
Abstract
Background:
Intensive rehabilitation of individuals with bilateral lower limb loss poses a great challenge to both rehabilitation team and amputees themselves due to unavailability of a sound leg to provide stability in standing and gait. Although gait characteristics of individuals with unilateral transtibial amputations are well documented in the literature, very less is known about those with bilateral limb loss.
Aim:
To examine the gait characteristics of an individual with bilateral transtibial amputation (BTA) and its comparison with an able-bodied (AB). This study also provides a real-life presentation of successful prosthetic rehabilitation.
Case content and methodology:
Temporal–spatial, kinematic and kinetic gait parameters were analysed for a 45-year-old male individual with traumatic BTA using prosthesis in a motion analysis laboratory setting with force platform (BTS P-6000) and cameras with reflective markers (BTS SMART-DX6000).
Findings and conclusion:
Variances in many temporal–spatial, kinematic and kinetic parameters were observed. The findings of temporal–spatial parameters revealed that the individual with BTA walked with slower speed, lower cadence, shorter step lengths and wider step width compared to that of AB. Ankle dorsiflexion, stance knee flexion and swing hip hiking were reduced in an individual with BTA compared to AB. In kinetics, he demonstrated low peak ankle muscle power, increased muscle power amplitudes and phase duration at the hip and knee joints compared to AB individual. The combination of an intensive prosthetic rehabilitation led to completely independent and remarkable degree of functional ambulation.
Introduction
Rehabilitation helps the people to regain abilities and maintain independence which is affected in terms of physical, social, psychological and work-related issues. The individuals with bilateral lower limb amputation present with a great challenge for the rehabilitation team to provide a degree of mobility that allows more normal place in society. 1 Compared to unilateral amputees, individuals with bilateral transtibial amputation (BTA) are at a further disadvantage as they lack additional compensatory mechanisms otherwise provided by the sound limb. 2 Primary means of mobility in these individuals is by a wheelchair or a prosthesis. It has been demonstrated that mobility by ambulation with prosthesis profoundly improves the quality of life compared to a wheelchair. 3 However, an earlier study has reported that a high proportion of these individuals eventually abandon their prosthesis in favour of a wheelchair due to high physiological costs of walking. 4 As a consequence, they become increasingly less active and are less likely to lead independent lifestyles. These individuals may continue to do well at a long-time follow-up of rehabilitation and their survival rate improves, therefore they should be given strong consideration for prosthetic fitting. 5 Little evidence exists in relation to prosthetic fitting and gait training of persons with bilateral amputation to guide clinical procedures. 6 Gait of individuals with BTA has been investigated less and is not well understood like their unilateral counterparts. 7 In this study, quantitative gait analysis was performed to characterize the walking pattern of a person with BTA and it was compared with an able-bodied (AB) individual. This article describes about successful rehabilitation of a 45-year-old male individual with BTA who returned to his normal daily life.
Case report
A 45-year-old man (height: 171.5 cm and weight: 65 kg) sustained severe crush injury of both foot and ankle. Subsequently, immediate below knee amputation was performed at 24 h after a thorough debridement and proper patient resuscitation in June 2014 (Figure 1). Split skin graft and reconstruction surgery were performed on July 2014 at SCB Medical College and Hospital, Cuttack, India, for both lower limbs. The idea was to replace it with reasonable and functional prosthetic limbs for a much faster return to work and performing other activities of daily living. He was referred to Swami Vivekanand National Institute of Rehabilitation Training and Research (SVNIRTAR), Cuttack, India, in January 2015 for prosthetic rehabilitation. The aim of rehabilitation was to achieve maximal independence in mobility and self-care activities and to overcome social and vocational problems. This involved full cooperation of all members of the rehabilitation team, including physiatrist, physiotherapists and prosthetists, as well as the well-motivated individual and his family members. Physical examination revealed that he was a well-oriented individual with normal vital signs. His neurological and cardiac examinations were normal. His residual limb length was 15 cm on the left side and 21 cm on the right side from the joint line with no contracture. The incision line was well healed with an adherent scar. General strength was graded 4+ out of 5 in both upper and left lower extremities through manual muscle testing procedure by a trained Physiotherapist. Physiotherapy consisted of strengthening the upper limb and trunk muscles. Stump exercises to strengthen all remaining musculature and to improve range of motion were advised. Balance and transfer training and correct stump bandaging were taught. Prior to prosthetic fitting, both arm-span and hand length were used to estimate the total height of individual (H). Following the principles of body segment parameters, the knee height from floor was estimated to be 0.285 × H. 8

(a) Individual with BTA, (b) individual with a trial endoskeletal prosthesis, (c) complete prosthesis with a cosmetic foam cover, (d) individual standing with final prosthesis (anterior view) and (e) individual standing with a final prosthesis (posterior view). BTA: bilateral transtibial amputation.
