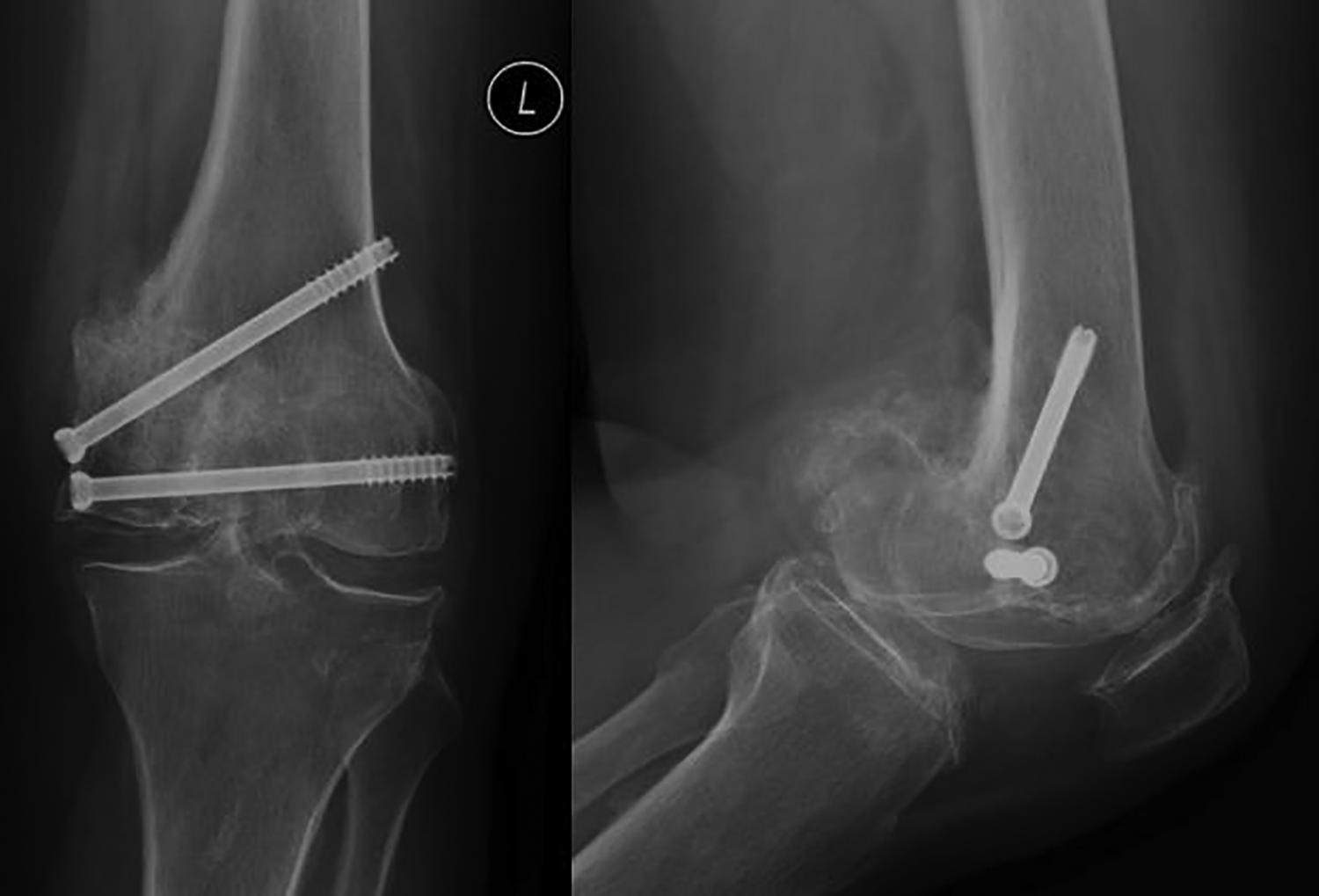
Radiograph showing fixation of the nonunion fragment.

Computed tomography showing the healed nonunion.
