
Abstract
Objective
This study aimed to evaluate variations in anterior condylar height (ACH) of the distal femur in varus knee osteoarthritis and evaluate the association between ACH and knee flexion.
Design
Computed tomography (CT) images of 171 knees (143 patients; age 73.7 ± 8.3 years; 132 females, 39 males) with symptomatic primary knee osteoarthritis and varus alignment undergoing primary total knee arthroplasty, unilateral knee arthroplasty, or high tibial osteotomy were evaluated. Several other anatomic parameters were measured on CT or radiography. The ACH and knee flexion correlation was analyzed, and factors contributing to knee flexion were determined using multivariable regression analysis.
Results
Medial ACH (mean, 8.1 mm; range, −2.8 to 19.9 mm) was smaller (P < 0.001) but more variable (F = 1.8, P < 0.001) than lateral ACH (mean, 10.7 mm; range, 3.6-18.3 mm). Medial ACH was moderately correlated with flexion (r = −0.44, 95% confidence interval [CI], −0.55 to −0.32), whereas lateral ACH was weakly correlated (r = −0.38; 95% CI, −0.50 to −0.25). On multivariable linear regression analysis of knee flexion, body mass index (B [partial regression coefficient] = −1.1), patellofemoral Kellgren-Lawrence grade (B = −4.3), medial ACH (B = −1.2), medial posterior condylar offset (B = 1.2), age (B = −0.4), and varus alignment (B = −0.6) remained significant independent variables (adjusted R2 = 0.35).
Conclusions
Wide variation and anteriorization of the anterior condyle of the distal femur was observed in advanced osteoarthritis, as an independent determinant of limited knee flexion.
Introduction
Osteoarthritis (OA) is a prevalent disease that limits mobility and impairs activities of daily living in elderly individuals. As OA progresses, patients suffer from limited range of motion (ROM), which disrupts activities such as sitting and stair walking and causes pain at rest and/or during motion. 1 Surgery in cases of severe OA can reveal a wide variety of shapes of the anterior condyle of the distal femur. Large osteophyte formation, which can affect patellar tracking, occurs in some patients. However, almost no damage to the patellofemoral (PF) joint is seen in others despite severe degenerative changes to the tibiofemoral (TF) joint. Although PF joint degeneration is often described in terms of pain, the correlation between PF joint and ROM is less fully elucidated.2,3 OA in the PF joint is not uncommon, occurring in 19% to 64% of symptomatic knees,2-5 whereas a cadaveric study revealed that up to 79% of individuals aged >65 years had PF OA. 6 PF OA is an important cause of pain in knee OA,7,8 and comorbid PF and TF OA is associated with worse clinical symptoms. 3 Osteophytes in the PF joint can cause overstuffing that increases joint pressure and shear force, which could theoretically decrease knee flexion. 9
Regarding knee ROM, age, body mass index (BMI), OA progression in the TF or PF joint is correlated with knee flexion.10-13 After total knee arthroplasty (TKA), several anatomic factors such as posterior condylar offset (PCO), tibial slope, and patellar position are determinants of knee flexion,14-16 although controversy persists regarding which anatomic feature contributes the most to ROM limitations in knee OA.
In terms of the anatomy of the anterior condyle of the distal femur, Fehring et al. 17 introduced the concept of anterior condylar height (ACH), which they defined as the height of the prominence of the anterior trochlea at 10 mm above the joint line, and reported wide variation in the ACH of the medial and lateral condyles even in a healthy population. Yang et al. 18 analyzed the most prominent point of the ACH in OA knees excluding cases of severe malalignment. Here, we measured ACH using the most prominent point of varus OA knees, including those of patients with symptomatic OA who underwent surgeries, and investigated the effect of ACH on knee flexion as well as other anatomic and characteristic parameters. This study aimed to evaluate ACH size of the distal femur in varus OA knees and investigate the influence of ACH on limited knee flexion under the hypothesis that ACH is largely affected by knee OA and that a high ACH is associated with limited knee flexion.
