
Abstract
Multiple fractures of the femur, defined for the purposes of this study as the association of three or more non-contiguous fractures on the same bone segment, is an exceedingly rare condition with an unknown incidence in the literature. A limited number of studies, mainly consisting of case reports or small case series, have addressed this topic, and no shared consensus or guidelines exist on what the ideal timing and sequence of multiple fracture fixation is. The present paper reports the clinical case of a 36 years old man who sustained a blunt chest injury, a non-concussive head injury, a displaced intracapsular fracture of the left femur (AO 31B2), a left diaphyseal multifragmentary fracture (AO 32B3), a supradiacondylar fracture of the distal end of the left femur (AO 33C1.1), a Hoffa fracture of the lateral left femoral condyle (AO 33B3.2 f), and a multifragmentary fracture of the left patella with bone loss (AO 34C3) due to a vehicular high-energy trauma. The patient was surgically treated by open reduction and internal fixation according to a proposed algorithm of treatment and reported excellent clinical and radiological outcomes at 32 months follow-up. The primary aim of this study is to describe our experience in the treatment of such complex fractures, by presenting our clinical and radiological results, and to propose a treatment algorithm. The secondary aim is to provide a comprehensive review of the literature on this topic.
Background
Multiple fractures of the femur, defined for the purposes of this study as the association of three or more non-contiguous fractures in the same bone segment, is an exceedingly rare condition whose incidence has not yet been reported in the literature. Limited data on the surgical treatment and clinical outcomes exist, especially when dealing with complication rate and need for revision surgery. Besides, a poor knowledge on the causal mechanism of lesion is present in the literature. Although several traumatic mechanisms have been reported, there is no agreement on what is the position of the limb at the moment of the trauma that may cause such fracture pattern.1,2 This injury pattern, which has been associated with high-speed vehicular accidents or major trauma due to high-energy mechanisms,1–4 poses a unique challenge for the treating surgeon because the choice of surgical device and the fixation sequence for each of the fractures is critical.
Although a limited number of studies, consisting mainly of case reports1,4 or small clinical series,2,3,5 have been published on this topic, none has proposed a clear algorithm to define the timing, the fixation sequence, and the type of surgical device to be used depending on all the possible fracture pattern combinations. It should in fact be borne in mind that fixation devices that might be suitable for the treatment of an isolated fracture may be incompatible in this scenario. The aim of the present study was: (1) to describe our clinical and radiological experience and results in the treatment of multiple fractures of the femur (one case reported), (2) to propose a therapeutic algorithm for the timing, fixation sequence, and fixation devices to be used according to the fracture pattern and to the patient’s clinical conditions, and (3) to perform a qualitative review of the literature on this topic.
Case presentation
A 36-year-old male patient sustained a high-energy vehicular accident with frontal impact while driving his car. The patient sustained a blunt chest injury, a non-concussive head injury, a displaced intracapsular fracture of the left femur (AO 31B2), a left diaphyseal multifragmentary fracture (AO 32B3), a supradiacondylar fracture of the distal end of the left femur (AO 33C1.1), a Hoffa fracture of the lateral left femoral condyle (AO 33B3.2 f), and a multifragmentary fracture of the left patella with bone loss (AO 34C3) (Figure 1) (Table 1). There were no open fractures. The AO classification 6 was used to classify the observed fractures, while the Oxford Knee Score 7 and the Harris Hip score 8 were used to assess the clinical function of the patient. The injury severity score (ISS) 9 was 36 at the time of admission. Owing to the patient’s conditions, an emergency surgical procedure was performed within 3 h of the patient’s admission. On a traction table, the displaced intracapsular fracture was reduced and fixed with three 6.5-mm cannulated screws (Synthes), according to the standard positioning technique. An external fixator with a femoral-tibial configuration was applied to the left limb and the patient was sent to the intensive care unit because he was considered ineligible for an early total care protocol. After 5 days, the definitive surgical intervention was performed by adopting an anterolateral knee approach on a traction table with proximal lateral extension, using the universal bone distractor device as a reduction tool. The Hoffa fracture was first reduced with a fully-threaded 3.5-mm cortical screw (Synthes) and the femoral condyles were fixed with two 6.5-mm cannulated screws (Synthes) positioned outside the planned location of the femoral plate. An 11-hole less invasive stabilization system (LISS) 4.5-mm Locking Compression Plate (LCP) plate (Synthes) was then placed after open reduction and temporary stabilization of the supracondylar fracture, followed by an indirect reduction of the diaphyseal fracture obtained by means of the universal distractor device. Finally, by using the same anterolateral knee approach, the patella was fixed by a dynamic tension band wiring technique, free 1.8 K wires for small fragments and a non-absorbable wire circumferential cerclage (Figure 2). No ligamentous lesions were observed at the moment of the surgical treatment nor were any meniscal tears detected. The post-operative period was uneventful and the patient was discharged 10 days after the injury and was instructed to avoid weight bearing on the lower left limb and to perform passive knee flexor-extension exercises within a controlled range for the first 15 days, followed by active exercises. The fracture healed with no complications; the diaphyseal fracture of the femur was the last to show a valid callus at 6 months. At 16 months, the patient underwent patellar tension banding removal following complaints related to prominent hardware and discomfort; a prominent free intercondylar cannulated screw and distal LISS screws were also removed in that surgical procedure (Figure 3). No complications were observed.