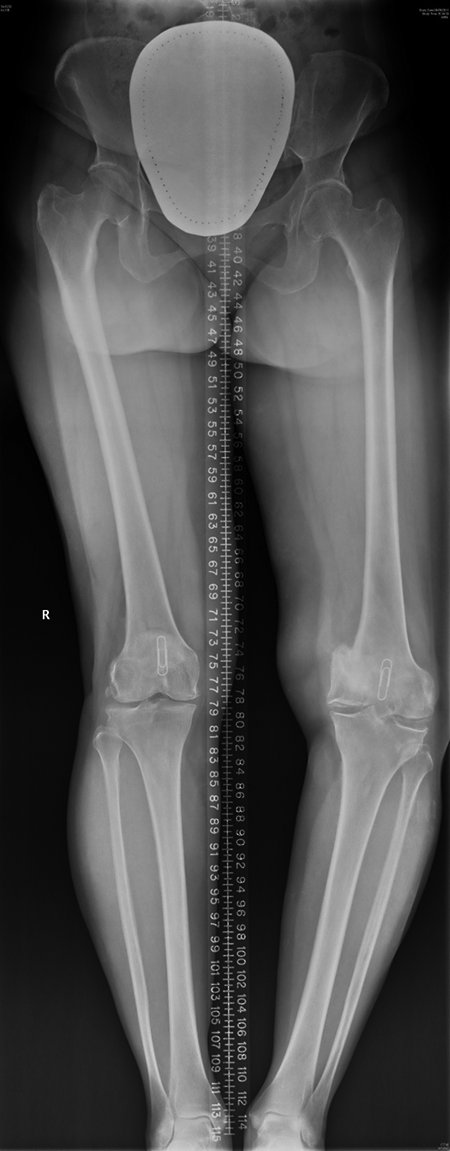
Preoperative lower limb long film showing the varus deformity.

Postoperative lower limb long film showing the improved left lower limb alignment.
Discussion
Isolated femoral condyle fractures are rare. Those with nonunion and complicated with secondary osteoarthritis are challenging cases for surgeons. Both nonunion and osteoarthritis need to be tackled to reconstruct a stable, mobile, pain-free, and well-aligned knee joint. There are a number of options to treat this challenging condition, 4,5 including (1) simple excision of small nonunion fragment with TKA, (2) staged fixation of nonunion fragment and TKA, (3) one stage fixation and TKA with stemmed prosthesis, (4) excision of nonunion fragment with femoral condyle strut allograft and TKA, (5) excision of nonunion fragment with metal augment and TKA, (6) excision of distal femur with total knee prosthesis–allograft composite, and (7) excision of distal femur and replaced with total knee megaprosthesis.
Due to the low incidence, the number of cases of femoral condyle nonunion complicated with secondary osteoarthritis of knee is scanty in the current literature. Most of the series presented mixed nonunion cases around the knee, with majority involving the supracondylar region rather than isolated femoral condyle region. Jiang et al. reported a case of a 27-year nonunion Hoffa fracture in a 46-year-old patient, who presented with progressive pain and swelling. It was treated with open reduction and internal fixation with augmentation by bone graft. Results were satisfactory with the patient able to fully bear weight with a full range of motion with no ligamentous instability. 7 Kress et al. reported five cases of femoral supracondylar nonunions, 8 with two cases involving a native knee joint, treated with TKA with an uncemented pressfit intramedullary rod and bone grafting. All achieved union within 6 months. Papadopoulos et al. reported the result of TKA following prior distal femoral fracture, with 3 of the 48 knees being nonunion cases. 9 Long stem cemented femoral component and bone grafting were used. Femoral component revision was required in one knee 18 months after the index operation due to the dissociation of the modular stem. Megaprosthesis had been implanted to replace the supracondylar nonunion fragment in a number of series. 10 –13 Good results were reported in two patients by Davila et al., 10 four of five patients by Freedman et al., 11 and all eight patients by Vaishya et al. 12 All authors suggested its exclusive use in elderly patients with osteopenic bone and difficult bony reconstruction or failure to achieve bony union despite multiple surgeries. Haidukewych was the only author, who reported the treatment of isolated femoral condyle nonunion with TKA. 5 Three of his 17 nonunion cases were unicondylar, with lateral femoral condyle in two cases and medial femoral condyle in one case. One lateral condyle nonunion was managed with resection of the nonunion fragment and use of a total condylar femoral component (Johnson & Johnson, USA) with a distal augmentation and an allograft strut. Another lateral nonunion was managed with complete resection of the nonunion fragment and the use of a geometric prosthesis. The medial condyle nonunion was managed with internal fixation with cancellous screws and use of a posterior stabilized pressfit condylar prosthesis (Johnson & Johnson). The 5-year survivorship of his cohort with aseptic failure as end point was 91%. As seen from the above, there have been various management strategies suggested to tackle this scenario with various outcomes.