He was fitted with definitive endoskeletal prostheses (Figure 1(d) and (e)) after thorough evaluation and assessment. Prosthetic components included patellar tendon-bearing copolymer sockets with ethaflex-made soft inserts, supracondylar cuff suspension straps, ranger foot (solid ankle design) and a pair of shoes (Figure 1(c)). Standing balance and weight transfer exercises were taught inside parallel bars until a satisfactory stability was achieved. Ambulation was initially taught within parallel bars. Four-point gait was first encouraged to generate stability. Progression in ambulation training consisted of transition in use of a walking frame, pair of axillary crutches and canes and at last he achieved independent hand-free mobility. After an extensive gait training programme of 4 weeks, he achieved independent ambulation with both of his hands-free for other activities. He was discharged in April 2015 after final finishing of prosthesis and satisfactory check out procedures. He reported to our institute again in September 2018 after 3 years of successful use of prosthesis. As reported, he has not received any additional rehabilitation in these 3 years. After a thorough inspection of stump and previous prosthesis, it was decided that the replacement of sockets is essential as the number of socks used by him for prosthetic application exceeds the optimal standard of four layers. Within a span of 2 weeks, his sockets were replaced. This time suspension straps were eliminated because of intimate fitting of sockets and liner. Instrumental gait analysis was performed with written informed consent after successful dynamic alignment and final check out.
The force platform (BTS P-6000, BTS Bioengineering Corp., Italy) and six high-definition optoelectronic cameras with reflective markers (BTS SMART-DX 6000, BTS Bioengineering Corp., Italy) were used for kinetic and kinematic data in our gait lab (Figure 2). The sampling rate of force platform was 1000 Hz and the maximum acquisition sampling frequency of the optoelectronic cameras was 2000 fps. A Helen Hayes model was applied concurrently to track the motion of the lower limbs and pelvis through 13 markers placed at different bony landmarks. The obtained data were processed using BTS Smart Analyzer (BTS Bioengineering Corp., Italy). The data were processed using MATLAB (version 9.1), including filtering of marker trajectories with a fourth-order low-pass Butterworth filter. The individual was advised to walk in his self-selected speed over a span of 10 m. He was not aware of location and position of force platform on walking surface. Data were recorded under normal conditions on level surface walking. To compare and analyse the walking pattern, an AB individual (height: 170.7 cm and weight: 64 kg) was selected and his gait analysis was performed following the same protocol. An average of three trials was considered for analysis.

Individual standing in motion analysis laboratory with a force plate and markers placed at different landmarks.
Results
The comparison of temporal–spatial parameters in both individuals is presented in Table 1.
Temporal–spatial parameters.
