
Abstract
Pediatric humeral medial condyle fracture (HMCF) is a rare condition and is difficult to detect, especially in young children. The management of late presentation of HMCF is challenging and lacks consensus. Herein, we reported four cases of HMCF nonunion received open reduction and internal fixation (ORIF) or supracondyle osteotomy from our institution. In addition, 12 cases of ORIF and 4 cases of osteotomy reported in the previous studies were also reviewed. The HMCF nonunion can heal after ORIF, but the indication and the optimal techniques need to be clarified. Supracondylar osteotomy alone is an effective and safe treatment option to improve the functional and cosmetic outcomes of HMCF nonunion.
Introduction
Humeral medial condyle fractures (HMCFs) are very rare injuries, and they account for <1% of all pediatric elbow fractures; consequently, HMCF diagnosis is very challenging. 1 –3 Late trochlear ossification may increase the risk of misdiagnosis in young patients. 4 Pediatric HMCF is classified as a Salter–Harris type IV injury and intra-articular fracture. Nonunion, growth disturbance, joint stiffness, and gross deformity are common occurrences in neglected HMCF cases. 4 –7 Early recognition and appropriate therapy for HMCF can generally achieve satisfactory results 8 ; however, there is currently no consensus on the management of HMCF nonunion.
In neglected HMCF cases, open reduction internal fixation (ORIF) may lead to suboptimal and unpredictable results. 3,4,7,9 Ippolito et al. concluded that operating on nonunion HMCF tends to have bad outcome. 10 Humeral supracondylar osteotomy is an alternative treatment option; however, little is known about the indications and outcomes of corrective osteotomy for neglected HMCF. In this report, our aim was to present four HMCF nonunion cases treated at our institution and to review the surgical outcomes of the neglected HMCF in the literature.
Materials and methods
Case series
After approval was obtained from the institutional review board, we retrospectively reviewed the data of patients who were diagnosed with HMCF nonunion at our institute between January 1, 1990, and December 30, 2018. HMCFs were confirmed based on X-ray data at diagnosis. We defined HMCF nonunion as ≥3 months after injury without evidence of fracture union. The clinical, radiological, and outcome data were extracted from the electronic health record system. Of the four cases obtained, one patient had received ORIF, and three patients had received humeral supracondylar dome osteotomy (SDO) as previously described. 11 –13 Briefly, SDO was performed to correct the cubitus varus through the posterior approach of the elbow. The arc of SDO was done based on preoperative planning. A lateral 3.5-mm Locking Compression plate (LCP) distal humerus plate or multiple Kirschner wires were applied for fixation according to the size of the osteotomy site.
Patients were followed up for a minimum of 12 months after surgery, with the fracture site and osteotomy site healing and radiological alignment being assessed by an independent orthopedic surgeon. The surgical outcomes were assessed using the Mayo Elbow Performance Score (MEPS) at the last outpatient clinic follow-up, and the modified criteria introduced by Bensahel et al. were used for evaluating HMCF cases. 2
Results
Case series
Case 1
A 21-year-old female patient visited our clinic with complaints of chronic right elbow pain and cubitus varus deformity (Figure 1). She had sustained right elbow injury at the age of 9 years. Radiographic examinations showed HMCF nonunion in which a bony fragment was displaced anterior medially. The radiographic carrying angle (RCA) of the right upper extremity was 12° varus. Surgical treatment was indicated for pain relief. After ulnar nerve anterior transposition through the posterior approach of the elbow, the fragment was refreshed and fixed using two 4.0-mm cannulated screws in the position in which the contact area was the largest, without affecting the range of motion (ROM) of the elbow. A long arm cast was applied with the elbow held at 90° of flexion and the forearm was kept in the neutral position for 4 weeks. At the 2-month follow-up, radiographic examination demonstrated that fracture union was achieved, and the right RCA was about 8° varus; numbness on the volar side of the right fourth and fifth fingers was reported, but there was no motor weakness or claw hand. Additionally, right elbow ROM slightly decreased compared with the preoperative ROM (preoperative: 10–90°; postoperative at 2 months: 15–90°). At 5 months after surgery, the screws were removed and the intra-articular adhesive scar tissue was debrided under general anesthesia. At the last follow-up 1 month after the removal of screws, both the reported numbness and the elbow ROM had significantly improved (10–115°).

Preoperative and postoperative radiographs of case 1. (a) Preoperative radiograph. Varus alignment of the whole elbow (preoperative: 8° varus). (b and c) Postoperative radiograph. The fracture had united at 2 months after surgery and the radiographic carrying angle was slightly improved (postoperative: 4° varus). (d and e) Post screws removal at 12 months after surgery. Persistent cubital varus was noted.