Methods
This study was approved by the Kyoto University Graduate School and Faculty of Medicine, Kyoto University Hospital ethics committee (approval number E2013) for the prospective data collection. Written informed consent was obtained from all participants. Among 285 consecutive surgeries performed between 2012 and 2016 against primary varus knee OA, 171 varus knees from 143 patients for whom preoperative lower extremity computed tomography (CT) scans were available were included. Among 171 knees, TKA was performed on 149 knees, high tibial osteotomy was performed on 18 knees, and unilateral knee arthroplasty was performed on 4 knees. Demographic data for all 171 OA knees are shown in Table 1 . Knee ROM was measured preoperatively using a handheld goniometer by a physiotherapist who was not involved in the study. Anteroposterior, lateral, and skyline Merchant X-rays of the knee and full-length anteroposterior X-rays of the lower legs were taken. Kellgren-Lawrence (KL) grades of the TF and PF joints were scored separately from those on preoperative plain radiographs. 19 The hip-knee-ankle (HKA) angle, the angle between the mechanical axis of the femur and the tibia, was also measured on the full-length lower extremity radiographs. Neutral alignment was defined as an HKA = 0°, whereas varus and valgus alignments are expressed as positive and negative values, respectively.
Demographics of the Patients with OA.
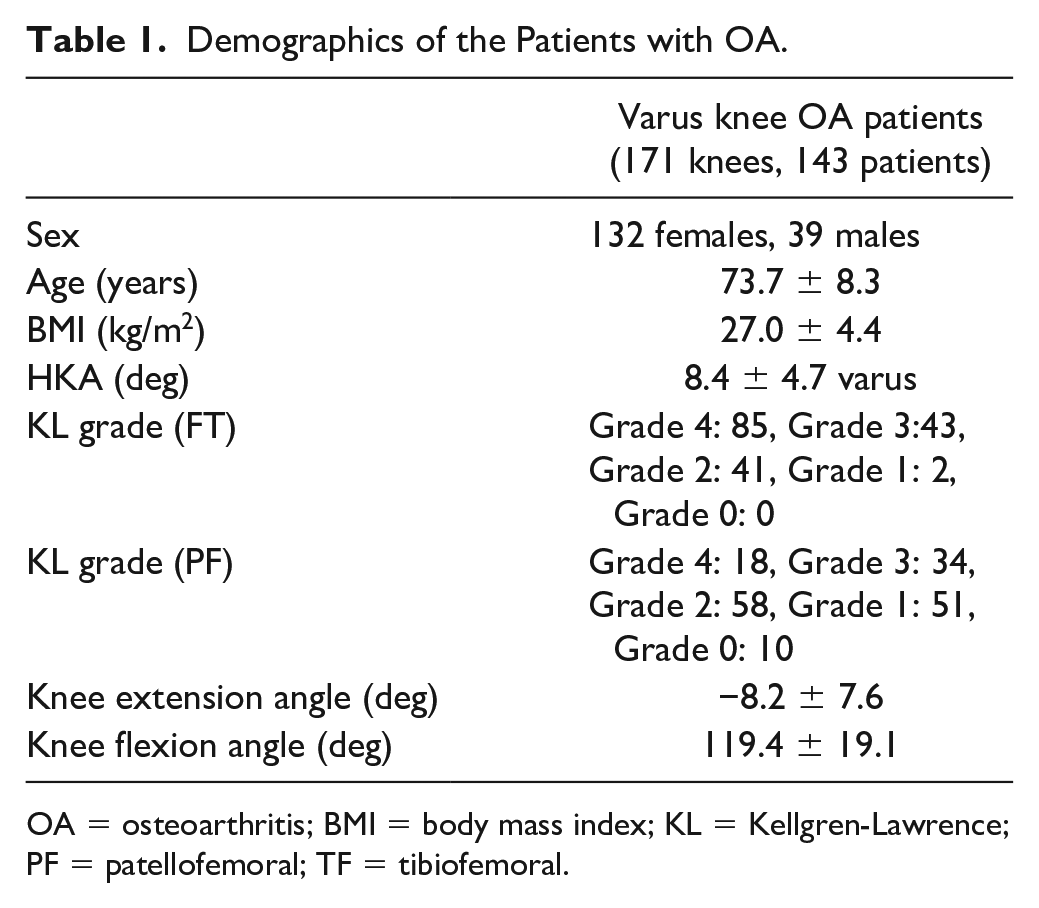
OA = osteoarthritis; BMI = body mass index; KL = Kellgren-Lawrence; PF = patellofemoral; TF = tibiofemoral.