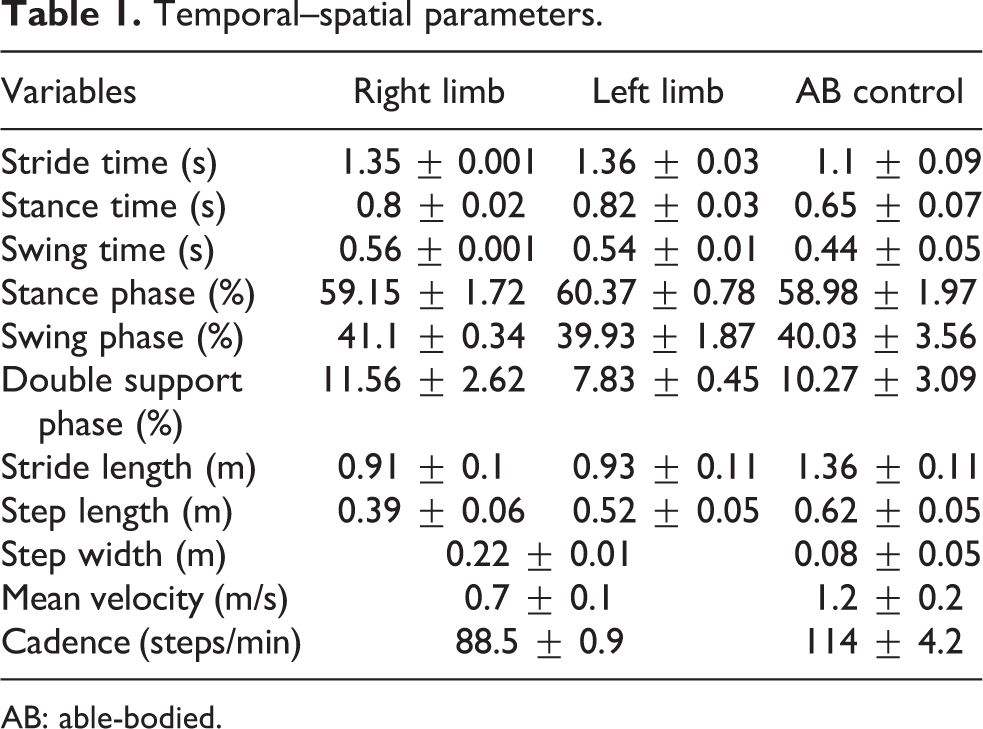
AB: able-bodied.
The kinematic data of major joints of lower limb, for example, hip, knee and ankle, are shown in Figure 3.
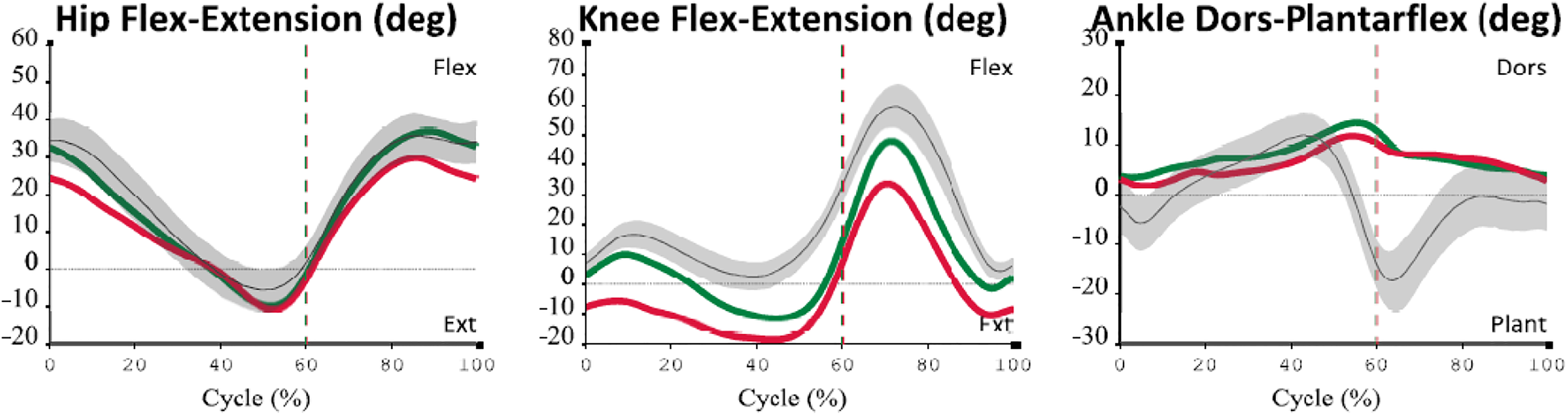
Sagittal plane kinematics of hip, knee and ankle (green line for right limb, red line for left limb and thin black line for AB control). AB: able-bodied.