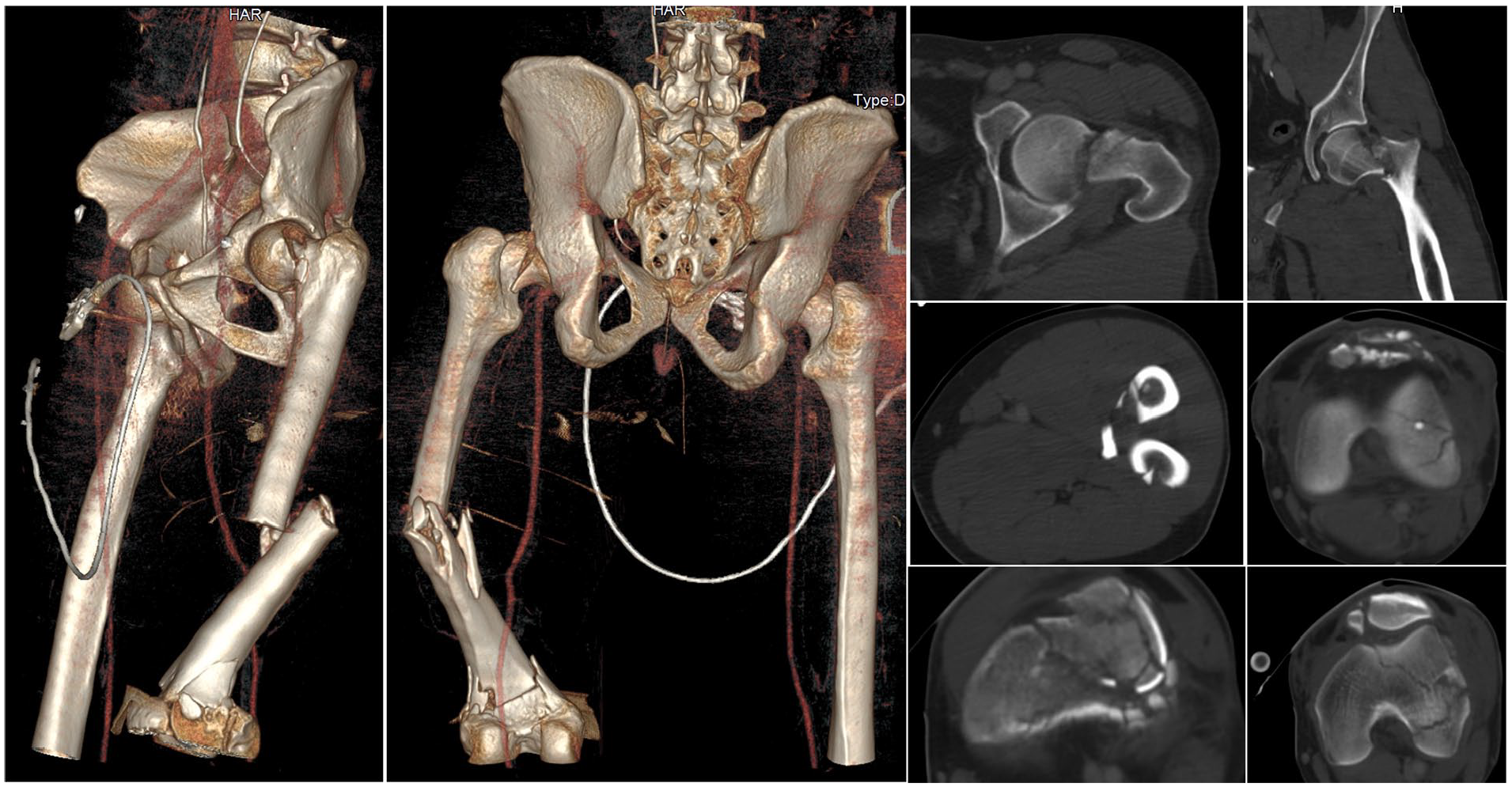
The figure shows the combination of multiple non-contiguous fractures of the left femur: displaced intracapsular fracture of the left femur (AO 31B2), a left diaphyseal multifragmentary fracture (AO 32B3), a supradiacondylar fracture of the distal end of the left femur (AO 33C1.1), a Hoffa fracture of the lateral left femoral condyle (AO 33B3.2 f), and a multifragmentary fracture of the left patella with bone loss (AO 34C3).