Computed Tomography
CT scans were taken of each affected lower extremity. Three-dimensional reconstructions were performed and each ACH was measured as follows. The anterior cortex of the femur was identified on the midline sagittal image of the distal femur, and the plane that included the anterior cortex and was parallel to the surgical epicondylar axis was identified as plane A ( Fig. 1A ). In the axial image, the length in millimeters of a perpendicular line from the most prominent point of the medial anterior condyle, the deepest point of the trochlea sulcus, and the most prominent point of the lateral anterior condyle to plane A was measured ( Fig. 1B ). Among consecutive axial slices in the distal femur, the maximum length in each measurement was defined as medial ACH, sulcus height, and lateral ACH, respectively. For the first 24 knees, the measurements of medial and lateral ACH were performed independently by 2 orthopedic surgeons, and the interobserver intraclass correlation coefficient (ICC) was 0.70 (0.24-0.89) for medial ACH, 0.63 (0.32-0.82) for sulcus height, and 0.74 (0.32-0.91) for lateral ACH. The intraobserver ICC was determined using repeated measurements of the same patients after a 1-week interval and were determined to be 0.89 (0.77-0.95) for medial ACH, 0.79 (0.51-0.91) for sulcus height, and 0.87 (0.72-0.94) for lateral ACH. Several other parameters possibly related to ROM were also measured on the same CT scans. The medial and lateral tibial posterior slope (angle between the medial or lateral natural posterior slope and the mechanical axis of the tibia 20 ), PCO (the line from the most prominent point of the medial or lateral femoral condyle to the plane that included the posterior cortex of the distal femur and was parallel to the surgical epicondylar axis 21 ), and Insall-Salvati ratio (calculated by dividing the patellar tendon length by the patellar length on the mid-sagittal view 22 ) were measured as previously described. The anterior bowing angle of the femoral shaft (sagittal angle between the proximal quarter axis and the distal quarter axis 23 in the midcoronal plane of the femoral shaft) and the lateral bowing angle of the femoral shaft (coronal angle between the proximal quarter axis and the distal quarter axis in the midsagittal plane of the femoral shaft23,24) were also measured.
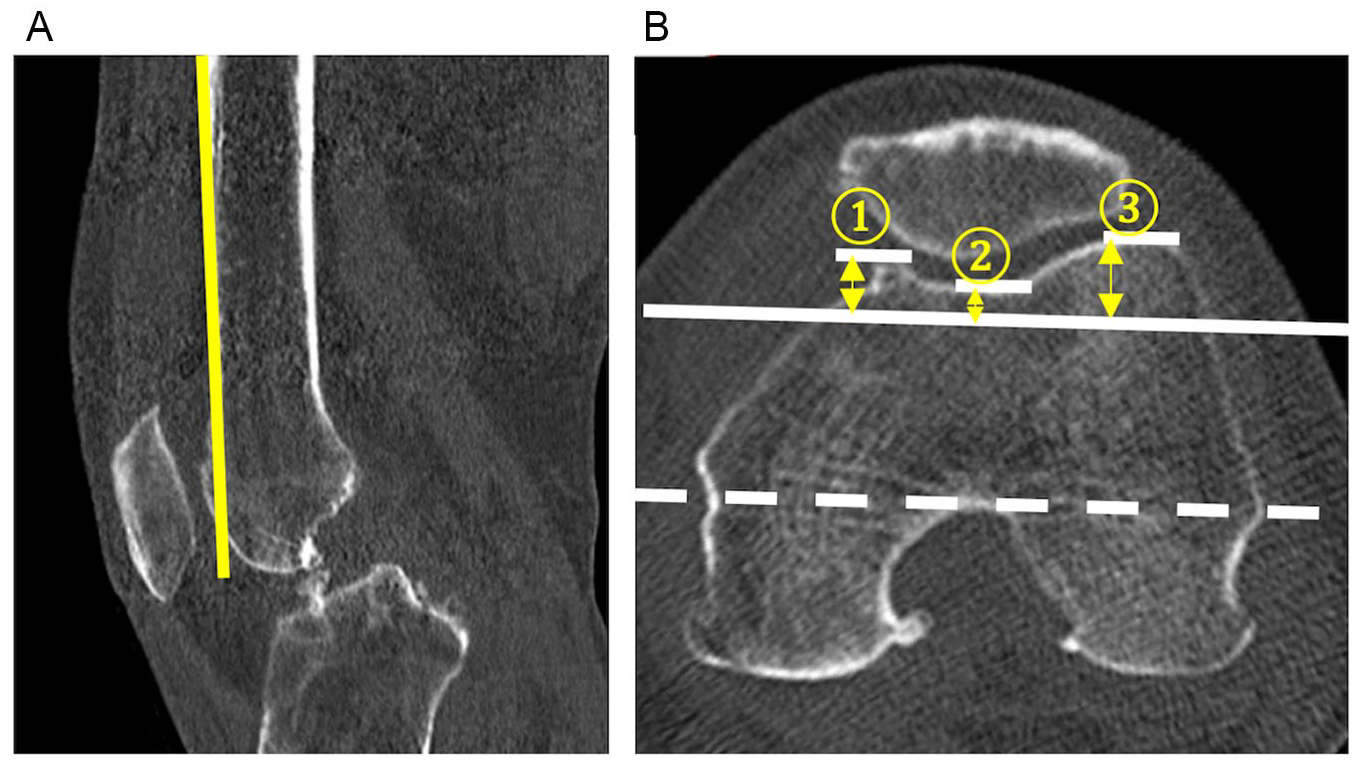
Computed tomography image of plane A containing the anterior cortex of the femur (yellow line in
Statistical Analysis