The kinematics of pelvic motions of left and right limb and its comparison with AB are shown in Figure 4.
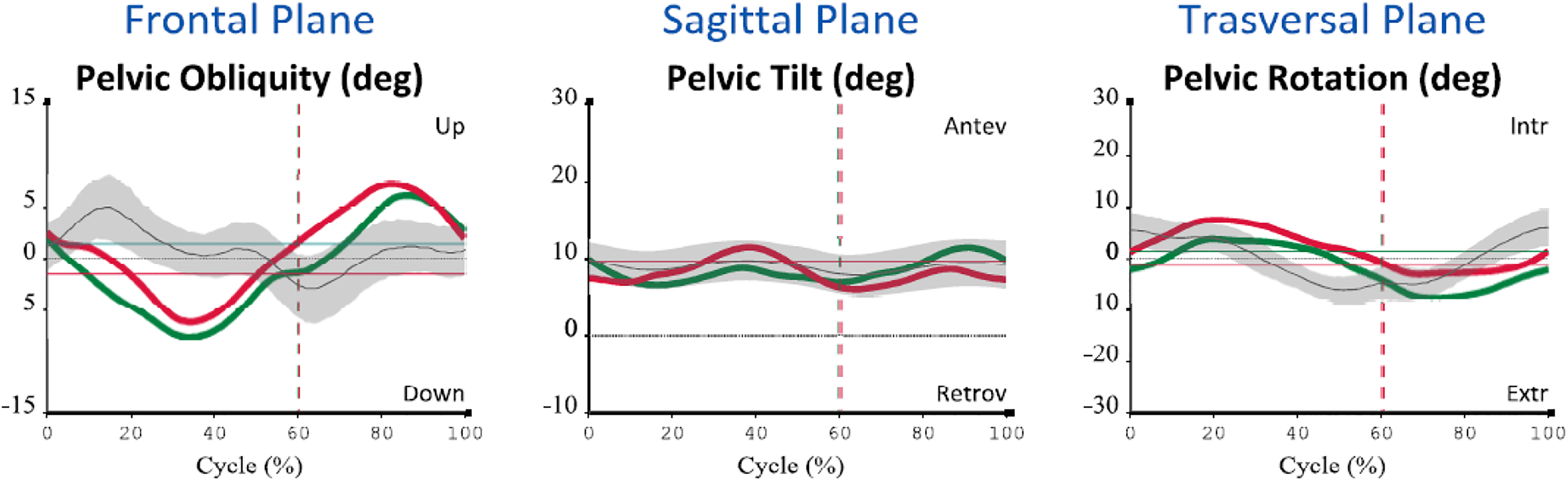
Pelvic motions (green line for right limb, red line for left limb and thin black line for AB control). AB: able-bodied.
In gait kinetics, the different components of ground reaction force (GRF), that is, antero-posterior (AP) and medio-lateral (ML) and vertical and its comparison between individual with BTA and AB control are shown in Figure 5.

GRF during gait (green line for right limb, red line for left limb and thin black line for AB control). GRF: ground reaction force; AB: able-bodied.
The mean pattern of power of lower limb joints for an individual with BTA and AB control is shown in Figure 6.