Demographic data, trauma mechanism, fracture pattern, fixation sequence, and devices.

DCO: damage control orthopedics; ISS: Injury Severity Score; LISS: less invasive stabilization system; ORIF: open reduction internal fixation.
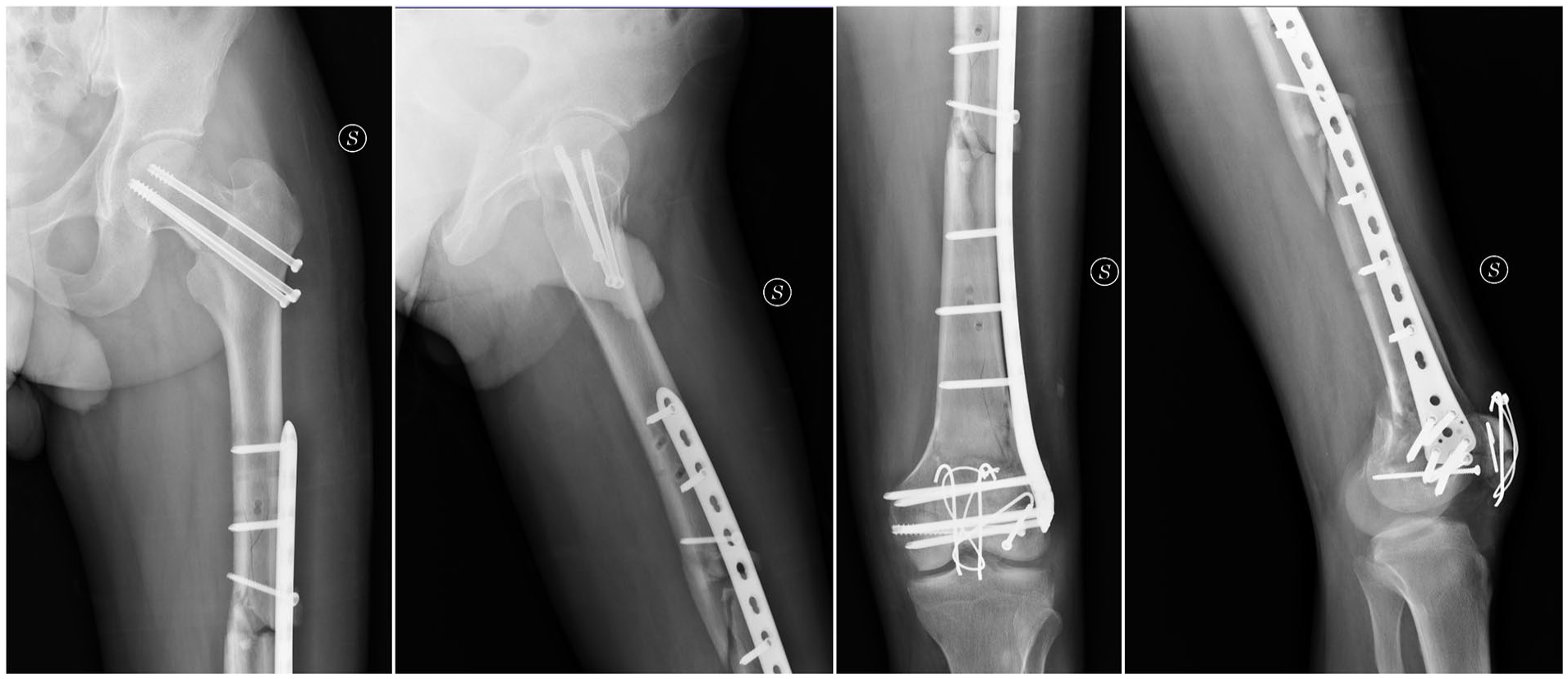
The post-operative X-ray: an 11-hole less invasive stabilization system plate and screws, a 3.5-mm anteroposterior screw, 6.5-mm cannulated screws for the femoral neck, and intercondylar fracture fixation were used.

