
Abstract
Objective
To compare the clinical outcomes of locking compression plate (LCP) and distal femoral replacement (DFR) for periprosthetic distal femoral fractures (PDFFs) after total knee arthroplasty.
Methods
This retrospective study identified patients with PDFFs in an institutional database between January 2012 and December 2021. Demographic data and clinical outcomes, including postoperative complications, reoperation, 1-year mortality, Knee Society Scores (KSS) and Knee Society Functional Score (KSFS) were analysed.
Results
In total, 12 patients treated with LCP and six patients treated with DFR were included. There was no significant difference between the LCP and DFR groups in terms of postoperative complications (25.0% versus 33.3%, respectively), reoperation (8.3% versus 0.0%), respectively, 1-year mortality (8.3% versus 16.7%, respectively) or mean ± SD KSS (80.3 ± 8.3 versus 78.0 ± 2.5, respectively). However, the mean ± SD KSFS was significantly better for patients with LCP than for those with DFR (51.8 ± 12.5 versus 37.0 ± 6.7, respectively).
Conclusion
DFR provides similar clinical outcomes compared with LCP for PDFFs. Patients with advanced age may benefit from DFR to allow early weight bearing.
Keywords
Introduction
With the ageing of the population and increased demand for patients to remain active, the number of total knee arthroplasties (TKA) is growing annually.1–3 Subsequently, periprosthetic distal femoral fractures (PDFFs) after TKA have become more common, with an incidence of 0.3%–3.5%.4–6 However, treatment for PDFFs is challenging due to osteoporosis, limited bone stock and medical comorbidities. 7 Generally, internal fixation with a locking compression plate (LCP) or retrograde intramedullary nailing (RIMN) is recommended for fractures with stable implants and adequate bone stock, and distal femoral replacement (DFR) is considered a salvage option for those with loose components or extreme distal comminutions.8,9
To date, whether to fix or revise PDFFs remains controversial. Recent evidence supports DFR as a preferred option for PDFFs owing to its advantages, including early weight-bearing and independence of fracture healing.10–12 However, the disadvantages of DFR include a lack of revision options and higher costs. 13 Currently, there is a paucity of direct comparative studies on internal fixation and DFR for PDFFs.
Thus, a retrospective study was undertaken to compare internal fixation with LCP and DFR for PDFFs after primary TKA. The primary outcome was postoperative complications. The secondary outcomes included surgical time, intraoperative transfusion volume, reoperation, 1-year mortality and functional score. The current study hypothesized that DFR could offer outcomes comparable with those of LCP for patients with PDFFs.
Patients and methods
Study population
This retrospective study consecutively enrolled all patients diagnosed with PDFFs in the Department of Orthopaedics, The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu Province, China between January 2012 and December 2021 that were identified through the electronic medical record database. The inclusion criteria were as follows: (i) patients with PDFFs after primary TKA; (ii) patients that underwent surgery with either LCP or DFR; (iii) patients with a minimum follow-up of 12 months.
This retrospective study was approved by the Institutional Research Ethics Board of The First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu Province, China. Written informed consent was obtained from all patients prior to surgery and verbal informed consent was obtained when patients were contacted for follow-up.
Data collection
All fractures were classified according to previously published classification systems.14,15 The plates for fixation were from Synthes (Oberdorf, Switzerland) and Zimmer Biomet (Warsaw, IN, USA). The DFR prostheses were provided by Lidakang (Beijing, China). Demographic data, including sex, age, diagnosis of primary TKA, time from TKA to fracture, mechanism of injury, time from fracture to surgery and American Society of Anesthesiologists (ASA) score were collected from the electronic medical record database. Surgical time and intraoperative transfusion volume were reviewed using electronic operative recordings. Postoperatively, active knee movement was encouraged for all patients, and weight-bearing, as tolerated, was allowed for patients with DFR on the second day. Patients with LCP began partial weight-bearing 4 weeks after surgery. Clinical and radiographic examinations were routinely performed at 1, 3, 6 and 12 months postoperatively. Complications, any cause of reoperation, and 1-year mortality rates were recorded. At the final follow-up, functional outcomes were evaluated using the Knee Society Score (KSS) and Knee Society Functional Score (KSFS). 16 Patients that failed to visit the clinic were followed-up by telephone.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., Armonk, NY, USA). An independent-samples t-test was used for continuous data and Pearson’s χ2-test was used for categorical data. A P-value <0.05 was considered statistically significant.