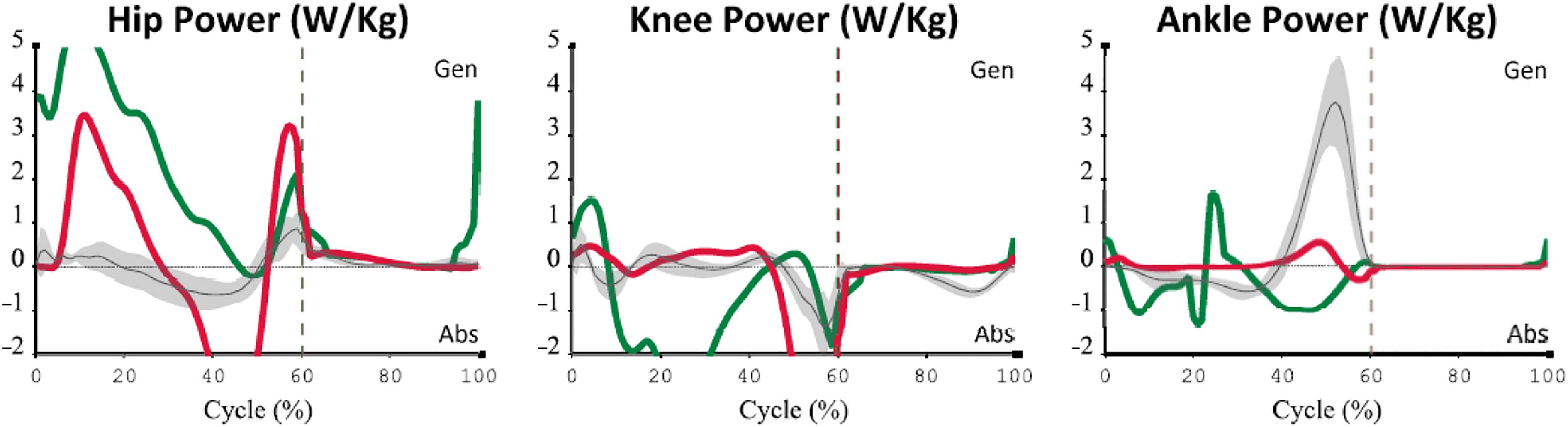
Mean pattern of power of lower limb joints for the individual with BTA and AB control (green line for right limb, red line for left limb and thin black line for AB control). BTA: bilateral transtibial amputation; AB: able-bodied.
The major kinetic data for individual with BTA and AB control are presented in Table 2.
Kinetic data (mean ± standard deviation) for individuals with BTA and AB.
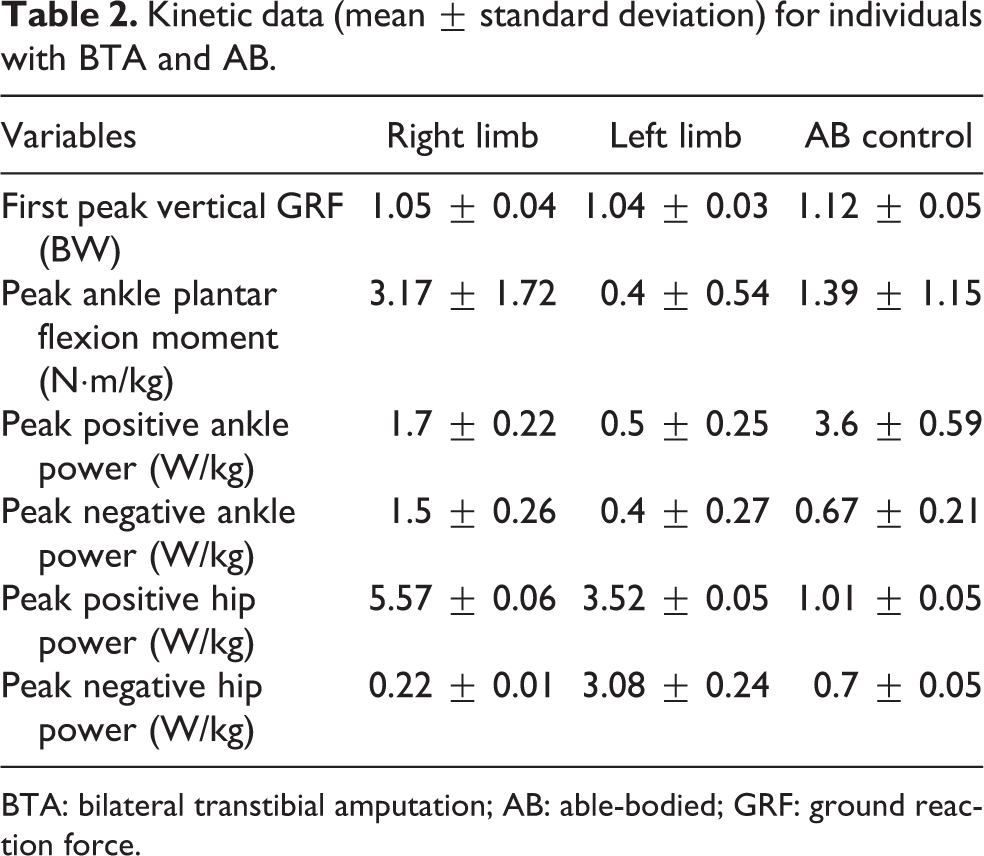
BTA: bilateral transtibial amputation; AB: able-bodied; GRF: ground reaction force.