The figure shows the fractures healing and the removal of the patellar tension banding cerclage wire, condylar cannulated screws, and distal less invasive stabilization system condylar screws.
All the fixation devices were removed at 24 months. At the 32-month follow-up, the Oxford Knee Score was 48 and the Harris Hip Score was 96, the patient presented no avascular necrosis of the femoral head, walked without crutches and had a full knee range of motion (ROM) (0°–135°) and full hip ROM (Figure 4) with no signs of knee instability. No radiological signs of degenerative arthritis were observed at the last X-ray examination of the knee joint and all the fractures healed uneventfully. (Figure 5). A written informed consent was obtained by the patient involved in this study.
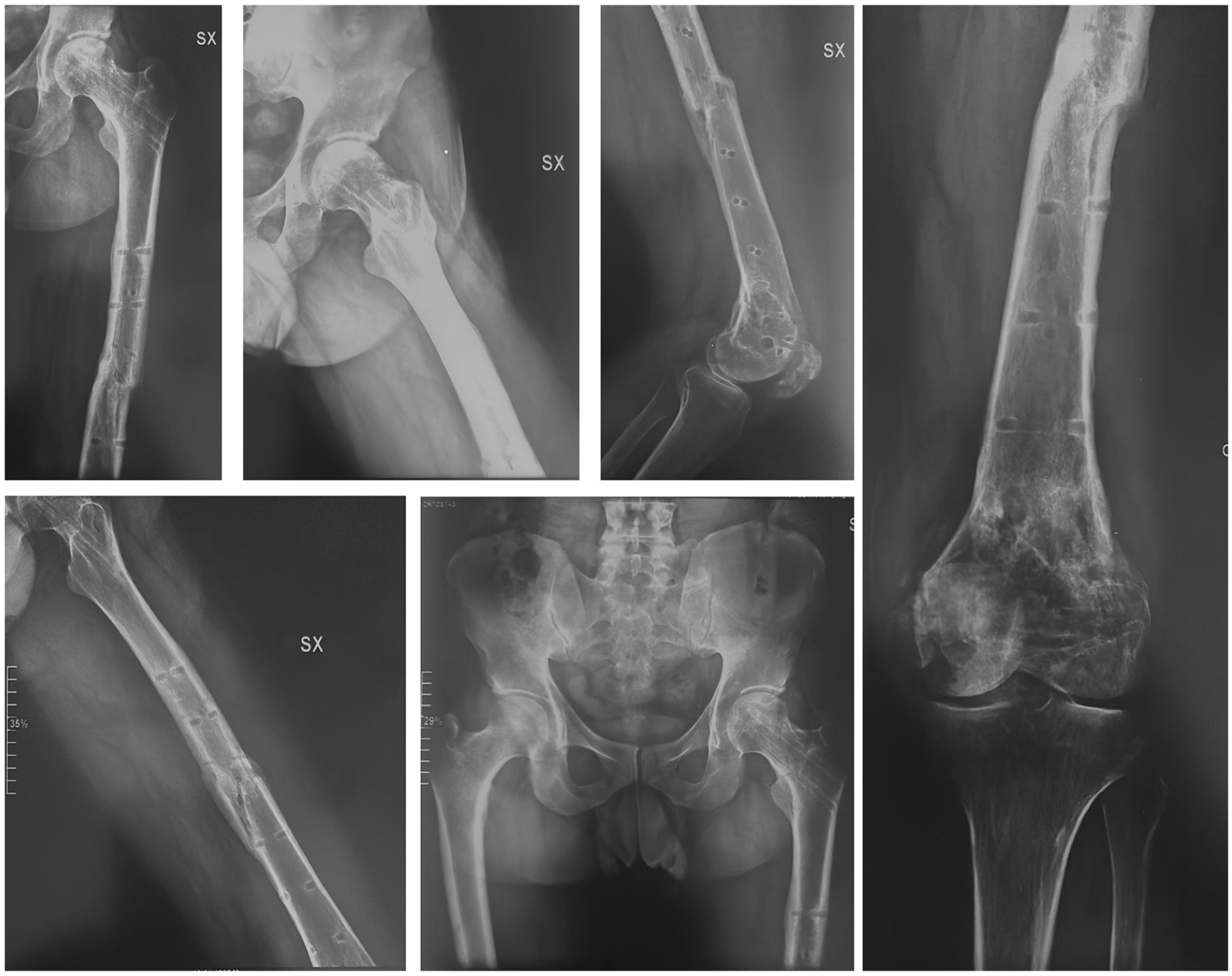
The figure shows the X-rays after hardware removal 24 months after the original trauma.