The homogeneity of variance between ACH values was evaluated using F test. To compare ACH and sulcus height values, the Kruskal-Wallis test was used with Dunn’s post hoc comparison. The upgoing trend of ACH values and sulcus height according to KL grade in TF or PF joints were analyzed using the Jonckheere-Terpstra test. A downward trend in the difference of medial ACH and lateral ACH was also analyzed by the Jonckheere-Terpstra test. The correlations between ACH and sulcus height with HKA were evaluated using Pearson’s correlation coefficient. To examine the correlation between knee flexion and each ACH or sulcus height, Pearson’s correlation coefficient was used. In the Pearson correlations, values of r ≤ 0.20, 0.20 < r ≤ 0.40, 0.40 < r ≤0.70, 0.70 < r ≤ 0.90, and 0.90 < r were considered negligible, weak, moderate, strong, and very strong, respectively. 25 Multivariable linear regression analyses were performed with knee flexion as the dependent variable and patient characteristics and anatomical parameters as independent variables. A backward-stepwise approach to minimize the Akaike information criterion for optimal model fit was used. Statistical analyses were performed using R 3.3.1 (R foundation, Vienna, Austria) with the EZR plug-in (Saitama Medical Center, Jichi Medical University, Saitama, Japan) and R 3.4.3. Statistical significance was set at values of P < 0.05.
Results
In the study participants, the medial ACH (8.1 mm ± 3.6 SD; range, –2.8 to 19.9 mm) was more variable (F = 1.8, p < 0.001), but it had a smaller mean than the lateral ACH (10.7 mm ± 2.7 SD; range, 4.8-18.3 mm), while the sulcus height (4.3 mm ± 2.3 SD; range, 0.0-10.8 mm) was the smallest ( Fig. 2 ). The lateral ACH was greater than the medial ACH in 144 knees, while the medial ACH was greater in 27 knees in OA knees.
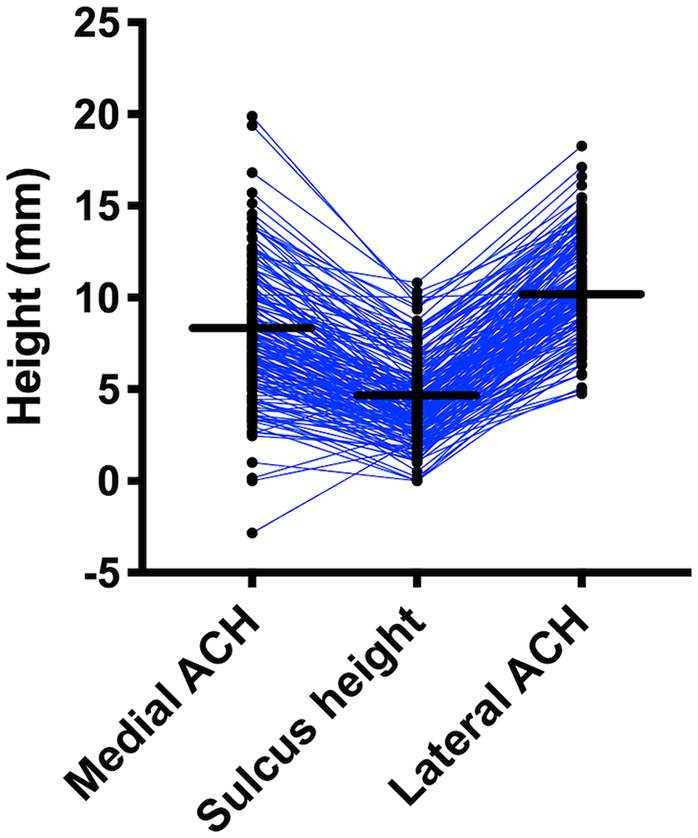
Shown is a dot-plot with mean (solid bar) of preoperative medial ACH, sulcus height, and lateral ACH. Medial ACH was smaller but more variable than lateral ACH. ACH, anterior condylar height
Medial ACH, sulcus height, and lateral ACH were correlated with HKA (medial ACH: r = 0.28; 95% confidence interval [CI], 0.14-0.42; sulcus height: r = 0.33; 95% CI, 0.19-0.46; lateral ACH: r = 0.26; 95% CI, 0.11-0.39). A clear trend of increased medial and lateral ACH and sulcus height at higher TF ( Table 2 ) and PF ( Table 3 ) KL grades was found. A trend was also found in the difference between medial and lateral ACH, which became smaller with progression of TF (P = 0.049) and PF OA (P = 0.004).