Discussion
Temporal–spatial parameters
No difference was observed for temporal–spatial parameters like percentage of stance and swing phase. Smaller step length, stride length, cadence and higher step width, stride time, stance time and swing time were observed for either limb of the individual compared to AB. His self-selected speed was 0.7 m/s compared to 1.2 m/s for the AB individual. Therefore, he walked at 58.33% of speed adopted by the AB individual. The reason for the obtained result is due to the fact that, after BTA, the individual lacked dynamic balance and walked with greater lateral trunk motion and adopted an increased step width to enhance stability. Su et al. 9 examined differences in gait characteristics between persons with BTA of trauma and vascular cause and compared it with data from AB. The authors found similar results. A wider base of support in the individual indicates that his balance may have been compromised due to poor proprioception and perception of stability. There is almost no difference between the performance of right and left limb of the individual in terms of temporal–spatial gait parameters. However, compared to the left limb which is shorter, the right limb achieved greater step and stride length. This may be due to an individual’s ability to bear weight on the right limb (longer in length) and progress his left limb with more stability and comfort.
Gait kinematics
The peak-to-peak hip and knee flexion and extension in stance phase did not differ significantly between BTA and AB individual (Figure 3) and followed similar curves. The maximum knee flexion achieved during push off was 45° compared to 60° in AB. Ankle joint dorsiflexion and plantar flexion range varied significantly due to the presence of Ranger foot (a sold ankle design) in BTA. Comparing both limbs, it was observed that the left limb produced lesser range of flexion–extension for hip and knee joints.
The Ranger foot (solid ankle cushion heel type) used in this study has excellent stability and cosmetic appearance. Studies have shown that most bilateral lower limb amputees can perform extracurricular recreational activities with conventional prostheses. 1 Plantar flexion is simulated by compression of the heel cushion but ankle dorsiflexion is not available. This is the reason why a flatter curve was obtained in ankle kinematics of both limbs for the individual. Although inversion and eversion are absent, forces in the coronal plane are dampened by compression of the rubber sole. Hyperextension of toes is simulated by the flexible toe portion distal to the end of the internal keel. Although studies on comparison between SACH and energy-conserving foot in bilateral amputees are scarce, previous studies on unilateral transtibial amputees have generally reported no significant differences between these two in terms of cadence, step length, walking speed and inconsistent effect on first peak of vertical GRF. 10 An increase in the magnitude of both positive and negative ankle joint power was observed with SACH feet and these results are in accordance with earlier researches. 10 However, the use of energy-conserving foot with increased prosthetic ankle motion may improve some gait parameters of persons with BTAs.
The variance in pelvic motion patterns (pelvic obliquity, tilt and rotation) and magnitudes was observed between two individuals (Figure 4). The individual with BTA raised the pelvis on the side of the trailing leg during the loading response phase instead of letting it drop, as observed in the AB. Consequently, the shock absorbed during gait may have been substantially reduced in individual with BTA as a result of reduced stance-phase knee flexion and an abnormal pattern of pelvic obliquity. Similar results were obtained by earlier researchers. 11
Gait kinetics
Individual with BTA displayed a smaller second peak of vertical GRF compared to AB during self-selected walking speed (Figure 5). The first peak of vertical GRF was similar in both lower limbs of the subject with trans-tibial amputation. The same peak was also noticed for AB individual. The AP and ML shear components of GRF did not reach the peaks and followed asymmetrical curves compared to AB individual.