Clinical results at the last follow-up visit (32 months).
A qualitative literature review with no temporal limits was performed using the MEDLINE database (PubMed) and Google scholar platform. The following inclusion criteria were used: studies reporting on the clinical and radiological results of patients treated for multiple non-contiguous fractures of the ipsilateral femur; English language; and indexed journal. The following exclusion criteria were applied: lack of data on the surgical technique used; unreported fixation sequence; lack of data on the clinical results evaluated by means of validated scores; and papers not published in English or published in non-indexed journals.
The literature review identified 10 potential articles that addressed the topic dealt with in the present study. According to the exclusion criteria applied, three articles were excluded because they had been published in languages other than English, while a further two articles were excluded because neither the fixation sequence nor the follow-up data were reported, thus leaving five articles to be included in the present review. A Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flowchart was reported (Figure 6). These five articles included three case reports that contained one case each and two small clinical series. The review was thus based on a total of 16 patients treated for multiple non-contiguous fractures of the femur. Details of the articles included in the review are shown in Table 2.
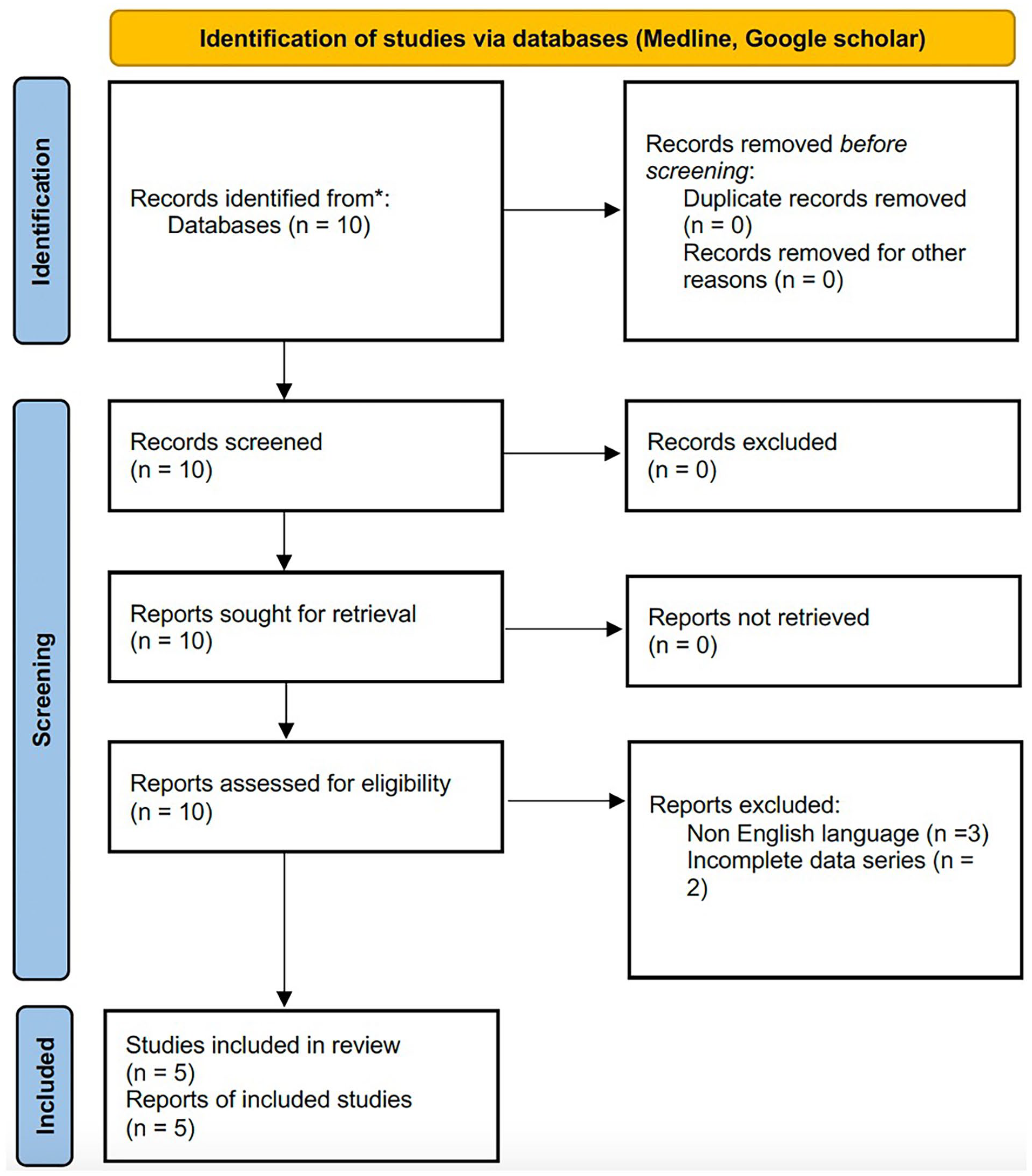
PRISMA flowchart for literature review.