ACH and Sulcus Height According to TF KL grade.
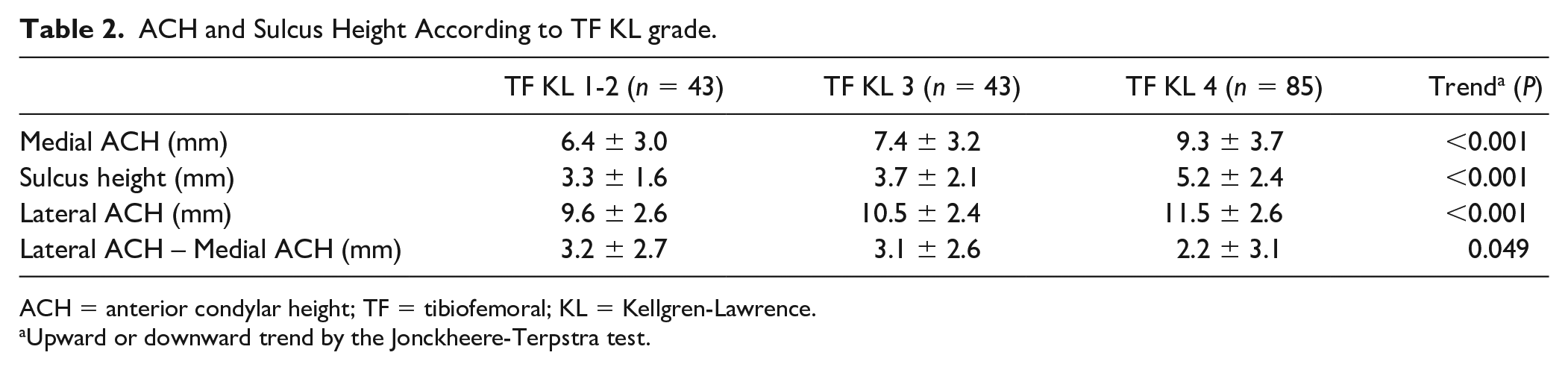
ACH = anterior condylar height; TF = tibiofemoral; KL = Kellgren-Lawrence.
Upward or downward trend by the Jonckheere-Terpstra test.
ACH and Sulcus Height According to PF KL Grade.
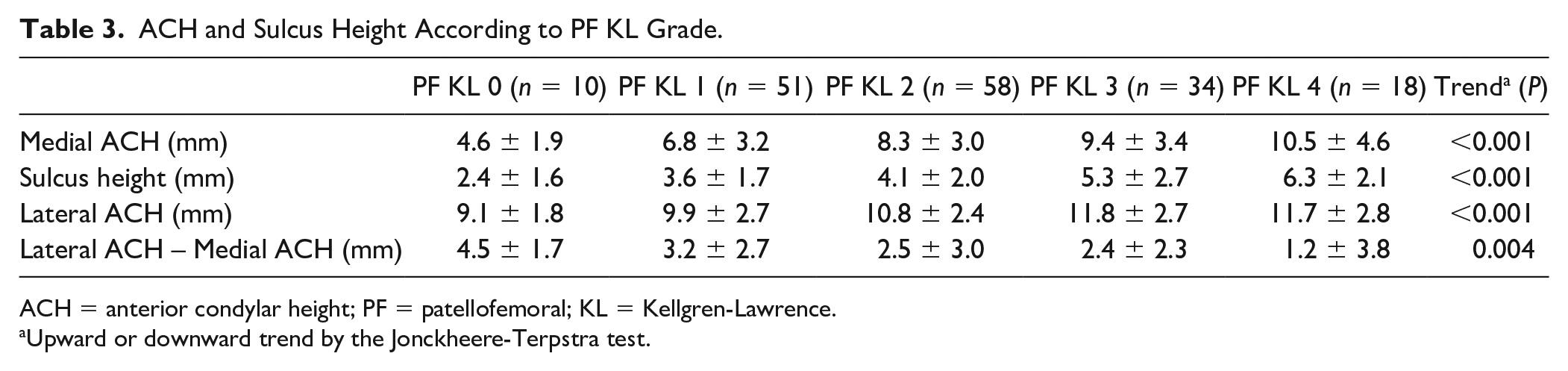
ACH = anterior condylar height; PF = patellofemoral; KL = Kellgren-Lawrence.