Results
This retrospective study identified 18 patients with PDFFs after primary TKA, 12 of whom were treated with LCP (Figure 1) and six with DFR (Figure 2). The mean age of the total cohort was 70.8 years (range, 42–85 years) and there were 16 women and two men (Table 1). In terms of fracture classification, there were 12 Rorabeck-Taylor type II fractures, three Su type I fractures, seven Su type II fractures and two Su type III fractures in the LCP group; and two Rorabeck-Taylor type II fractures, four Rorabeck-Taylor type III fractures, one Su type II fracture and five Su type III fractures in the DFR group. The DFR group had a significantly higher ASA score (P = 0.001) and a significantly longer time from fracture to surgery (one patient treated with DFR at 378 days after fracture for symptomatic nonunion was excluded, Figure 3) compared with the LCP group (P = 0.0002). No significant differences were found between the two groups in the cause of primary TKA, time from TKA to fracture, follow-up duration or mechanism of injury.

A 74-year-old female patient included in a study to compare internal fixation with locking compression plate (LCP) and distal femoral replacement for periprosthetic distal femoral fractures after primary total knee arthroplasty was treated with LCP: (a, b) preoperative anteroposterior and lateral radiographs and (c, d) anteroposterior and lateral radiographs at 10 months postoperatively.

A 65-year-old female patient included in a study to compare internal fixation with locking compression plate and distal femoral replacement (DFR) for periprosthetic distal femoral fractures after primary total knee arthroplasty was treated with DFR for extremely distal comminution: (a, b) preoperative anteroposterior and lateral radiographs and (c, d) postoperative anteroposterior and lateral radiographs.
Demographic and clinical characteristics of patients (n = 18) included in a study to compare internal fixation with locking compression plate (LCP) and distal femoral replacement (DFR) for periprosthetic distal femoral fractures after primary total knee arthroplasty (TKA).