Literature review.

Discussion
The present study addressed the treatment of multifocal fractures of the femur, which yielded good clinical and radiological results. These encouraging results confirm that satisfactory outcomes can be achieved when an appropriate treatment protocol with the correct timing and fixation sequence is applied.
Multiple femur fractures occur with a fairly predictable fracture pattern combination: a proximal femur fracture is always associated with a diaphyseal and a distal metaphyseal femur fracture, with or without intra-articular extension, or with a unicondylar fracture (medial or lateral). The fracture pattern is often complicated by Hoffa fractures or multifragmentary patellar fractures. Several soft tissue (ligament, meniscus, and tendons) lesions have been described in association with such fractures.1–4
The complexity of each fracture varies widely in different studies,1–5 ranging from undisplaced fractures to severely comminuted and displaced fractures. According to the literature, the fracture pattern incidence is as follows: medial proximal femur fractures are the prevalent fracture pattern in the proximal femur (11 patients, 68.7%), with the AO 31B2 pattern being the most frequent (10 patients, 90.9%), followed by transcervical fractures AO 31B3 (1 patient, 9.1%); proximal lateral femur fractures (AO 31A) account for 31.2% of the total number of fractures (5 patients), with 31A1 accounting for 80% of these cases and subtrochanteric fractures (AO 31A3) accounting for 20% (1 patient). This fracture pattern distribution may be explained by the trauma mechanism, with vertically-oriented fractures of the femoral neck resulting from direct axial load along the femoral diaphysis with a flexed hip and knee; by contrast, more lateral proximal femur fractures may be due to a different trauma mechanism (lateral impact) or a different hip position (slight abduction) at the moment of trauma.
Femur diaphyseal fractures mainly occur in the pattern of transverse fractures (AO 32A, seven patients), with AO 32A3 accounting for 85.7% (six patients) and AO 32A2 accounting for 16.6%. The second most common fracture pattern is the wedge fracture AO 32 B (six patients), with the intact wedge fracture (AO 32B2) accounting for 66.6% (four patients) and the fragmentary wedge fracture (AO 32B3) accounting for 33.3% (two patients). Multifragmentary diaphyseal fractures are reported in 3 out of 16 patients, with AO32C1 accounting for 33.3% (1 patient) and AO32C3 accounting for 66.6% (2 patients). The fracture pattern distribution depends on differences in the traumatic mechanism, which most often consists of a direct impact force rather than a rotatory one. Hoffa fractures of the femur (AO33B3) account for the majority of distal femur fractures (five patients), with lateral unicondylar fractures (AO 33B1) accounting for 14.2% (three patients) and medial unicondylar fractures (AO33B2) accounting for 9.5% (two patients). Extra-articular fractures account for 6.25% of the distal femur fractures (one patient): spiral fracture pattern (AO33A2, one patient, 33.3). Simple articular and metaphyseal fractures (AO33C) are reported in five patients (31.2%), with AO33C1 accounting for 80% (four patients) and AO33C3 accounting for 20% (one patient).
Patellar fractures are reported in two studies,1,2 in which they are described as open fractures, although no description of the fracture pattern is provided.
On the basis of our experience and of the current recommendations for the treatment of polytrauma patients, we propose the following algorithm for the treatment of such fractures (Figure 7).

Algorithm flowchart proposal.
Owing to the high-energy traumatic mechanism underlying these fracture patterns, patients with such lesions are expected to frequently have associated lesions of the chest or head as well as hemodynamic instability, which means admittance to intensive care units is mandatory. Since early total care in severely injured patients is unfeasible, as has been reported in previously published papers on this topic,10,11 a staged treatment based on the “window of opportunity” is the current routine approach.10,11 The initial emergency treatment is based on the application of external fixation (EF) frames of the femur or “bridging” the femoral-tibial EF frames with several configurations according to the fracture pattern; a computed tomography examination is subsequently performed in order to better define the fracture pattern and the articular involvement (if present), including the bone fragments, so as to allow accurate pre-operative planning.