Upward or downward trend by the Jonckheere-Terpstra test.
The larger the ACH or sulcus height, the more the knee flexion was restricted. Medial ACH (r = −0.44; 95% CI, −0.55 to −0.32) and sulcus height (r = −0.43; 95% CI, −0.54 to −0.31) were moderately correlated with knee flexion ( Fig. 3 ). Although the correlation was weak, lateral ACH (r = −0.38; 95% CI, −0.50 to −0.25) was also significantly correlated with knee flexion ( Fig. 3 ). On the multivariable regression analysis, older age, higher BMI, varus alignment, progression of PF KL grade, higher medial ACH, and lower medial PCO were independently associated with knee flexion with an adjusted R2 = 0.35 ( Table 4 ).
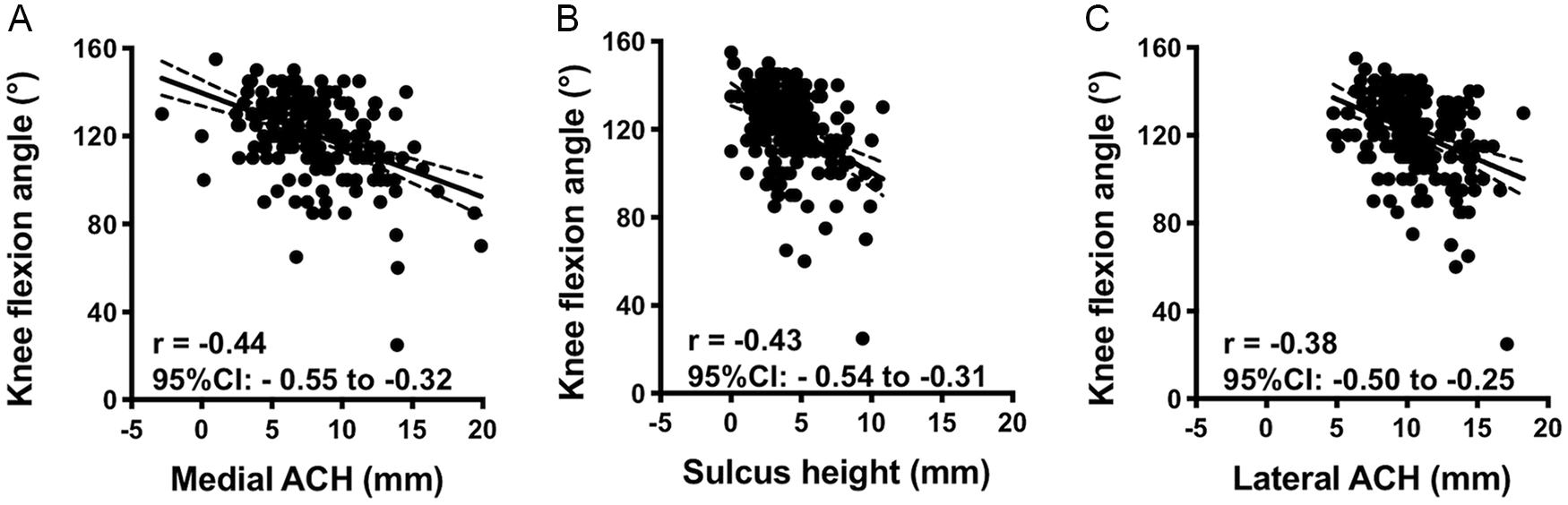
Scatterplot of medial ACH (
Multivariable Regression Analysis to Minimize AIC for Knee Flexion.