In our present report, staged operation with fixation of medial femoral condyle nonunion, followed by TKA after healing of the nonunion fragment, was initially planned. Our patient was 57 years old at the time of operation, a relatively young age for TKA. There were two main concerns. First, preservation of bone stock, as we hope the patient is able to keep as much of her native bone as possible, and second, timing of TKA. Revision surgery is expected in patients who have undergone arthroplasty and given her young age, we would hope to delay the timing of surgery as much as possible so as to reduce the number of revisions the patient may have to undergo.
In the first stage, we preferred to fix the nonunion fragment and realign the lower limb as it is known that realignment to a more anatomical axis may redistribute the loads across the knee joint leading to less imbalance thus less pain for the patient. During the operation, the nonunion fragment was intentionally pulled distally and fixed in anatomical position. This aimed at improving the varus malalignment but not total correction as this was planned to be done at the second-stage arthroplasty. The improvement in the varus malalignment, however, helped to offload the medial compartment, which decreased the knee pain. In addition, this also prevented medial soft tissue contracture, which decreased the chance of requiring constrained and stemmed prosthesis in the second-stage TKA of which may complicate future revision surgeries. A two-staged operation was also preferred, as single-stage operation required the use of stemmed prosthesis to protect the fixation of the nonunion fragment, which will complicate revision surgeries in long run. In contrast, routine TKA prosthesis can be utilized if second-stage operation is required, provided there is a union of the femoral condyle fragment. Also, any complication of fixation of the condyle fragment in the single-stage operation will jeopardize the function of the TKA leading to unnecessary need for revision. As for the fixation of the nonunion fragment, screw fixations were preferred over plate fixation. This was in consideration of avoiding usage of stemmed TKA prosthesis, which was essential to bypass the stress riser after plate removal in the second-stage operation. However, as the pain relief was so satisfactory after the first-stage operation, the patient declined TKA, and thus, all associated risks and complications of TKA were foregone. Retrospectively, it can be considered in such cases that fixation of the nonunion fragment be a definitive treatment and TKA as a follow-up plan if fixation of the nonunion fragment fails to alleviate the symptom.
Overall, in managing osteoarthritis of the knee associated with femoral condyle nonunion, a number of factors need to be considered during the preoperative planning, including the age of the patient, premorbid activity level, bone quality and healing potential, and the location and size of the fracture fragment. In addition, the condition of the surrounding soft tissue, history of infection, and the presence of retained internal fixation devices also needed to be addressed. Identifying the underlying cause of nonunion is also important. In reviewing our management of this lady’s condition, there are several factors, which we may pay attention to. First, it would be important to delineate the source of the knee pain, whether it is from the nonunion site or is it due to secondary osteoarthritis. This can be assessed by factors, such as clinically whether the nonunion fragment is mobile, exaggerated pain on weight bearing, and intrinsic conditions of the knee joint; radiologically, whether the affected joint has a high degree of osteoarthritic changes and also by comparing with the other knee. Second, fixation of the nonunion fragment should be considered if the patient is young as native bone stock is of utmost importance in this group of patients. It should also be considered whether fixation of nonunion fragment will lead to significant improvement in alignment of the lower limb axis. Third, if there are significant osteoarthritic changes in the other compartments of the knee, TKA may have to be considered as it should be regarded that fixation of nonunion fragment alone may not be able to improve the overall osteoarthritic condition. In such scenarios, if the nonunion fragment is small and does not bear the collateral ligament, nor does it jeopardize the bony support for the femoral component of the TKA, excision of the fragment and TKA with routine prosthesis can be employed. Otherwise, preservation or replacement of the nonunion fragment is required. For young patients, we should be aware that the bone stock should be preserved, but the ability to cooperate with postoperative protected weight bearing is the prerequisite. Fixation of the native femoral condyle and augmentation with autologous bone graft are preferred, which preserve both the bone stock and collateral ligament stability. Fixation and TKA can be done as single-stage or two-stage, with the advantages of two-stage operation, as discussed above. The use of allograft with knee prosthesis should be reserved for young patients with failed fixation of the nonunion fragment and poor bone stock. For older patients, pain relief, avoidance of prolonged immobilization, and immediate weight bearing are preferred so as to facilitate rehabilitation. Therefore, distal femoral excision with TKA using megaprosthesis can be considered. However, expertise in TKA with megaprosthesis is needed, and the revision of megaprosthesis will be extremely difficult. So, the use of megaprosthesis should be reserved for older patients with limited life expectancy.
In conclusion, reduction and fixation for the nonunion fragment of femoral condyle fractures should be considered. TKA can be considered as a follow-up plan if the initial management of reduction and fixation fails.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.