When dealing with medial femur neck fractures in young patients with multiple fractures, every effort should be made to save the native femoral head in order to avoid complications and sequelae of a total hip replacement performed at a young age. Hence, it is of paramount importance to treat such fractures at the earliest opportunity, if possible in the emergency treatment phase, in order to avoid femoral head osteonecrosis due to vascular damage.10,12–14 The treatment consists in the reduction (if displaced) and fixation with percutaneous cannulated screws on a traction table. When treating a young patient with multiple fractures of the ipsilateral femur including a medial neck fracture that is suitable for internal fixation (Garden type 1–3), the fixation sequence needs to proceed from the proximal to the distal portion in a staged sequence, according to current practice.
In the other cases, the fixation sequence is mainly influenced by the variable combination of the fracture patterns present, both proximally and distally in the femur.
Lateral femur neck fractures associated with diaphyseal femur fractures and simple fracture patterns of the distal femur (A or B fractures according to AO classification) can be treated with a combination of a long proximal cephalo-medullary nail and distal plate and screws or with cannulated screws alone, proceeding from the proximal to the distal portion. We believe that the treatment of associated type A fractures of the distal femur can be performed with the use of a proximal long nail alone in only one circumstance: that is, when the distal fragment is large enough to accept at least three distal blocking screws locked in the nail and in a safe corridor in order to obtain sufficient bone purchase and withstand the axial and torsional forces acting on the distal femur. If the distal fragment is too short (<5 cm), a short LISS plate with the use of proximal monocortical angular stability screws surrounding the nail or an augment device associated with multiple screws in the same configurations is recommended. It is the authors’ opinion that the use of cerclage wire fixation around diaphyseal bone segments causes periosteal damage and potentially affects fracture healing; hence, it is not used by the authors in current practice. In cases in which type B mono-condylar fractures are associated, 6.5- or 7.5-mm cannulated screws with a neutralization 3.5 LCP plate can be used. The use of screws alone reduces the likelihood of early mobilization due to the limited possibility of withstanding the vertical displacing forces.
When the fracture consists of a simple lateral femur fracture, a diaphyseal fracture and a complex distal femur fracture (AO type C), the ideal sequence should start distally and proceed proximally.
The 3.5-mm multihole dedicated plates and free cannulated screws can be used in the distal femur. When a multifragmentary fracture of the metaphyseal area is present, a medial pre-contoured additional plate with autologous bone graft should be used because the lateral plate alone cannot withstand the displacing forces acting on the medial cortex. The proximal lateral fracture can be treated with a dynamic hip screw device when a stable fracture pattern is present. In cases in which complex proximal lateral femur fractures or sub-trochanteric fractures are present, an intramedullary device is recommended; in such cases, the nail length should exceed that of the diaphyseal fracture and of the distal plate or plates used for the internal fixation device, which can be achieved by using fixation augments anchored to the plate.
Medial femur fractures treated with cannulated screws allow for the placement of retrograde nails in case of diaphyseal fractures associated with simple extra-articular fractures of the distal femur (type A) or the use of a plate and screws to treat the diaphyseal and distal complex femur fracture (AO type B or C fractures). To the best of our knowledge, no studies in the current literature have described the use of prosthetic hip replacement for the treatment of displaced intracapsular neck fractures of the femur in patients with this injury pattern. This may be due to the fact that the traumatic energy is progressively dissipated along the femur, generally causing a non-displaced or mildly displaced intracapsular fracture of the proximal femur that is amenable to internal fixation. Only one study 4 described the use of the open reduction of a completely displaced medial neck fracture through an anterolateral Smith-Petersen surgical approach; no complications were reported by the authors of that study.
Patellar fractures should be treated with tension band wiring with or without cannulated screws or dedicated plates and screws, depending on the fracture pattern. Hoffa fractures are mainly treated with interfragmentary compression screws. The presence of Hoffa fractures requires the need for an arthrotomy that could be extended to explore the patella in case of concomitant patellar fractures.
Associated ligamentous lesions of the knee, such as anterior cruciate ligament and lateral or medial collateral ligament lesions, are difficult to treat in the acute-subacute setting since the surgical devices (plates, screws) in the distal region of the femur significantly interfere with the positioning of bone tunnels and may prevent the treating surgeon from performing the standard surgical procedures. Hence, it is logical to expect that such lesions are generally treated in the chronic setting, when fracture healing allows the removal of the surgical devices. It may be possible to treat both menisci lesions and osteochondral fractures in the acute setting, although no description of such treatment is reported in the literature.
According to Dousa et al., 1 no more than two surgical devices should be used for each bone segment, although the authors do not provide a biomechanical reason for their claim. We instead believe that the number of devices used should be based on the need to provide the most effective fracture treatment, that is, to create a sound biomechanical environment that allows the fracture to heal. It is thus our opinion that no limitations should be imposed in this respect.
The proximal to distal fracture fixation sequence was clearly described by Barei et al. 5 and Griffin et al. 3 in all their cases, as the review of the literature showed; interestingly, Barei et al. 5 reported an occult fracture of the femur neck discovered in two cases during the surgical intervention. Dousa et al. 1 reported a proximal to distal fixation sequence in three out of five cases, while a distal to proximal fixation sequence was adopted in the remaining two cases: their choice of sequence was based on the presence of either a B or C type fracture of the distal femur, leading to a proximal to distal or to a distal to proximal sequence, respectively. No data about the fixation sequence were reported in the other studies.
Surprisingly, in no studies was the use of an EF device as a damage control procedure reported. Bartonicek et al., 2 Griffin et al. 3 , and Kim et al. 4 performed the definitive surgical procedures on the day of trauma in spite of the presence of concomitant life-threatening injuries in their patients (such as severe head injury, rhabdomyolysis with acute renal failure, and chest injury with pulmonary contusion); Barei et al. 5 performed the definitive surgical procedure within 24 h of the original trauma in five out of seven patients, while no data were reported on when the other two patients underwent the surgical procedure. Barei et al. reported that two of the seven patients in their series had a severe abdominal injury, two had a severe chest trauma, and three had a closed head injury. No data on the surgical timing were provided by Dousa et al. 1 According to current clinical practice, most of these procedures would have been delayed because of the concomitant severe life-threatening injuries.
The clinical results reported in the studies included in the review are satisfactory, although none of the studies used validated scores to assess the clinical results.
The complication rate reported in the literature is 38%, with a reintervention rate of 19%; details are shown in Table 2. As is to be expected given the marked complexity of such lesions, axial deviations in the coronal plane with fracture malunion of the proximal or distal femur segment, limb length discrepancy, and non-union of the distal meta-diaphyseal portion of the femur are the most common complications. We did not observe any complications during follow-up in the patient in our study; the only complaint made by the patient was due to the prominence of the patellar tension band wiring fixation. This study has several limitations: since the nature of the study (case report), the treatment algorithm may need to be validated by a larger cohort of patients to highlight potential criticisms. Besides, this study represents the experience of a single tertiary center for the treatment of polytrauma patients.
However, this study has several strengths: the uniqueness of the clinical case presented here is the association of four different fracture patterns in the same femur, complicated by a concomitant patellar fracture, and the absence of associated ligamentous or meniscal tears. To the best of our knowledge, this is the first time such a complex pattern has been described in the literature. Besides, it is the first time that a proposal for a treatment algorithm of this injury pattern, comprehensive of timing and sequence of fixation for each possible combination of fracture, is reported in literature.
Conclusion
A patient-based treatment algorithm is indispensable to address all the possible fracture combinations observed in these challenging injury patterns and to provide the surgeon with general rules in the choice of the sequence, timing and fixation devices. We recommend that the surgical strategy be planned by first assessing the type of proximal femur fracture: whether a neck fracture is intracapsular or extracapsular may affect not only the timing but also the sequence and the type of fixation devices to be adopted since the treatment of medial fractures must be prioritized due to the risk of avascular necrosis caused by hip vascular damage. Besides, the correct surgical timing for definitive treatment should be respected in order to avoid the immunosuppressive phase in polytraumatized patients and to avoid the use of contraindicated devices in case of chest trauma (e.g., intramedullary devices) due to the risk of inflicting iatrogenic lesions on the patient. A temporary external fixator is recommended in such patients: in addition to offering the possibility to plan surgery by showing the fracture fragments spanned by ligamentotaxis, it also allows the surgeon to obtain all the fixation devices required and to carefully plan the overall surgical sequence. Highlighting the importance of this aspect, which has been overlooked in previous studies on this topic, may be considered the main strength of this study.
Footnotes
Acknowledgements
NA.
Author contributions
P.S. contributed to original writing, conceptualization, supervision; M.G. contributed to data curation; E.L. contributed to graphic art; S.A.M. contributed to data review; G.G. contributed to manuscript revision and supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from AO San Camillo-Forlanini, Rome, INSTITUTIONAL REVIEW BOARD (APPROVAL n SCF-20240721).
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.