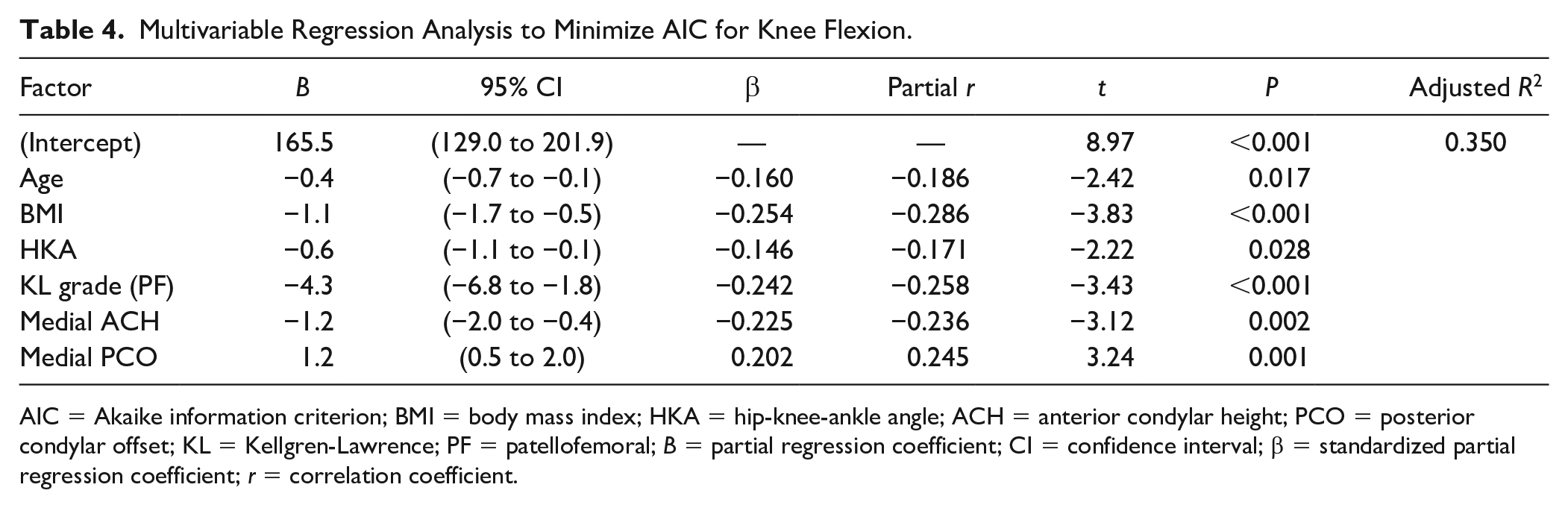
AIC = Akaike information criterion; BMI = body mass index; HKA = hip-knee-ankle angle; ACH = anterior condylar height; PCO = posterior condylar offset; KL = Kellgren-Lawrence; PF = patellofemoral; B = partial regression coefficient; CI = confidence interval; β = standardized partial regression coefficient; r = correlation coefficient.
Discussion
ACH, especially medial ACH, showed wide variety in OA patients and independently contributed to limited knee flexion. Medial ACH was higher than lateral ACH in 27 of 171 cases (16%) in varus OA knees. ACH and sulcus height were related to knee OA progression determined by KL grade, in which mean ACH and sulcus height were higher in advanced OA knees than in mild OA knees. A high ACH in knee OA, especially medial ACH, was associated with restricted knee flexion independent of OA grade.
In most OA cases included in this study, lateral ACH was greater than medial ACH. One previous study measured ACH 10 mm above the joint line, 17 whereas another defined ACH as the maximum protrusion of the medial or lateral femoral condyle. 18 We adopted the most prominent point as that influencing OA progression and speculated that, in OA patients, the ACH at the most prominent point may influence PF joint pressure more than ACH at 10 mm above the joint. Fehring et al. 17 reported that the mean lateral ACH was greater than the mean medial ACH, although in contrast to our results, the range of the lateral ACH was greater than that of the medial ACH. The critical difference between the studies was due to their study including healthy individuals, whereas ours included patients with advanced OA who required TKA. Yang et al. 18 investigated ACH in OA patients and reported mean lateral and medial ACH values of 8.2 ± 1.8 mm and 3.1 ± 1.5 mm for men and 7.4 ± 1.7 mm and 3.6 ± 1.5 mm for women, respectively. Mean ACH values were higher in our study (lateral ACH, 10.7 ± 2.7 mm; medial ACH, 8.1 ± 3.6 mm), presumably due to the more advanced OA stage in our series. Their series excluded cases with deformities >15° varus or valgus, whereas our OA cohort included cases with severe varus deformity. Because cases of advanced OA had a higher mean ACH and sulcus height values than those of mild OA condition, the entire patellar groove was deemed to have shifted anteriorly as the OA progressed. Therefore, during attempts to restore the healthy anterior condyle anatomy in TKA, restoration of the preoperative anatomy of the anterior condyle may lead to anterior replacement against the healthy anterior condyle.
A trend was found of a decreasing difference between medial and lateral ACH with increasing value of TF and FT KL grade. The mean lateral ACH was 4.5 mm higher in PF KL grade 0 but only 1.2 mm higher in PF KL grade 4 than medial ACH. Although the correlation coefficient to HKA was similar between medial and lateral ACH, previous reports suggest that the progression of OA might affect medial anterior condyle more than lateral anterior condyle. In the PF joint, varus knee alignment increases the Q(quadriceps)-angle, increasing medial PF force and theoretically leading to medial PF OA occurrence or progression. Varus alignment is reportedly associated with a 2-fold increase in the likelihood of medial PF OA progression. 26 In a study that investigated osteophyte size and direction in the TF and PF joints in detail, the incidence of osteophyte formation at the anterior condyle, which potentially increases ACH, was 35.9% on the medial side and only 5% on the lateral side in OA patients. 27 As suggested by previous reports, this study also included several cases of a high medial ACH due to significant osteophyte formation.
ACH independently affects knee flexion. Knees with an elevated condyle tended to have restricted ROM. A high ACH increases PF joint pressure, and overstuffing of the PF joint can result in restricted knee flexion.28-32 In the multivariable regression analysis, higher BMI, worse PF KL grade, higher medial ACH, lower medial PCO, varus alignment, and older age were independently associated with limited knee flexion. The relationship between restricted flexion and age, BMI, or PF OA has been reported.33,34 Although the effect of anatomical parameters such as PCO or tibial slope on ROM after TKA have been widely studied,14-16,21,35-37 the contribution of PCO to OA knees has not been fully described. In terms of the anterior anatomy of the distal femur, to our knowledge, this is the first study to demonstrate the relationship between anterior condyle shape and restricted knee flexion. Our multivariable regression model explained about one-third of the knee flexion in OA knees, with partial correlation coefficient of medial ACH as −0.236.
In this study, 2 factors of the PF joint were related to knee flexion. Holla et al. 13 reported that BMI, osteophytes of the medial TF joint, and some clinical factors such as pain and crepitus were determinants of knee flexion. In another report, knee flexion was correlated with KL grade of the medial TF joint but not of the PF joint. 11 There is a critical difference between their study and ours in patient characteristics in that their study enrolled patients with early OA and >130° of flexion, whereas ours enrolled patients with moderate-to-advanced OA including severe varus deformities who were undergoing TKA with a mean flexion of 120°. In patients with early OA, PF joint degeneration was not frequently severe, whereas TF joint degeneration was predominant. However, in patients with severe OA, PF joint degeneration further progressed, which might have overcome the effect of the TF joint on knee flexion. This study’s findings emphasize the importance of the impact of PF joint degeneration and anatomical changes on knee flexion in advanced OA knees.
This study demonstrated a new significance of the anterior condyle anatomy in advanced OA knees. However, it has some limitations. First, because this is a cohort study of OA patients undergoing surgery, healthy controls and early OA patients were not included. For ethical reasons, it was difficult to subject healthy or asymptomatic OA populations to CT. Compared with past studies, the ACH of moderate-to-advanced OA knees in this study was higher, but a direct comparison cannot be performed. Second, because this investigation included patients with moderate-to-advanced OA, osteophytes played an important role in ACH. It is unknown whether ACH affects knee flexion in early OA knees. Third, changes in patellar size were not included in this study. Degeneration of the patellar cartilage and the trochlea was seen along with osteophyte formation in the patella and anterior condyle. In theory, an increased patellar thickness could cause overstuffing and affect ROM. 31 Fourth, pain and crepitus, which are possibly related to flexion, were not included in this study. However, it was assumed that all patients had considerable pain by which patients agreed to undergo surgery. Fifth, because this was a cross-sectional study, although we speculated that OA progression caused the ACH enlargement, the causative effect of OA on an increased ACH could not be concluded. Sixth, valgus knee OA was not discussed in this study. Despite these limitations, the strength of this study was its use of CT to evaluate anatomical parameters as it yields accurate measurements as well as the number of included anatomical parameters that could have affected ROM.
In summary, advanced OA knees had high ACH values with large variations, especially in the medial anterior condyle. A high ACH was correlated with limited knee flexion. High BMI, advanced PF OA, high medial ACH value, small PCO, varus alignment, and older age independently contributed to limited flexion in varus OA knees. Orthopedic surgeons should be aware that the patellar groove may shift anteriorly when they aim to restore native anterior anatomy during TKA.
Footnotes
Authors’ Note
This work has performed at Kyoto University Hospital.
Acknowledgments and Funding
The authors thank Drs. Yoshihisa Tanaka, Mutsumi Watanabe, Motoo Saito, and Shigeo Yoshida for their thoughtful discussion and ordinary support. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Kyoto University Graduate School and Faculty of Medicine, Kyoto University Hospital ethics committee (approval number E2013) for the prospective data collection.
Informed Consent
Written informed consent was obtained from all participants.
Trial Registration
Not applicable.