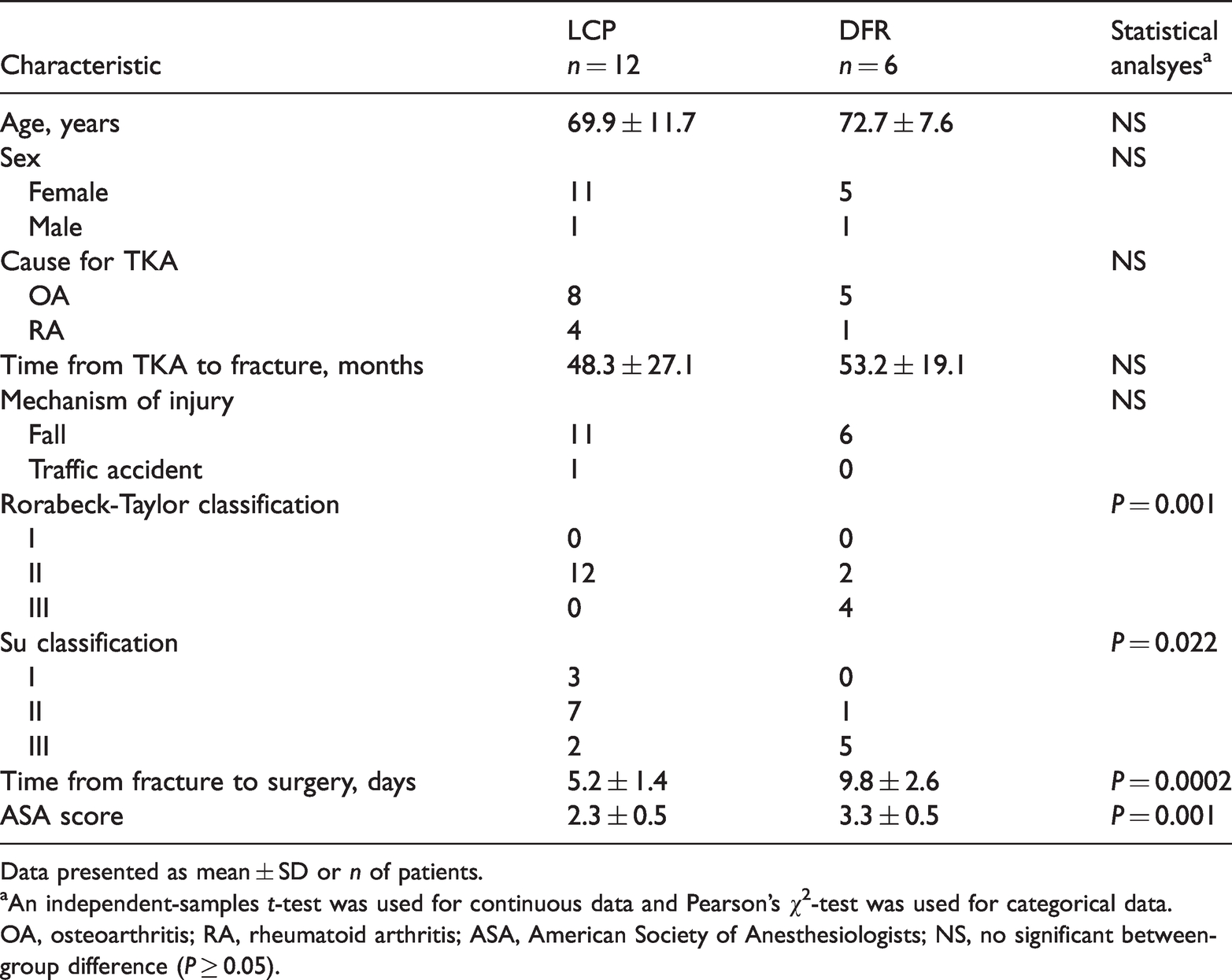
Data presented as mean ± SD or n of patients.
aAn independent-samples t-test was used for continuous data and Pearson’s χ2-test was used for categorical data.
OA, osteoarthritis; RA, rheumatoid arthritis; ASA, American Society of Anesthesiologists; NS, no significant between-group difference (P ≥ 0.05).

A 64-year-old female patient included in a study to compare internal fixation with locking compression plate and distal femoral replacement (DFR) for periprosthetic distal femoral fractures after primary total knee arthroplasty underwent conservative treatment initially and was treated with DFR at 378 days after injury for nonunion: (a, b) preoperative anteroposterior and lateral radiographs and (c, d) Postoperative anteroposterior and lateral radiographs.
The surgical time was longer in the DFR group, but the difference was not significant (Table 2). Patients with DFR received significantly higher intraoperative transfusion volume than those with LCP (P = 0.024). In the LCP group, infection occurred in two patients, one of whom required debridement; and one patient experienced implant failure but refused reoperation. There were two complications in the DFR group, including one infection (treated effectively by oral antibiotics) and one deep vein thrombosis. There was no significant difference between the LCP and DFR groups in terms of postoperative complications, reoperation and 1-year.
Clinical and surgical outcomes of patients (n = 18) included in a study to compare internal fixation with locking compression plate (LCP) and distal femoral replacement (DFR) for periprosthetic distal femoral fractures after primary total knee arthroplasty (TKA).

Data presented as mean ± SD or n of patients (%).
aAn independent-samples t-test was used for continuous data and Pearson’s χ2-test was used for categorical data.
KSS, Knee Society Score; KSFS, Knee Society Functional Score; NS, no significant between-group difference (P ≥ 0.05).