Joint moments and power generation
The ankle, knee and hip moments and their peak magnitudes differed between both individuals. An individual with BTA demonstrated a greater ankle dorsiflexion and plantar flexion moment than the AB. Although the pattern followed by knee and hip moment generation was similar in both individuals, the peaks were higher for individual with BTA which produced gait asymmetry. With an aim to identify a relationship between torque values, symmetry of muscle torque of hip flexors and extensors and a degree of gait asymmetry in patients with lower limb amputation, Kucharska et al. observed significant correlation between hip joint extensors and gait asymmetry as found in this study too. 12
Although three-dimensional data have been used to describe the gait of individuals, only muscle powers developed in the sagittal plane were used to assess below-knee amputee locomotion. 13 As expected, a low peak ankle muscle power was observed for both lower limbs caused by a slight deformation capability of the prosthetic foot compared to AB. In a similar study, Sadeghi et al. studying muscle power compensatory mechanism of transtibial amputees using SACH foot found similar results. 14 By virtue of compensating loss of normal ankle muscle power functions, muscle power amplitudes and phase duration at the hip and knee joints were increased. Hip muscle power peaks showed greater activity on the individual with BTA than AB especially during loading response (Figure 6). However, the variance was observed in power generation of both lower limb joints for individual with BTA (Table 2).
The phases of rehabilitation for individual with BTA typically progressed from pre-prosthetic therapy to prosthetic fitting and training and then to gradual mobility training. Advancement was made from standing to level ground walking, ramps and stairs, obstacle negotiation and, finally, sports and recreational activities with successful results. A home visit was carried out prior to discharge to ensure total independence within the home. Assessing the need for any structural alteration, the supply of equipment, family’s acceptance of the individual and his ability to manage a wheelchair or prostheses in his home environment was checked. Suitable accommodation and social support play an important part in the success or failure of rehabilitation and getting the final degree of independence achieved. The individual was leading a normal life with full independency in functional daily living activities (Figure 7).

Different day to day activities. (a) Pumping water from bore well, (b) taking drinking water to his home, (c) cutting wood for use as fuel, (d) driving motorcycle for marketing and (e) recreational activities.
Most of the individual’s functional activities require good range of pelvic, hip, knee and ankle motions. Except for the limitation of ankle dorsiflexion range in the prosthetic foot, the prosthesis does not hinder the motions of other joint motions. Although temporal–spatial gait parameters were altered to achieve stability and comfort with the cost of loss of both limbs, these are essential requirements for activities of daily living. AB individual with intact muscles produced active plantar flexion to provide push off and generate significant power for forward progression. Push off impairment and compensation with symmetric single-stance hip work appear sufficient to explain many asymmetries commonly observed in the gait of bilateral lower limb amputees. Weak prosthetic-side push off leads to a large collision on the intact leg, followed by lower stance-phase speed and higher stance duration. To compensate for the lost push off work (in order to maintain average speed), work output is increased in both legs during stance phases. Prosthetic foot and ankle components that allow for greater sagittal and transverse plane rotations provide substantial benefit during walking and should be considered for individuals with BTA. 10 Apart from these clinically established parameters, functional training was given as a part of rehabilitation that helps with the acquisition of special abilities or the attainment of some forms of manipulative skills in the use of equipment for daily activities. These should conform to recognized therapeutic procedures like strength, balance, coordination and endurance.
Conclusion
Careful evaluation by a multidisciplinary team is the key for right treatment decision and successful rehabilitation of individual with BTA. A remarkable degree of functional ambulation was achieved by applying proper surgical, therapeutic, prosthetic and other rehabilitation techniques at the appropriate time. Large variances in many of the temporal–spatial parameters like smaller step length, stride length, cadence and higher step width, stride time, stance time and kinematic data (e.g. ankle dorsi–plantar flexion) was observed for either limb of the individual compared to AB. Therefore, it can be concluded that the BTA gait is complex and varied. Further research investigating the physiological energy expenditure, psychological factors and their interplay that may affect walking performance is encouraged to gain a better understanding of the gait abnormalities in these individuals.
Footnotes
Acknowledgements
The authors would like to thank our individual for his sincerity and cooperation throughout this case study. The authors would also like to thank Dr P.P. Mohanty, HOD, Department of Physiotherapy for giving permission and Mr Kiran Kumar Subudhi, MPT student for taking data in the gait lab.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.