Case 2
An 18-year-old male patient was referred to our clinic for right cubitus varus deformity (Figure 2). He had sustained right elbow injury at the age of 5 years and received no treatment. No significant pain or joint instability was reported. Radiographic examinations revealed right HMCF nonunion, and the fracture fragment was displaced anterior medially. The preoperative right elbow RCA was 13° varus and the ROM was 15–130°. We performed SDO to address varus deformity and left the nonunion fragment alone. The postoperative RCA was 9° valgus. Osseous union of the osteotomy site was achieved at 2 months after surgery. The postoperative ROM was 0–130°, and the MEPS was 100 at 5 months after surgery.

Preoperative and postoperative radiographs of case 2. (a to d) Preoperative radiographs and the 3D CT reconstruction. Varus alignment of the whole elbow. (e and f) Postoperative radiograph. The postoperative alignment was restored to the neutral position.
Case 3
A 17-year-old female patient was referred to our clinic for left elbow varus deformity and persistent tenderness. She had sustained left elbow contusion at the age of 6 years and received ORIF at the age of 11 years at another hospital. Our initial radiographs revealed persistent HMCF nonunion and RCA of 13° varus. We performed SDO and left the nonunion fragment alone. The postoperative RCA was 15° valgus and union of the osteotomy site was achieved at 3 months after surgery. The patient returned to normal activities with no reported difficulties. The postoperative ROM was 5–120° at 6 months after surgery, and the final MEPS was 100 at 6 months after surgery.
Case 4
A 4-year-old female patient was referred to our clinic for right elbow varus deformity (RCA of 38.7° varus) and limited ROM (0–105°). She had sustained right elbow injury at the age of 3 years, and the initial radiographic examinations revealed humeral supracondylar and intercondylar fracture. She had immediately received closed reduction and long arm casting at another hospital, with union of the supracondylar fracture being achieved. However, persistent HMCF nonunion was observed while visiting our clinic the year following. We performed SDO and left the nonunion fragment alone when the patient had attained 5 years of age. The postoperative RCA returned to the neutral position and union of the osteotomy site was achieved at 3 months after surgery. However, she sustained right elbow dislocation after falling with an outstretched hand at the age of 9 years. The dislocation was very unstable and open reduction with soft tissue reconstruction was performed. The patient returned to normal activities with no further complaints or newly occurred dislocation, and the postoperative elbow ROM was 0–135° at 6 months after the second surgery. The final MEPS was 95 at 6 months after the second surgery.
Literature review
We searched for relevant articles from the PubMed database using the term “HMCF” and “distal humeral fracture.” Articles that were published in English and involved human subjects were included. We selected all original case series studies that reported surgical outcomes for HMCF nonunion. The demographic data, surgical treatment, and postoperative results were recorded and summarized.
Case series from a total of 14 articles that met the inclusion criteria were summarized and categorized into the ORIF or osteotomy groups (Tables 1 and 2). The ORIF group included 14 patients from both our case series and the literature. The mean age at injury was 7.17 years (range 3–13 years), and the mean age at surgery (ORIF) was 9.5 years (range 4–21 years). The fracture union was achieved in nine cases, and two cases had persistent nonunion after ORIF. In the ORIF group, five patients had poor, six patients had fair, and two patients had good functional outcomes (Table 3).
Demographic, clinical, and surgical outcomes of patients who had received ORIF for late presentation of HMCF.

ORIF: open reduction internal fixation; HMCF: humeral medial condyle fracture; Ref.: reference; no.: number; M: male; F: female; NM: not mentioned; Preop: preoperative; ROM: range of motion; Fr.: fracture; Y: yes; N: no; Postop: postoperative.
a Surgical outcomes were evaluated based on the criteria of this table.
b Case 14 in the ORIF group is same as case 6 in the osteotomy group.
Demographic, clinical, and surgical outcomes of patients who had received humeral supracondylar osteotomy for late presentation of HMCF.
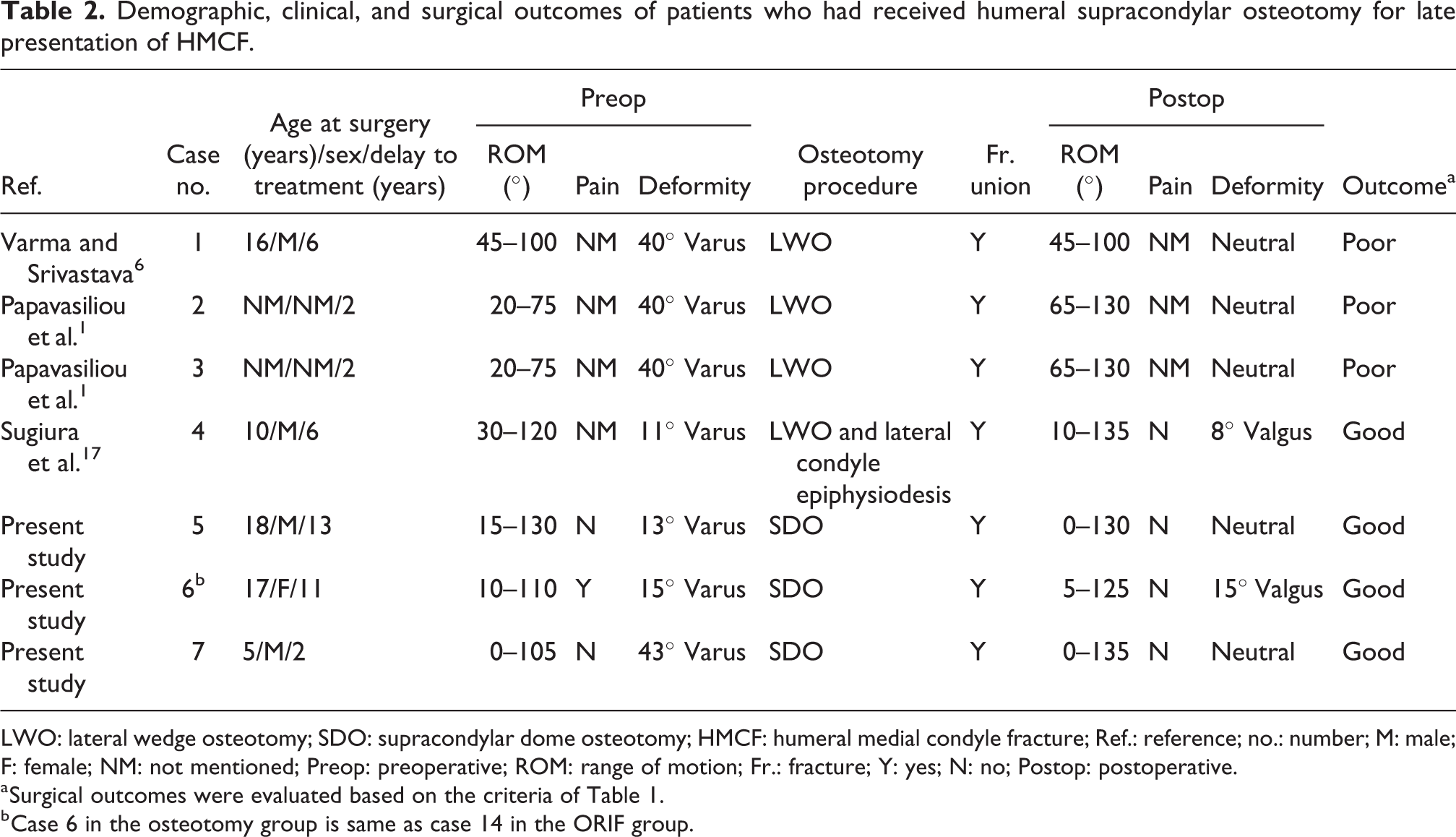
LWO: lateral wedge osteotomy; SDO: supracondylar dome osteotomy; HMCF: humeral medial condyle fracture; Ref.: reference; no.: number; M: male; F: female; NM: not mentioned; Preop: preoperative; ROM: range of motion; Fr.: fracture; Y: yes; N: no; Postop: postoperative.
a Surgical outcomes were evaluated based on the criteria of Table 1.
b Case 6 in the osteotomy group is same as case 14 in the ORIF group.
Classification of functional outcomes after surgery.a
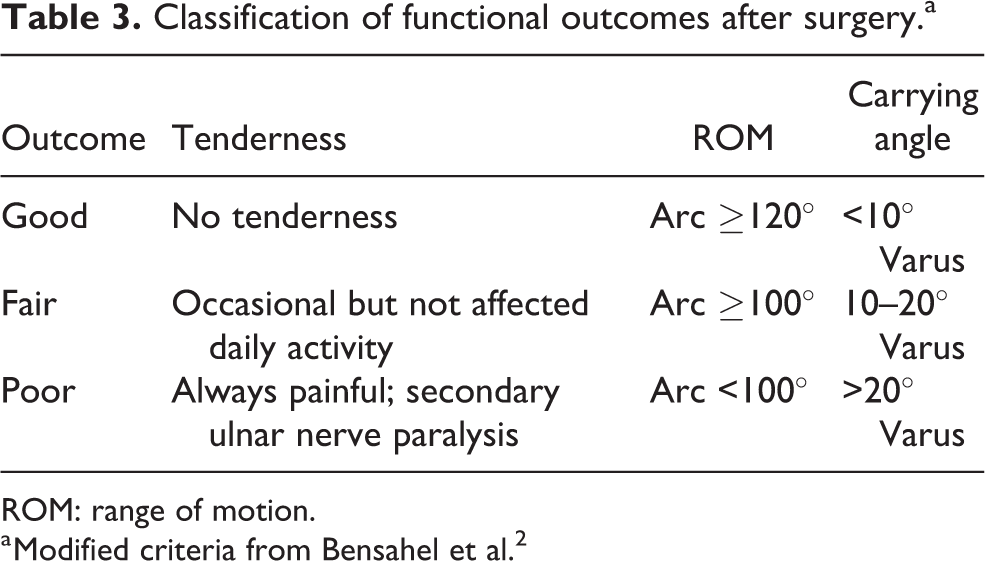
ROM: range of motion.
a Modified criteria from Bensahel et al. 2
The osteotomy group included seven patients. The mean duration between definite surgery and injury was 6 years (range 2–13 years). Supracondylar lateral closing wedge osteotomy was performed in most cases except the present study, in which SDO was performed. All patients achieved osteotomy site union, and the postoperative elbow ROM was either maintained or improved. Among these seven cases, four had good and three had fair functional outcomes (Table 3).
Risk factors related with bony union after ORIF
Logistic regression analysis was used to analyze the risk factors affecting bony union after ORIF. Sex (odd ratio (OR) <0.001; p = 0.947), age at ORIF (OR 1.124; p = 0.4476), and interval between injury to ORIF (OR 0.999; p = 0.9422) were not significant risk factors for nonunion after ORIF.
Discussion
A total of approximately 7.4–33.3% of patients with HMCF had persistent nonunion are reported as having been left untreated. 4,6,14 Management of HMCF nonunion is very challenging, and persistent pain, limited ROM, and gross deformity of the elbow and forearm are common in these patients. 1,3,5,14,18 Both ORIF and supracondylar osteotomy are the common surgical treatment options for HMCF nonunion. This study provides the largest series of HMCF nonunion cases and a review of the surgical outcomes of HMCF nonunion cases in previous studies.
Fowles and Kassab advocated that untreated fractures lasting for more than 4 weeks should not be operated on. 4 Based on our literature review, ORIF was not an absolute contraindication for the late presentation of HMCF. Our literature review indicated that the union rate after ORIF was 85.7 % in HMCF nonunion cases. Of the 14 patients who had received ORIF, two had persistent nonunion after surgery. We found sex, age at ORIF, and interval between injury to ORIF were not significant risk factors for nonunion after ORIF. However, it is difficult to draw conclusions with such small numbers of patients. The other possible cause of nonunion is excessive soft tissue stripping, which is a pervasive risk factor but appeared difficult to evaluate from the literature review. Fracture fragments with anterior–medial displacement and rotation were commonly observed in HMCF nonunion. To achieve acceptable alignment and reduction, extensive soft tissue stripping is usually necessary to eliminate the scar or fibrotic tissue and bring the fragment into apposition. These procedures may increase the risk of nonunion in these ORIF cases. Some authors have advocated the use of a bone graft or fixation in the functional position rather than the anatomical position. 14,15 However, more cases are required to demonstrate the effectiveness of these techniques. Additionally, ORIF alone may reduce elbow ROM and cannot prevent further irregular articular surface, fishtail deformity, or cubitus varus deformity. The indication of ORIF in this population should be clarified in the future.
Humeral supracondylar osteotomy is an alternative treatment for HMCF nonunion, especially for deformity correction. Our review indicated that all patients who received the osteotomy procedure achieved satisfactory deformity correction without experiencing severe complications. Three cases had poor outcomes after osteotomy due to persistent limited ROM, but none had reduced ROM. As there is no consensus on the most optimal osteotomy procedure option, we performed SDO based on the surgeon’s preference. After the procedure of SDO, although the reported surgical outcome of osteotomy is encouraging, longer term follow-up is need to determine whether post-traumatic osteoarthritis can be avoided after elbow alignment is corrected in these patients.
There are several limitations in this study. Firstly, it was a case series report and literature review only for the cases that involved surgery, which contained original and selection bias. The natural history of HMCF nonunion was not fully elucidated. Secondly, it was difficult to draw any convincing conclusions, given the small sample size (n = 20) and limited information. Thirdly, the duration of postoperative follow-up was relatively short and varied among reports. Our findings should be further validated with larger case cohorts.
In conclusion from the literature review, surgical treatment is effective to reduce the symptoms, correct the deformity, and prevent the late complication of the HMCF nonunion. While ORIF achieved fragment stability and bone union in these cases, it did not resolve residual elbow deformity and ROM limitations. Fair-to-good results can be expected in these patients after osteotomy. We found that humeral supracondylar osteotomy alone effectively corrected varus deformity in HMCF nonunion patients without causing complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.