At 1-year postoperation, there was no significant difference in the KSS between the LCP and DFR groups (Table 2). However, the KSFS was significantly better for patients with LCP than for those with DFR (P = 0.027).
Discussion
The treatment of PDFFs aims to restore function with the lowest possibility of complications. In this current retrospective study, patients with DFR showed a significantly higher facture complexity and ASA score but comparable postoperative complications, reoperation, 1-year mortality and KSS as those with LCP. In addition, higher intraoperative transfusion volume and lower KSFS were found in patients treated with DFR compared with those treated with LCP.
Similar outcomes have been reported previously. For example, a retrospective analysis of 39 internal fixation cases with stable prosthesis and 29 re-arthroplasty cases with loose prosthesis found no significant difference between the treatment groups regarding satisfaction, status of ambulation, complications, reoperation or mortality. 17 A retrospective review of 35 patients with LCP and 23 patients with DFR reported no difference in mortality, complications or ambulatory status at the 1-year follow-up. 18 Their postoperative rehabilitation protocol was similar to that used for the current patients, which allowed immediate weight-bearing for patients with DFR, but only touchdown weight-bearing or non-weightbearing within 6–8 weeks for those with LCP. 18 Equivalent mortality and complication rates for PDFFs were demonstrated in patients treated with either LCP or DFR. 19 These authors suggested fracture location, distal bone stock, patient mobility and current comorbidities as treatment guidelines. 19 However, details of the fracture classification were not reported in their study. 19 This current study found more complex fractures (Rorabeck-Taylor type II, Su type III) in the DFR group, but they did not affect the outcomes, although the sample size was relatively small. Regarding functional scores, a previous showed similar KSS between LCP and DFR but better KSFS for LCP, 20 which was consistent with the current findings. In our opinion, the older age and higher ASA score were responsible for the significantly worse KSFS in the DFR group, which led to a longer time from fracture to surgery in the current study. In addition, a recent meta-analysis also failed to identify the optimal treatment for PDFFs because there was no difference in major complications or reoperations between LCP, RIMN and DFR. 21
Controversy over fixation versus revision has mainly focused on low PDFFs. 22 A systematic review of low PDFFs revealed a lower reoperation rate and earlier weight-bearing but slightly worse knee function with DFR. 23 A retrospective cohort study of 60 low PDFFs, including 40 Su type II and 20 Su type III fractures, found that patients with DFR underwent fewer reoperations and had better 5-year survivorship than those with LCP. 24 However, the authors admitted that reoperation after DFR was complex and suggested particular caution when using DFR for patients with greater life expectancy. 25 Another finding of their study was that reoperation following LCP was associated with medial comminution. 26 Therefore, the double-locking plate technique may be a viable option in this situation. A previous study reported excellent function (KSS 94 and KSFS 89.5) and fewer complications for very low PPDFFs using double-locked plating. 27 In addition, dual plating with minimal invasion or intramedullary fibular strut allograft has shown satisfactory outcomes.26,27 However, these were observational studies without control groups. Further research comparing the double-locking plate and DFR for low PDFFs is required.
This current study had several limitations. First, it had a retrospective design. Secondly, the sample size was limited. Procedures conducted by different surgeons may also have led to bias. Thirdly, the costs associated with each procedure were not included, which obviously affects decision making. Finally, the duration of follow-up was relatively short and the functional scores assessed through telephone interviews in some patients may have influenced the reliability and accuracy of the results.
In conclusion, DFR allowed earlier weight-bearing and showed similar outcomes as those of LCP for PDFFs in terms of complication, reoperation, 1-year mortality and KSS. However, patients with DFR underwent more intraoperative transfusions and had worse KSFS. Well-designed studies with larger sample sizes are required to identify the optimal treatment for PDFFs.
Footnotes
Author contributions
Peng Fu was responsible for the data collection and manuscript preparation. Zhenzhen Gao and Song Zheng were responsible for data analysis and manuscript preparation. Wenwei Liang was responsible for data analysis. Weimin Fan was responsible for manuscript preparation.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors.